Ilizarov External Fixation for Tibial Shaft Fractures: Surgical Guide
Key Takeaway
The Ilizarov external fixator is a highly versatile device for managing complex tibial shaft fractures. By utilizing tensioned fine wires and circular rings, it provides optimal biomechanical stability while allowing axial micromotion to promote secondary bone healing. This guide details the step-by-step surgical technique, including frame assembly, safe-zone wire insertion, multi-planar fracture reduction, and postoperative management to minimize complications such as pin track infections and neurovascular injury.
Comprehensive Introduction and Patho-Epidemiology
The management of complex, comminuted, or open tibial shaft fractures presents a formidable challenge to the orthopedic surgeon. The anterior medial border of the tibia is notoriously devoid of robust muscular coverage, rendering the diaphyseal bone highly susceptible to high-energy trauma, severe soft tissue compromise, and open fractures. Traditional methods of internal fixation, such as rigid plating or intramedullary nailing, while highly effective for closed or lower-energy injuries, can catastrophically compromise the already tenuous periosteal and endosteal blood supply in severe Gustilo-Anderson Type IIIB and IIIC injuries. The Ilizarov external fixation system, pioneered by Professor Gavriil Abramovich Ilizarov in Kurgan, Russia, revolutionized the treatment of these devastating injuries by introducing the biological concept of the tension-stress effect.
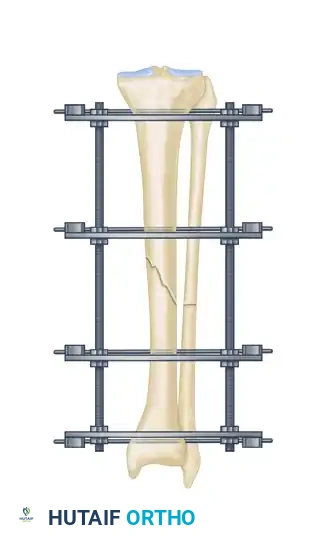
Unlike rigid internal fixation modalities that rely on absolute stability and primary bone healing, the Ilizarov circular frame utilizes tensioned fine wires to provide exceptional shear and torsional stability while deliberately permitting controlled axial micromotion. This unique biomechanical environment stimulates robust secondary bone healing via endochondral ossification (callus formation) without the need for any soft tissue stripping at the fracture site. By spanning the zone of injury and anchoring into healthy proximal and distal metaphyseal or diaphyseal bone, the circular fixator preserves the fracture hematoma, respects the biological envelope, and allows for simultaneous management of complex soft tissue defects, including the application of local or free flaps.
The epidemiology of tibial shaft fractures necessitating circular external fixation is heavily skewed toward high-energy mechanisms, including motor vehicle collisions, motorcycle accidents, industrial crush injuries, and ballistic trauma. These mechanisms frequently impart massive kinetic energy to the limb, resulting in multi-fragmentary fracture patterns, segmental bone loss, and severe periosteal stripping. In this context, the Ilizarov method is not merely a fracture stabilization tool; it is a comprehensive limb salvage strategy. The modularity of the frame allows for the simultaneous or staged treatment of concomitant pathologies, such as acute shortening for soft tissue closure followed by distraction osteogenesis, or the treatment of established infected nonunions via bone transport.
This comprehensive guide details the surgical technique for applying an Ilizarov external fixator to tibial shaft fractures, expanding upon foundational operative principles to provide a masterclass in frame assembly, multi-planar fracture reduction, safe-zone wire insertion, and the meticulous management of postoperative complications. Mastery of this technique requires a profound understanding of cross-sectional anatomy, biomechanical principles, and the biological imperatives of bone healing under tension.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the cross-sectional anatomy of the lower extremity is the absolute prerequisite for the safe and effective application of an Ilizarov frame. The leg is divided into four distinct fascial compartments: anterior, lateral, superficial posterior, and deep posterior. Each compartment houses critical neurovascular structures that must be meticulously avoided during the insertion of transfixation wires. The "safe corridors" for wire insertion vary significantly depending on the axial level of the tibia. Proximal to the tibial tuberosity, the safe zone is relatively wide, allowing for a broad angle of wire crossing. However, as one progresses distally into the diaphysis, the safe zones narrow considerably due to the proximity of the anterior tibial artery and deep peroneal nerve anteriorly, and the posterior tibial artery and tibial nerve posteriorly.
