Intramedullary Nailing in Reconstruction Mode: Surgical Guide
Key Takeaway
Intramedullary nailing in reconstruction mode is a highly effective surgical technique for managing complex subtrochanteric femoral fractures. By utilizing cephalomedullary screws directed into the femoral head, this construct neutralizes extreme biomechanical deforming forces. This guide details precise patient positioning, entry portal establishment, anatomical reduction techniques, and sequential reaming to prevent varus malalignment and ensure optimal postoperative outcomes for orthopedic patients.
Comprehensive Introduction and Patho-Epidemiology
Subtrochanteric femoral fractures represent one of the most formidable and technically demanding challenges in the realm of orthopedic trauma surgery. Defined anatomically as fractures occurring within the zone extending from the lesser trochanter to approximately five centimeters distally into the proximal femoral diaphysis, these injuries disrupt the critical transitional zone between the proximal metaphyseal bone and the diaphyseal cortical bone. The epidemiology of subtrochanteric fractures classically exhibits a bimodal distribution. In the younger demographic, these fractures are typically the sequelae of high-energy trauma, such as motor vehicle collisions or falls from significant heights, often presenting with severe comminution, extensive soft tissue compromise, and concomitant polytrauma. Conversely, in the geriatric population, these fractures frequently result from low-energy mechanisms, such as simple falls from a standing height, and are intimately associated with osteopenia, osteoporosis, and structurally compromised bone architecture.
In recent decades, a distinct third epidemiological category has emerged: the atypical femur fracture (AFF). Chronic suppression of bone turnover, most notably through the prolonged administration of bisphosphonates or denosumab, has been definitively linked to the development of these unique subtrochanteric and diaphyseal fractures. Pathognomonically, AFFs present with localized lateral cortical thickening (beaking), a transverse or short oblique fracture line originating at the lateral cortex, and a distinct lack of comminution. The profoundly suppressed osteoclastic activity in these patients severely impairs targeted bone remodeling, leading to the accumulation of microdamage and eventual catastrophic failure under physiological loads. Managing these atypical fractures requires a nuanced understanding of their distinct biology, as they exhibit notoriously high rates of delayed union and nonunion, often necessitating specialized intramedullary nailing techniques and prolonged postoperative surveillance.
The historical evolution of subtrochanteric fracture management reflects a continuous pursuit of biomechanical optimization. Early operative interventions heavily relied upon extramedullary devices, such as the 95-degree angled blade plate or dynamic condylar screws. While these devices provided rigid fixed-angle constructs, their application required extensive open surgical exposures, profound periosteal stripping, and significant disruption of the fracture hematoma, culminating in unacceptable rates of infection, nonunion, and catastrophic hardware failure. The paradigm shifted dramatically with the advent of intramedullary nailing. By functioning as load-sharing rather than load-bearing devices, intramedullary nails significantly decrease the bending moment across the fracture site due to their closer proximity to the mechanical axis of the lower extremity.
To specifically address the extreme biomechanical demands of the subtrochanteric region, the concept of "reconstruction mode" nailing was developed. Unlike standard antegrade nailing, which utilizes transverse or oblique locking screws directed into the lesser trochanter or proximal diaphysis, reconstruction mode employs two robust cephalomedullary screws directed proximally into the dense cancellous bone of the femoral head and neck. This sophisticated construct effectively bypasses the severely compromised and mechanically disadvantaged subtrochanteric zone, providing unparalleled biomechanical stability against the relentless varus-producing forces inherent to the proximal femur.
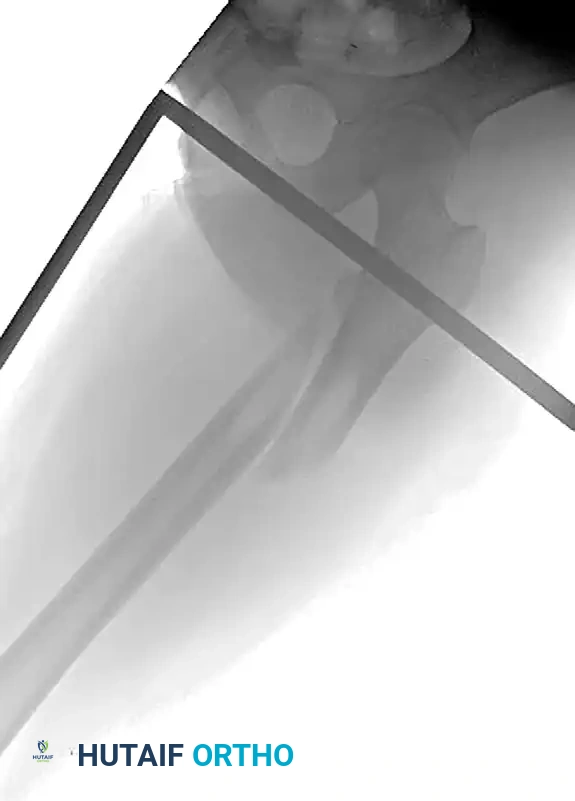
Preoperative radiograph demonstrating a displaced subtrochanteric femoral fracture with characteristic proximal fragment abduction and flexion.