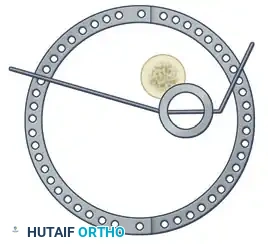
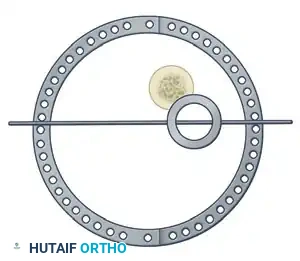
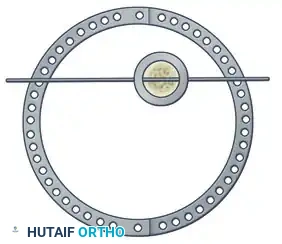
The biomechanical efficacy of the Ilizarov circular frame relies on the precise geometric arrangement of rings and the high-tensioning of fine wires. Standard fine wires, typically 1.5 mm or 1.8 mm in diameter, are inherently flexible and offer minimal structural support in their resting state. However, when tensioned to 110–130 kg using a dedicated dynamometric tensioner, these filaments are transformed into highly rigid beams capable of supporting physiological loads. This tensioning process is the biomechanical heart of the Ilizarov system. The wires act like the spokes of a bicycle wheel, centralizing the bone within the ring and resisting translational and bending forces.
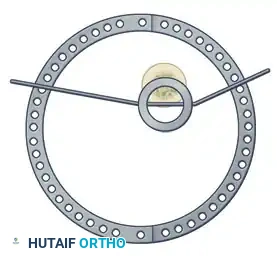
Construct stiffness is dictated by several highly modifiable variables. The diameter of the rings is inversely proportional to the stability of the construct; therefore, the surgeon must select the smallest ring diameter that still safely accommodates postoperative soft tissue edema (the "two-fingerbreadth rule"). The crossing angle of the wires is equally critical. While a 90-degree crossing angle provides optimal orthogonal stability, anatomical safe zones rarely permit this ideal configuration in the tibial diaphysis. Consequently, surgeons must often accept crossing angles of 45 to 60 degrees, compensating for the loss of orthogonal stability by adding a third wire, utilizing drop wires, or incorporating half-pins (hybrid fixation) to increase the stiffness of the block.
Furthermore, the distance between the rings and the fracture site significantly impacts the biomechanical environment. Rings placed closer to the fracture site increase the bending stiffness of the construct, while rings placed further away increase flexibility. The Ilizarov system's unique ability to decouple axial stiffness from torsional and shear stiffness allows the surgeon to create a custom biomechanical environment tailored to the specific fracture morphology. The controlled axial micromotion permitted by the tensioned wires under physiological weight-bearing is the primary mechanical stimulus for the differentiation of mesenchymal stem cells into osteoblasts, driving the robust callus formation characteristic of the tension-stress effect.
Exhaustive Indications and Contraindications
The decision to utilize an Ilizarov circular frame for a tibial shaft fracture requires a nuanced evaluation of the fracture personality, the soft tissue envelope, and the patient's physiological and psychological capacity to tolerate the device. While intramedullary nailing remains the gold standard for most closed diaphyseal tibial fractures, the Ilizarov method excels in scenarios where internal fixation is either biologically contraindicated or biomechanically insufficient. The primary indication is the management of severe open fractures (Gustilo-Anderson Types IIIB and IIIC) where massive soft tissue degloving or contamination precludes the safe insertion of hardware into the medullary canal or against the periosteal surface.