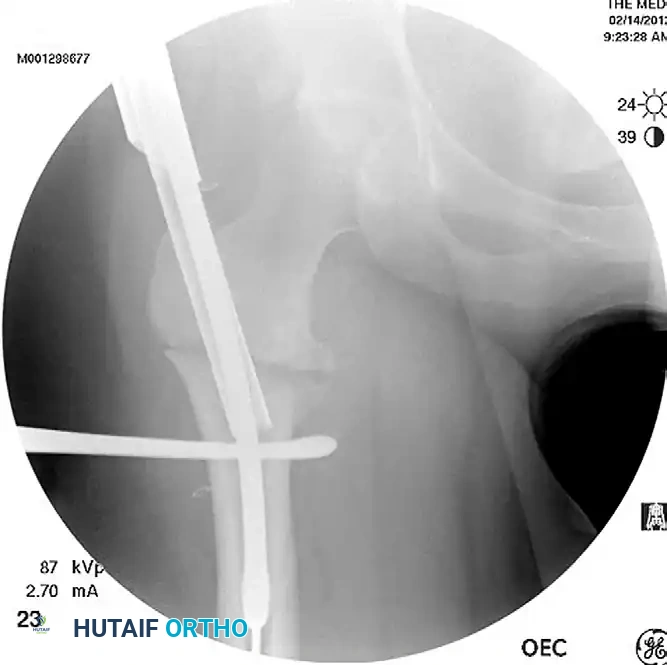
Postoperative anteroposterior radiograph following successful fixation with an antegrade intramedullary nail locked in reconstruction mode.

Postoperative lateral radiograph confirming central placement of the cephalomedullary screws within the femoral head.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and the complex biomechanical milieu of the proximal femur is the absolute prerequisite for successful subtrochanteric fracture management. The subtrochanteric region is subjected to the highest biomechanical stresses in the human skeleton. During normal physiological loading, such as the single-leg stance phase of the gait cycle, the medial cortex of the subtrochanteric femur is subjected to massive compressive forces that can routinely exceed 1,200 pounds per square inch. Simultaneously, the lateral cortex is subjected to significant tensile forces. This extreme mechanical environment dictates that any surgical construct must possess exceptional fatigue strength to withstand cyclical loading until robust osseous union is achieved.
The defining and most problematic characteristic of a subtrochanteric fracture is the profound, predictable, and multi-planar deformity of the proximal fragment, driven by the unopposed action of powerful pelvic and thigh musculature. The proximal segment is aggressively pulled into profound flexion by the iliopsoas muscle, which inserts directly onto the lesser trochanter. Simultaneously, the robust abductor musculature—specifically the gluteus medius and gluteus minimus, inserting onto the greater trochanter—forces the proximal fragment into severe abduction. Furthermore, the short external rotators (piriformis, superior and inferior gemelli, obturator internus and externus, and quadratus femoris) exert a powerful external rotation torque.
Conversely, the distal diaphyseal segment is subjected to an entirely different set of deforming forces. The massive adductor complex (adductor longus, brevis, and magnus), originating from the pubis and ischium and inserting along the linea aspera, forcefully pulls the distal segment into adduction. Concurrently, the powerful longitudinal pull of the quadriceps and hamstring muscle groups results in significant proximal migration and overall limb shortening. The net result is a classic "flexed, abducted, and externally rotated" proximal fragment paired with an "adducted and shortened" distal fragment. This extreme malalignment creates a catastrophic varus and apex-anterior angulation at the fracture site, which, if not meticulously corrected prior to intramedullary reaming, will result in an irreversible iatrogenic malunion.