Beyond acute trauma, the Ilizarov frame is the definitive treatment modality for complex nonunions, particularly those complicated by active osteomyelitis (infected nonunions). The ability to aggressively debride necrotic, infected bone and subsequently reconstruct the resulting defect via distraction osteogenesis (bone transport) is a unique capability of circular external fixation. Additionally, the frame is highly indicated for periarticular fractures that extend into the diaphysis, where the small proximal or distal bone segments provide inadequate purchase for traditional plates or nails.
Contraindications to the Ilizarov method are primarily related to patient compliance and severe systemic illness. The success of circular fixation relies heavily on the patient's ability to participate in rigorous daily pin site care, aggressive physical therapy, and, in cases of bone transport, the meticulous execution of daily frame adjustments. Patients with profound cognitive impairment, severe psychiatric disorders, or active substance abuse are generally poor candidates, as non-compliance can lead to catastrophic complications, including deep pin tract infections, joint contractures, and premature consolidation or nonunion.
| Category | Specific Condition | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Infected Tibial Nonunion | Allows for radical debridement of dead bone and sequential bone transport without introducing internal hardware. |
| Absolute Indications | Gustilo IIIB/IIIC Open Fractures | Spans the zone of injury, preserves vascularity, and allows unhindered access for plastic surgery soft tissue coverage. |
| Absolute Indications | Segmental Bone Loss | Facilitates acute shortening followed by lengthening, or classic bifocal/trifocal bone transport. |
| Relative Indications | Periarticular Fractures with Diaphyseal Extension | Fine wires can capture extremely small, osteopenic periarticular fragments that would not hold a screw. |
| Relative Indications | Severe Closed Fractures with Soft Tissue Compromise | Avoids a "second hit" to the soft tissue envelope (e.g., Tscherne C2/C3 closed injuries). |
| Relative Contraindications | Non-compliant Patient | High risk of pin site infection, contractures, and failure to perform required frame adjustments. |
| Relative Contraindications | Severe Peripheral Vascular Disease | Poor healing potential for pin sites; high risk of ischemic necrosis at wire insertion points. |
| Absolute Contraindications | Lack of Surgical Expertise | The learning curve is steep; improper application leads to severe neurovascular injury and deformity. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for Ilizarov external fixation is an exacting process that dictates the success of the intraoperative execution. Standard orthogonal radiographs (anteroposterior and lateral) of the entire tibia, including the knee and ankle joints, are mandatory. However, axial computed tomography (CT) scans with coronal and sagittal reconstructions are highly recommended, particularly for high-energy injuries. CT imaging delineates complex fracture morphology, identifies occult comminution or longitudinal split fractures that might propagate during wire insertion, and helps determine the optimal trajectory for multi-planar reduction wires.
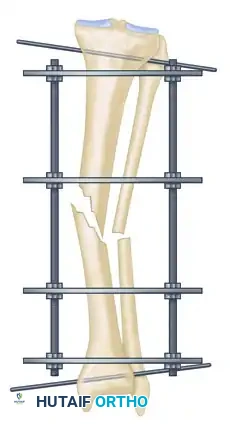
Sizing the frame preoperatively is a critical step. The diameter of the rings must be carefully selected to balance biomechanical stability with soft tissue clearance. The surgeon should measure the circumference of the patient's calf at its widest point and select a ring size that provides a minimum of two fingerbreadths (approximately 2 to 3 cm) of clearance circumferentially. This clearance is vital to accommodate the inevitable postoperative edema; failure to account for this will result in severe skin impingement, focal necrosis, and early frame failure. The frame is typically preassembled in the sterile processing department or on the back table prior to the induction of anesthesia, consisting of a proximal block (usually two rings) and a distal block (two rings), connected by threaded rods.
Optimal patient positioning is the first critical intraoperative step in ensuring a smooth surgical workflow and accurate frame application. The patient is placed supine on a radiolucent table or a specialized table extension. This setup is non-negotiable, as it allows for unimpeded, high-quality fluoroscopic imaging in both the AP and lateral planes without interference from the table's metal chassis. A bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, bringing the patella to a strict anterior facing position.
Longitudinal traction is frequently employed to restore limb length and gross alignment before frame application. This can be achieved using a dedicated fracture table with a calcaneal traction pin, or manually by an assistant. In many cases, the external fixator itself can be used as a traction device once the proximal and distal reference wires are secured. Longitudinal traction typically reduces most tibial shaft fractures to within 10 to 15 degrees of anatomical alignment. However, surgeons must be acutely aware of the dangers of over-distraction. Excessive or prolonged traction places undue tension on the neurovascular bundles, significantly increasing the risk of iatrogenic neurapraxia (particularly of the common peroneal nerve) or vascular compromise, and creates a distraction gap that will reliably lead to nonunion if not addressed.
Step-by-Step Surgical Approach and Fixation Technique
Frame Preparation and Initial Placement
The meticulous application of the preassembled Ilizarov frame begins with the preparation of the surgical field. After standard orthopedic skin preparation and draping, the preassembled frame must be opened to be placed around the limb. Disconnect the ring connection bolts on one side of the frame, allowing it to hinge open. Carefully pass the opened frame around the injured extremity, ensuring that the assistant maintains longitudinal traction and gross alignment of the fracture.
Once the limb is encompassed, reassemble the frame and tighten the connection bolts. At this stage, the surgeon must verify the soft tissue clearance circumferentially. Ensure the 2 to 3 cm clearance rule is respected, paying particular attention to the posterior calf, which is highly prone to dependent edema. The frame must then be aligned so that the longitudinal coupling bolts (threaded rods) are parallel to the anterior crest of the tibia in both the AP and lateral fluoroscopic planes. This parallel alignment is crucial, as it ensures that any subsequent lengthening or compression maneuvers occur along the true anatomical axis of the bone.

Reference Wire Placement and Frame Suspension
To establish the foundational alignment of the construct, proximal and distal reference wires must be placed with absolute precision. Hold the frame in the desired position, ensuring it is orthogonal to the mechanical axis of the tibia. Insert a proximal transverse reference wire through the safe zone of the proximal metaphysis, ensuring it is perfectly parallel to the knee joint line. Subsequently, insert a distal transverse reference wire parallel to the ankle joint line (tibial plafond).
As these reference wires are secured to the rings using wire fixation bolts and tensioned to 130 kg, the frame becomes a rigid template. Because the wires are parallel to the joints, and the frame is orthogonal to the wires, tensioning these reference wires forces the bone segments to align with the frame, thereby achieving initial correction of the fracture in the coronal plane.

If manual holding of the heavy frame is difficult during this initial stage, an alternative suspension technique can be employed. Suspend the frame using ordinary surgical suction tubing. Place the tubing around the extremity and secure it to the proximal and distal rings with towel clips. Eccentrically tilt the proximal and distal rings until they are perfectly parallel to the knee and ankle joints, respectively. After securing fixation with at least two tensioned wires to both the proximal and distal rings, adjust the longitudinal threaded rods to bring these two rings parallel to their counterparts in the center of the frame. This maneuver utilizes the frame's geometry to facilitate powerful indirect fracture reduction.