From a vascular perspective, the subtrochanteric region is a critical watershed area. The profound femoral artery, via its perforating branches, supplies the robust muscular envelope and the periosteal blood supply to the diaphyseal femur. However, the proximal femur and the femoral head rely heavily on the medial femoral circumflex artery (MFCA) and its ascending cervical branches. When utilizing a piriformis fossa or greater trochanteric entry portal for intramedullary nailing, the surgeon must maintain a profound respect for the terminal branches of the MFCA. Overzealous reaming, aggressive retractor placement, or catastrophic iatrogenic fracture of the femoral neck during reconstruction screw placement can compromise this tenuous blood supply, precipitating devastating avascular necrosis (AVN) of the femoral head.
Exhaustive Indications and Contraindications
The decision to proceed with intramedullary nailing in reconstruction mode requires a meticulous evaluation of the patient's physiological status, the specific fracture morphology, and the integrity of the proximal femoral bone stock. While intramedullary nailing remains the undisputed gold standard for the vast majority of subtrochanteric fractures, specific clinical scenarios dictate alternative approaches. The utilization of reconstruction mode is specifically indicated when standard transverse proximal locking would fail to provide adequate biomechanical stability, or when the fracture line extends proximally into the intertrochanteric or basicervical region.
A critical indication for reconstruction nailing is the presence of a combined, ipsilateral femoral neck and subtrochanteric (or diaphyseal) fracture. In these complex scenarios, standard antegrade nailing is strictly contraindicated, as it fails to address the femoral neck fracture and may cause catastrophic displacement during nail insertion. Reconstruction nailing allows for simultaneous, rigid fixation of both the diaphyseal/subtrochanteric component and the femoral neck component through a single load-sharing device. Furthermore, impending or completed pathologic fractures secondary to metastatic disease are prime indications for reconstruction nailing. The cephalomedullary screws provide secure anchorage in the uninvolved femoral head, bypassing the structurally compromised subtrochanteric metastatic lesion and allowing for immediate weight-bearing and pain palliation.
Contraindications to intramedullary nailing must be strictly observed to prevent catastrophic complications. Active soft tissue or osseous infection at the surgical site is an absolute contraindication, as the introduction of a massive intramedullary device will inevitably disseminate the infection throughout the entire femoral canal, leading to intractable pan-osteomyelitis. Severe physiological instability in a polytraumatized patient (the "in extremis" patient) may necessitate temporary damage-control external fixation rather than definitive intramedullary nailing. Relative contraindications include profound obliteration of the medullary canal (e.g., severe Paget's disease or prior intramedullary osteomyelitis), which may preclude the passage of intramedullary reamers and nails.
| Category | Intramedullary Nailing in Reconstruction Mode |
|---|---|
| Absolute Indications | Displaced subtrochanteric fractures (Russell-Taylor Types IA, IB, IIA) |
| Ipsilateral femoral neck and subtrochanteric/shaft fractures | |
| Impending or completed pathologic subtrochanteric fractures | |
| Atypical femur fractures (AFFs) with subtrochanteric extension | |
| Relative Indications | Subtrochanteric nonunions (often requiring concurrent bone grafting) |
| Osteoporotic fractures requiring enhanced proximal fixation | |
| Absolute Contraindications | Active deep infection or pan-osteomyelitis of the femur |
| Obliterated medullary canal precluding reamer passage | |
| Extreme pre-existing deformity precluding straight nail insertion | |
| Relative Contraindications | Severe comminution of the greater trochanter/piriformis fossa (entry portal compromise) |
| Polytrauma patients requiring damage-control orthopedics (DCO) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous, exhaustive preoperative planning is non-negotiable in the management of subtrochanteric fractures. The surgeon must thoroughly evaluate high-quality, orthogonal radiographs of the entire femur, including dedicated anteroposterior (AP) and cross-table lateral views of the hip, as well as AP and lateral views of the knee. The integrity of the greater trochanter and the piriformis fossa must be scrutinized, as severe comminution in these regions will obliterate the starting portal, rendering intramedullary nailing technically prohibitive and necessitating alternative fixation strategies, such as plate osteosynthesis.
Digital or acetate templating is a mandatory step to determine the optimal nail diameter, overall nail length, and the precise angle of the cephalomedullary reconstruction screws (typically 125, 130, or 135 degrees). The nail diameter should be templated at the narrowest portion of the medullary canal (the isthmus) on both the AP and lateral views. The length of the nail should be measured from the tip of the greater trochanter to the level of the physeal scar in the distal femur. Crucially, the surgeon must template the trajectory of the reconstruction screws to ensure they can be centrally placed within the femoral neck and head without breaching the superior, inferior, anterior, or posterior cortices.