Multi-Planar Fracture Reduction Using Olive Wires
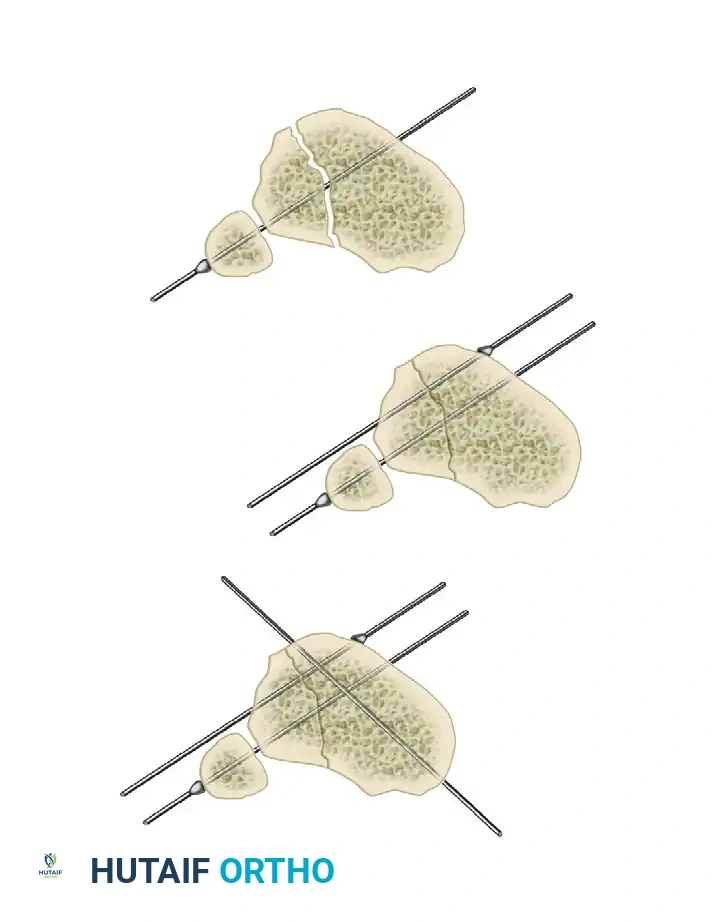
Olive wires—fine wires equipped with a small, forged metal bead or "olive" near the center—are the most powerful tools in the Ilizarov armamentarium for translating bone fragments and achieving precise, multi-planar final reduction. They act as intra-osseous joists, allowing the surgeon to pull a specific bone fragment in a desired direction.
For coronal plane correction, identify the residual displacement on the AP fluoroscopic view. Insert an arched olive wire in a transverse fashion through the displaced fragment, ensuring the trajectory remains strictly within the anatomical safe zone. The olive must be positioned on the side of the bone opposite to the direction of desired translation.
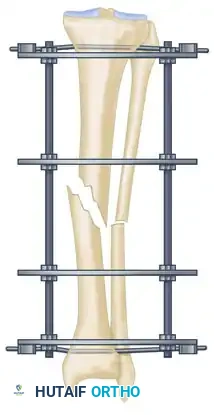
Secure the plain end of the wire to the tensioner on the ring. Apply tension to the wire without securing it tightly to the frame on the olive side. As the tensioner operates, it will pull the wire, causing the olive to engage the near cortex and drag the bone fragment toward the tensioner, effectively correcting the translation. Continuous image intensification is mandatory during this step to ensure adequate reduction is achieved without over-translating the fragment.
Once the anatomical axis is restored in the coronal plane, secure the wire to the frame on the olive side using a slotted fixation bolt, locking the reduction in place.
If further correction is required in the sagittal plane (e.g., correcting an apex anterior or posterior angulation/translation), a similar technique is employed. Connect another olive wire in an arched fashion, oriented to address the sagittal deformity. Tensioning this arched wire will impart a directional force vector to the bone, pulling it into precise sagittal alignment.

Eliminating Residual Distraction and Specific Fracture Patterns
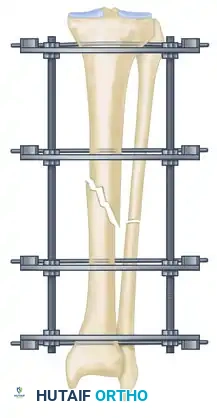
Following successful multi-planar correction using olive wires, the surgeon must critically assess the fracture site on fluoroscopy for any residual longitudinal distraction. Even a few millimeters of distraction gap at the diaphyseal fracture site will severely inhibit secondary bone healing and reliably lead to an atrophic nonunion. To resolve this, systematically adjust the nuts on the longitudinal threaded rods connecting the proximal and distal blocks. Shortening the distance between the blocks will compress the fracture site, eliminating any residual distraction and optimizing the environment for osteogenesis.
In specific clinical scenarios involving long oblique or spiral fracture patterns, a specialized technique utilizing opposing olive wires can be employed. Two olive wires are inserted from opposite sides of the limb, passing perpendicular to the plane of the fracture. As these wires are simultaneously tensioned, the opposing olives squeeze the fracture fragments together, effecting reduction and applying robust interfragmentary compression.
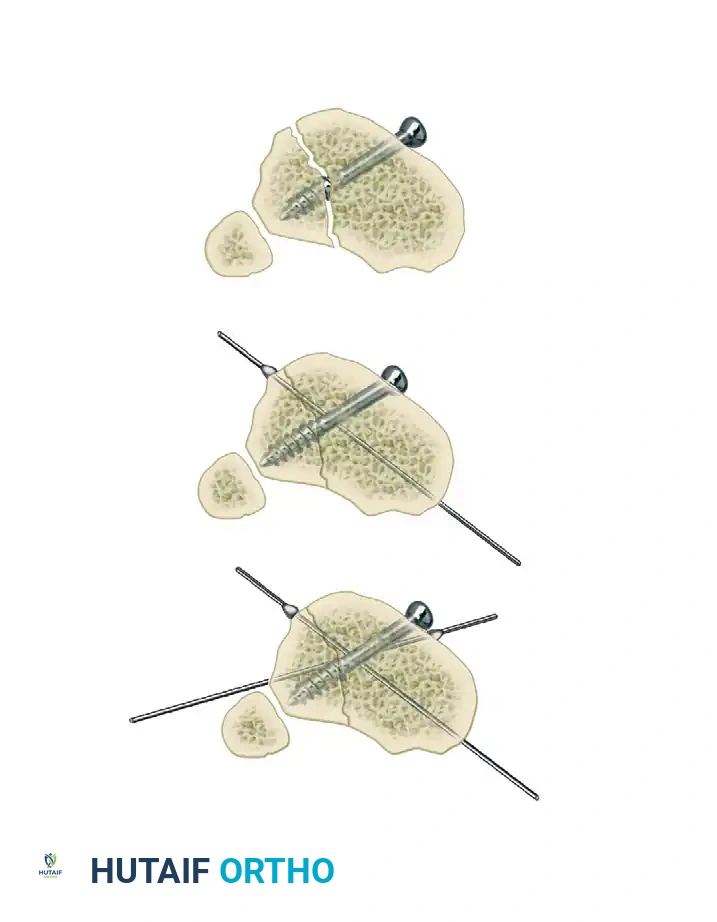
While opposing olive wires provide excellent compression, this pattern of wire placement may not always be anatomically safe due to the location of the neurovascular bundles. If safe corridors are unavailable, these specific metaphyseal or highly stable diaphyseal fracture patterns may occasionally be fixed with one or more independent lag screws, followed by the application of the Ilizarov frame to neutralize bending and torsional forces. However, extreme caution is advised: rigid interfragmentary screws negate the axial flexibility of the circular frame, which is the primary driver of secondary osteogenesis. This hybrid technique should be strictly reserved for highly specific configurations and is generally discouraged for primary diaphyseal healing.
Safe Transfixation Wire Insertion Protocol
The insertion of fine transfixation wires must be executed with meticulous care to avoid thermal necrosis of the cortical bone and catastrophic injury to the surrounding soft tissues. Thermal necrosis leads to ring sequestrum formation, premature pin loosening, and deep pin tract infections.