Patient positioning is a critical determinant of surgical success. The patient is typically placed supine on a specialized radiolucent fracture table, though the lateral decubitus position on a flat, radiolucent table is an acceptable alternative based on surgeon preference and experience. When utilizing a fracture table, the injured extremity is secured in longitudinal traction through either a skeletal traction pin placed in the distal femur or proximal tibia, or via a specialized traction boot. A well-padded perineal post is positioned to provide counter-traction, taking extreme care to avoid pudendal nerve compression.
A vital positioning maneuver is the flexion of the injured hip to approximately 30 to 40 degrees. This specific degree of flexion is not arbitrary; it is a calculated biomechanical intervention designed to relax the tension on the iliopsoas muscle. By neutralizing the profound deforming flexion force exerted by the iliopsoas on the lesser trochanter, the proximal fragment naturally drops posteriorly, facilitating anatomical alignment with the distal diaphyseal segment. Accurate restoration of femoral version is equally paramount to prevent devastating postoperative gait abnormalities. The gold standard for determining correct version is contralateral templating. The surgeon obtains a true lateral fluoroscopic image of the uninjured hip and knee, calculates the inherent patient-specific anteversion, and then precisely matches this rotational profile on the injured side by externally rotating the distal fragment through the traction apparatus.
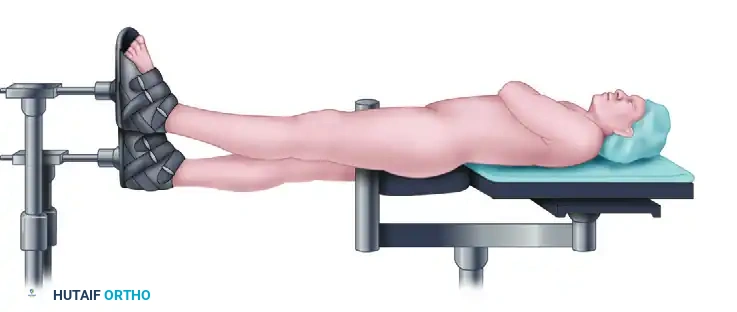
Patient positioned supine on the fracture table with the injured extremity in traction and the hip flexed to neutralize deforming forces.
Step-by-Step Surgical Approach and Fixation Technique
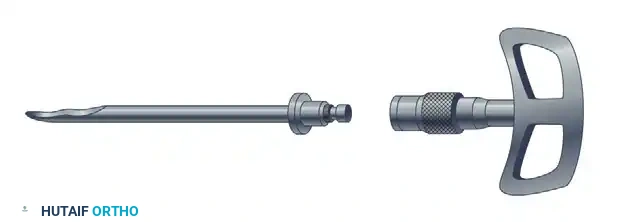
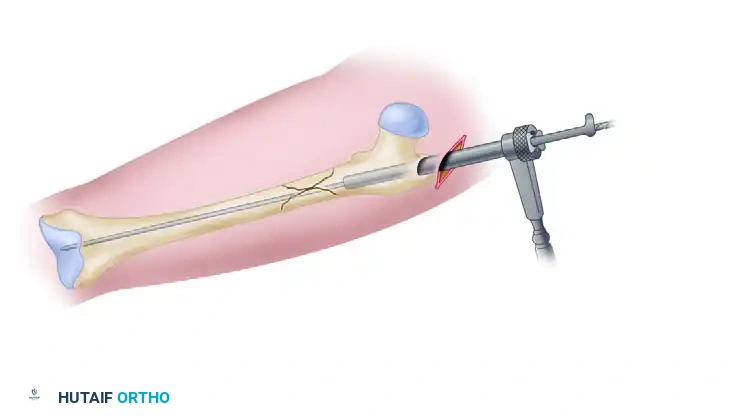
Incision and Entry Portal Establishment
The establishment of an anatomically perfect entry portal is the most critical step in subtrochanteric nailing; a millimeter of deviation at the entry site translates to degrees of catastrophic malalignment at the fracture site. Make a longitudinal incision beginning approximately 3 to 5 centimeters proximal to the tip of the greater trochanter, extending proximally in line with the coarse fibers of the gluteus maximus. Bluntly dissect through the gluteal fascia and split the muscle fibers to expose the proximal femur.
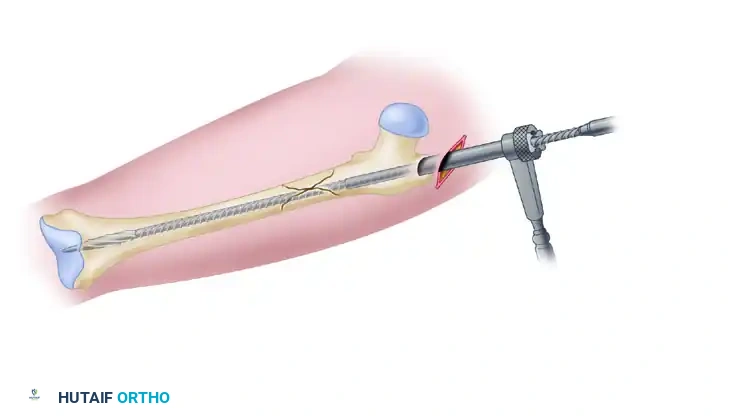
Small incision beginning proximal to the greater trochanter, allowing access for the entry reamer.
The selection of the entry portal is strictly dictated by the specific design of the intramedullary nail being utilized. For a trochanteric entry nail, the guide pin is placed slightly medial to the exact tip of the greater trochanter on the AP view, and perfectly centered on the lateral view. For a piriformis fossa entry nail, the starting point is further medial, directly in line with the central axis of the femoral canal.
However, when utilizing a piriformis entry nail in reconstruction mode, a critical surgical modification is required. The guide pin must be intentionally "cheated" approximately 5 millimeters anteriorly on the true lateral fluoroscopic view. This deliberate anterior offset is absolutely mandatory. If the nail is placed perfectly central in the piriformis fossa on the lateral view, the subsequent trajectory of the two cephalomedullary reconstruction screws will be directed far too posteriorly, inevitably impinging upon or breaching the posterior cortex of the femoral neck. By starting slightly anteriorly, the nail is positioned to allow the reconstruction screws to pass perfectly through the central axis of the femoral neck.

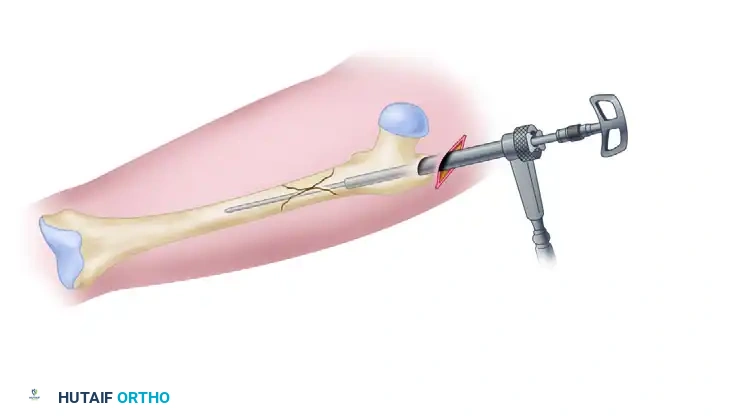
Establishment of the precise entry portal using a guide pin under fluoroscopic guidance.
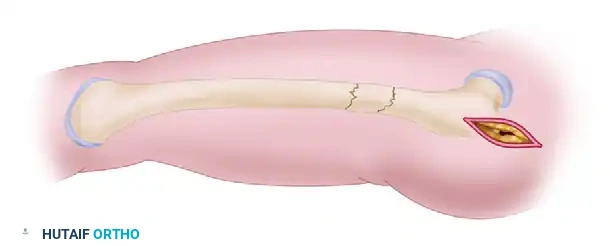
Anatomical Reduction of the Proximal Segment
The most fundamental axiom of subtrochanteric nailing is this: Never ream an unreduced subtrochanteric fracture. Reaming a malaligned femur will inevitably create an eccentric, erroneous medullary track. Once this false track is established, the insertion of the rigid intramedullary nail will permanently lock the fracture into a varus, flexed, or externally rotated malunion.
The surgeon must aggressively correct the typical flexion, abduction, and external rotation deformities of the proximal segment before passing the entry reamer. This is frequently accomplished through percutaneous or mini-open techniques. A combination of a ball spike pusher and a Cobb elevator can be introduced through a small anterior or lateral stab incision to manually depress the flexed and abducted proximal fragment. The surgeon physically pushes the proximal fragment down and medial to align it with the distal shaft.