First, appropriate wire selection is necessary. In general, 1.5-mm and 1.8-mm smooth wires require no skin incision or drill sheath. They can be passed directly. If larger 2.0-mm wires or half-pins are utilized, a small stab incision, blunt dissection to the bone, and the use of a protective drill sheath are mandatory. When handling the wire, sterile glove paper or an alcohol swab can be used to grasp the wire close to the insertion site, providing the surgeon with increased control and preventing the flexible wire from wandering off the curved cortical surface of the tibia.
Predrilling is not required for fine wire insertion. The surgeon must determine the safe angle for transfixation at the specific anatomical level, constantly referencing mental or physical cross-sectional anatomy atlases. Stab the wire directly through the skin and muscle down to the bone. Use a low-speed power drill, employing frequent pauses, or a hand drill, to advance the wire across both the near and far cortices. High-speed drilling generates excessive friction and heat, which is the primary enemy of stable external fixation.
Crucially, the moment the wire tip emerges from the far cortex, drilling must immediately cease. The surgeon should then tap the wire through the remaining soft tissues on the exit side using a mallet. This blunt passage technique significantly reduces the risk of the spinning wire wrapping, entangling, or lacerating the deep neurovascular structures. Once passed, attach the wires to the rings without bending them to meet the frame. Bending wires introduces asymmetric tension and profoundly weakens the structural integrity of the construct. If a wire does not sit flush against the ring, use small washers or spacers to build the connecting bolts off the frame to meet the wire in its natural trajectory. Finally, ensure there is no undue pressure on the pin-skin interface; release any tethered skin with a small scalpel incision (#11 blade) to prevent focal ischemia and necrosis.
Complications, Incidence Rates, and Salvage Management
The application and maintenance of an Ilizarov frame is an intensive process, and complications are not merely possible; they are expected. The surgeon's role is to proactively manage these issues before they compromise the ultimate goal of limb salvage and fracture union. Complications can be broadly categorized into pin-related, neurovascular, mechanical, and biological issues.
Pin track infection is the most ubiquitous complication, occurring in up to 80% of patients at some point during their treatment course. Most of these are superficial (Checketts-burns Grades 1-3) and respond rapidly to local wound care and short courses of oral antibiotics (e.g., cephalexin or clindamycin). However, deep infections involving the bone (Grades 4-6) require aggressive intervention. A loose wire must be suspected at the first sign of localized pain, erythema, and purulent discharge. If a wire is loose, it has lost its tension and is no longer contributing to frame stability; it must be removed or exchanged immediately to prevent the development of ring sequestrum and chronic osteomyelitis.
Neurovascular injuries, while less common (incidence of 2-5%), are potentially devastating. Acute nerve injury is usually the result of direct penetration or thermal damage during wire insertion. If a patient reports unusually severe, radiating pain along the distribution of a specific nerve immediately postoperatively, an offending wire must be suspected of impinging upon the nerve and should be removed without hesitation. Late neurovascular complications can occur during bone transport due to the stretching of structures, requiring a temporary halt to the distraction process.
Joint contractures are a frequent and highly problematic complication, particularly equinus contractures of the ankle and flexion contractures of the knee. The transfixation of muscles and fascia by the wires tethers the musculotendinous units, limiting their excursion. Prevention is the only effective management strategy. Immediate, aggressive active and passive range-of-motion exercises must be instituted on postoperative day one. Dynamic splinting may be added to the frame if contractures begin to develop.
Severe soft tissue impingement due to postoperative edema is a mechanical complication that requires structural modification of the frame. If severe skin impingement occurs early in the treatment course, the frame must be expanded. For major, circumferential impingement at multiple levels, a larger frame must be constructed around the original frame. The rings of the new, larger frame are positioned at exactly the same axial levels. The curled ends of the existing wires are straightened, and the wires are connected to the new, larger frame using slotted threaded rods or extension plates, after which the original, impinging inner rings are carefully dismantled and removed.