If manual pressure with simple elevators is insufficient to overcome the massive muscular forces, the surgeon must not hesitate to enlarge the lateral incision (which will conveniently be used later for the insertion of the reconstruction screws). Through this expanded approach, a large, aggressive bone-holding forceps, such as a Jungbluth or Farabeuf clamp, is introduced to physically grasp and manipulate the proximal segment into anatomical alignment. If the fracture pattern is highly unstable and the reduction is lost upon clamp removal, the surgeon should pass a percutaneous cerclage wire or cable around the fracture site to rigidly hold the anatomical reduction during the subsequent reaming process.
Utilization of a dedicated reduction tool to manipulate the proximal fragment and align the medullary canal.
Achieving and maintaining anatomical fracture reduction prior to the passage of the guide rod.
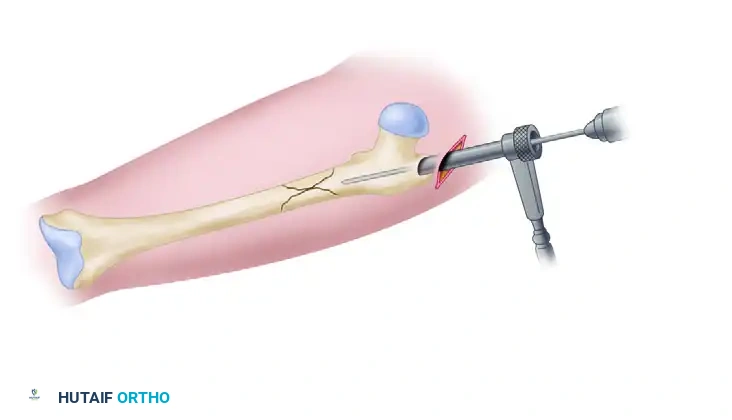
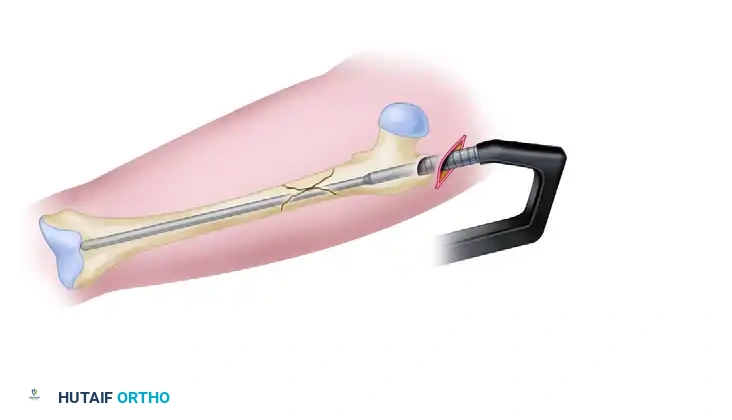
Trajectory Control and Proximal Reaming
A common and devastating technical error in subtrochanteric nailing is the inadvertent selection of a starting portal that is too lateral on the greater trochanter. A lateral starting point forces the rigid entry reamer, and subsequently the nail, to enter the medullary canal at an oblique angle. As the nail is advanced, it inevitably impinges on the medial cortex of the distal segment, physically pushing the distal segment medially and resulting in a severe, iatrogenic varus malalignment.
To ensure absolute "Trajectory Control," the surgeon must utilize a combination entry reamer or channel reamer to open the proximal femur. During the introduction of the entry reamer, the surgeon must maintain strict, deliberate medial pressure on the instrument handle. This medial pressure counteracts the tendency of the reamer to skid laterally off the hard cortical bone of the trochanter, thereby avoiding eccentric lateral reaming and preventing catastrophic lateral wall blowout.
Trajectory control: Establishment of a precise, slightly medial entry portal to prevent varus deviation.
Protection of the entry portal by reaming directly through the established channel, avoiding lateral wall blowout.