| Complication Type | Estimated Incidence | Prevention and Salvage Management Strategies |
|---|---|---|
| Superficial Pin Tract Infection | 60% - 80% | Prevention: Meticulous insertion technique; daily pin care with chlorhexidine/soap. Management: Oral antibiotics, increased frequency of local care. |
| Deep Pin Tract Infection / Osteomyelitis | 3% - 5% | Prevention: Avoid thermal necrosis (low-speed drilling). Management: Immediate wire removal, over-drilling of the pin tract, IV antibiotics. |
| Joint Contracture (Ankle Equinus) | 15% - 25% | Prevention: Early aggressive PT, avoiding transfixation of the Achilles tendon. Management: Add a foot ring to the frame, Achilles lengthening (rare). |
| Neurovascular Injury | 2% - 5% | Prevention: Strict adherence to anatomical safe zones; blunt passage of wires through soft tissue. Management: Immediate removal of offending wire; surgical exploration if vascular compromise is evident. |
| Delayed Union / Nonunion | 5% - 10% | Prevention: Eliminate distraction gaps intraoperatively; encourage early weight-bearing. Management: Frame dynamization, injection of orthobiologics (BMAC), or frame modification to increase axial micromotion. |
Phased Post-Operative Rehabilitation Protocols
The surgical application of the Ilizarov frame is only the first phase of treatment; the ultimate success of the procedure relies heavily on a rigorous, phased postoperative rehabilitation protocol. Unlike internal fixation, where the hardware is hidden, the external fixator requires active daily participation from the patient and the physical therapy team.
Immediate Post-Operative Phase (Weeks 0-2)
In the immediate postoperative period, the primary goals are pain control, edema management, and the initiation of early mobility. The limb should be elevated above the level of the heart to combat dependent edema, which can rapidly lead to soft tissue impingement against the rings. Pin site care typically begins on postoperative day 2 or 3. The wire-skin interfaces should be cleaned daily with mild soap and water or a dilute chlorhexidine solution. Gentle pressure dressings using sterile sponges or gauze are applied around the pin sites; this is critical to prevent pistoning motion between the pin and the skin, which is the primary catalyst for irritation and subsequent infection. Active range of motion of the knee and ankle is initiated immediately to prevent the tethered muscles from developing fibrotic contractures.
Intermediate Phase and Weight-Bearing Progression (Weeks 2-8)
As the acute postoperative pain subsides, the focus shifts to maximizing weight-bearing. Early weight-bearing in the frame is highly encouraged and is a fundamental tenet of the Ilizarov method. Axial loading of the limb transfers forces through the tensioned wires, creating the controlled axial micromotion at the fracture site that is biologically essential for the differentiation of callus. Patients are typically progressed from touch-down weight-bearing to partial, and eventually full weight-bearing as tolerated. During this phase, patients are permitted to take normal showers, as the mechanical flushing of water is beneficial for pin site hygiene. Swimming in chlorinated pools is also permissible, provided it is immediately followed by a clear water rinse and thorough drying of the pin sites.
Late Phase, Frame Removal, and Post-Removal Care
The late phase involves monitoring for clinical and radiographic signs of union. Radiographic evaluation of callus formation in the presence of a circular frame can be challenging due to the radiopacity of the rings and wires. Therefore, clinical assessment is paramount. Once bridging callus is seen on three out of four cortices on orthogonal radiographs, the frame can be "dynamized." This involves selectively loosening or removing the longitudinal threaded rods to transfer more physiological load directly to the healing bone, testing its structural integrity. If the patient can ambulate without pain following dynamization, the fracture is deemed clinically united. Frame removal is typically performed in the clinic under oral analgesia or light sedation. Following removal, the limb is temporarily protected in a patellar tendon bearing (PTB) cast or a functional fracture brace for 4 to 6 weeks to protect the newly formed bone and allow the pin tracts to fully ossify, preventing late-onset stress fractures through the pin holes.
Summary of Landmark Literature and Clinical Guidelines
The clinical application of the Ilizarov method is supported by decades of robust