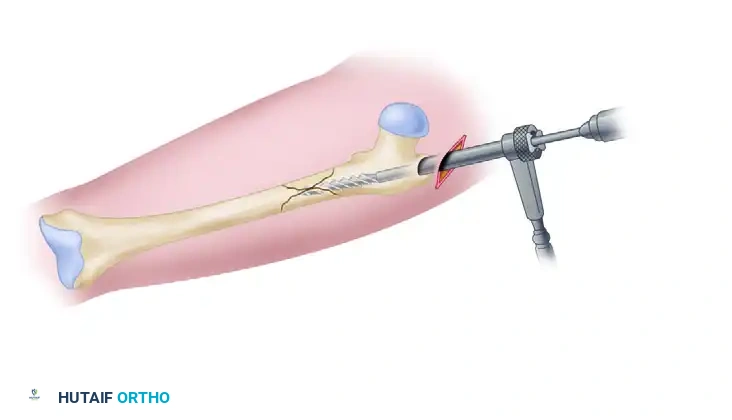
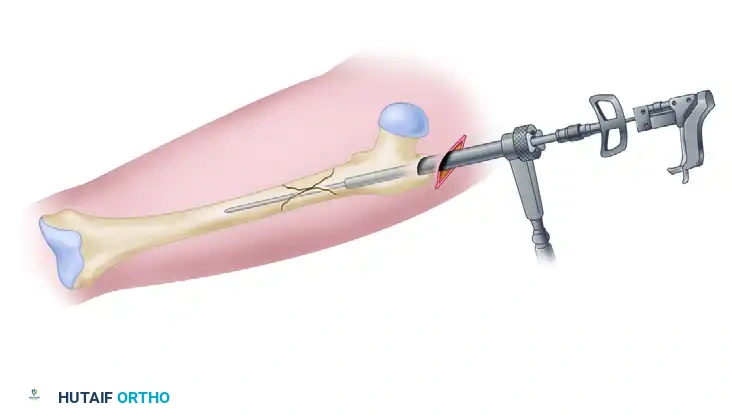
Introduction of the combination entry reamer/channel reamer into the proximal femur.
Proximal reaming completed, establishing a centralized track for the intramedullary nail.
Canal Preparation and Nail Insertion
Once the proximal segment is meticulously prepared and the fracture is rigidly held in anatomic reduction, the medullary canal is prepared for nail insertion. A long, ball-tipped guide rod is introduced through the proximal portal, carefully navigated across the anatomically reduced fracture site, and advanced centrally down the diaphyseal canal until it reaches the level of the physeal scar in the distal femur.
With the guide rod securely in place, the surgeon measures the required length of the intramedullary nail using a radiolucent ruler or a dedicated depth gauge placed over the guide rod. The measurement is taken from the anticipated proximal end of the nail (flush with or slightly recessed below the tip of the greater trochanter) to the distal tip of the guide rod. Following accurate measurement, the femoral shaft is sequentially reamed. Reaming is typically performed in 0.5-millimeter increments through the proximal channel reamer protector. The surgeon advances the reamers until distinct "cortical chatter" is felt and heard, indicating contact with the dense diaphyseal cortical bone. The canal must be over-reamed by 1.0 to 1.5 millimeters larger than the selected nail diameter to ensure smooth, unhindered nail insertion and to prevent iatrogenic hoop stress fractures. Finally, the appropriate-size intramedullary nail is manually inserted over the guide rod.
Insertion of the ball-tipped guide rod across the anatomically reduced fracture site.
Measurement for the precise length of the intramedullary nail using a radiolucent ruler or depth gauge.
Sequential reaming of the femoral shaft over the ball-tipped guide rod.
Placement of the intramedullary nail, advanced to the appropriate depth for proximal reconstruction locking.
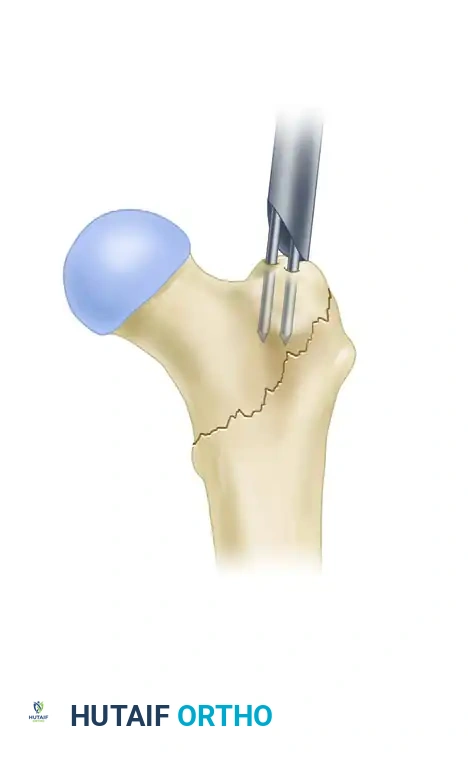
Proximal Locking in Reconstruction Mode
Locking the intramedullary nail proximally in reconstruction mode requires absolute precision to ensure that both cephalomedullary screws are entirely contained within the femoral neck and head, without breaching the cortices. The reconstruction targeting guide is securely attached to the proximal end of the nail. The surgeon must meticulously adjust the version of the nail by rotating the insertion handle until the targeting guide is perfectly aligned with the central axis of the femoral neck on the true lateral fluoroscopic view.
A critical technical pearl is to drill the distal screw hole first. The hole for the most inferior of the two cephalomedullary screws is drilled, aiming to position this screw so that it rests just superior to the dense cortical bone of the calcar femorale (the calcar buttress). This inferior positioning provides optimal biomechanical support against varus collapse. Crucially, the surgeon must leave the distal drill bit in place and not remove it. Leaving the rigid drill bit engaged in the femoral head provides immense rotational stability to the entire nail-bone construct, preventing the nail from inadvertently rotating while the proximal hole is drilled.
The hole for the proximal screw is then drilled. The screws are inserted sequentially: the distal cephalomedullary screw is inserted first to firmly establish the critical calcar support, followed by the proximal screw. Exhaustive fluoroscopic confirmation is mandatory; the surgeon must verify on multiple views, especially the true lateral, that both screws are perfectly centered within the femoral head and neck and have not violated the joint space.
Distal Locking and Rotational Assessment
The final stage of fixation involves locking the nail distally to control length and rotation. Distal locking is routinely performed using a standard free-hand fluoroscopic technique, commonly referred to as the "perfect circles" method. The C-arm is meticulously adjusted until the distal locking holes of the intramedullary nail appear as perfectly round circles on the monitor, indicating that the fluoroscopic beam is perfectly collinear with the axis of the holes. A sharp trocar or drill is then advanced precisely through the center of these circles to engage the far cortex.
Before the surgical drapes are removed, the surgeon must rigorously and exhaustively check for any iatrogenic external or internal rotational malalignment of the entire lower extremity. The leg is carefully removed from the traction apparatus. The surgeon moves the injured hip through a full, unrestricted range of motion, specifically assessing internal and external rotation with the hip and knee flexed to 90 degrees. This rotational arc is meticulously compared to the documented rotational arc of the contralateral, uninjured side. If a significant, clinically unacceptable side-to-side discrepancy exists (typically greater than 10 to 15 degrees), the surgeon must not hesitate to remove the distal interlocking screws, manually correct the rotation of the distal femur to match the contralateral side, and re-drill and re-lock the nail distally.
Complications, Incidence Rates, and Salvage Management
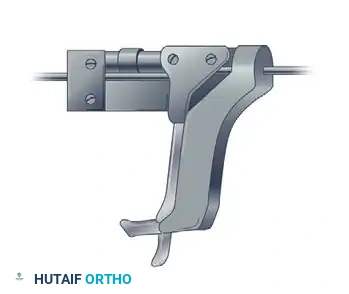
Despite meticulous preoperative planning and exacting surgical technique, subtrochanteric nailing remains fraught with potential complications. The most prevalent and biomechanically devastating complication is varus malreduction. This typically occurs due to a failure to adequately counteract the massive abductor forces on the proximal fragment, or from the inadvertent creation of a lateralized entry portal. Varus malalignment profoundly increases the bending moment on the intramedullary nail, exponentially increasing the risk of delayed union, nonunion, and catastrophic hardware fatigue failure.
If a suboptimal, lateralized entry portal is inadvertently created during the initial approach, the surgeon must immediately recognize the error and employ definitive salvage techniques before proceeding with reaming. The most powerful and elegant salvage option is the Poller (Blocking) Screw Technique. The surgeon places a rigid, anterior-to-posterior interlocking screw (the Poller screw) in the proximal fragment, positioned intentionally medial to the desired, correct nail track. This blocking screw acts as an artificial, unyielding medial cortex. As the reamer, and subsequently the nail, is advanced, it impacts the Poller screw and is physically deflected laterally, forcing the instrument into the correct trajectory and effectively correcting the var
Clinical & Radiographic Imaging Archive