Dynamic External Fixation of PIP Joint Fracture-Dislocations: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through dynamic external fixation for proximal interphalangeal (PIP) joint fracture-dislocations. We meticulously cover surgical anatomy, preoperative planning, and granular, real-time intraoperative execution, including precise K-wire placement and bending techniques. Emphasis is placed on preventing complications, ensuring joint stability, and guiding postoperative rehabilitation for optimal functional recovery.
Welcome, fellows, to the operating theater. Today, we are addressing one of the most notoriously challenging yet frequently encountered injuries in hand trauma: the proximal interphalangeal (PIP) joint fracture-dislocation. The procedure we will master today—dynamic external fixation—is an incredibly powerful tool in our surgical armamentarium. It is explicitly designed to restore articular stability while simultaneously promoting the early active motion that is absolutely paramount for optimizing functional outcomes in the hand. Observe closely, ask probing questions, and let us delve deeply into the physiological rationale, anatomical foundations, and technical intricacies of this elegant technique.
Comprehensive Introduction and Patho-Epidemiology
The proximal interphalangeal joint is the functional epicenter of the digital ray, accounting for approximately 85% of the total arc of motion required for a functional power grasp and fine pinch kinematics. Consequently, any disruption to its congruent articular surface or supporting ligamentous envelope can lead to devastating stiffness, chronic pain, and profound functional impairment. PIP joint fracture-dislocations typically arise from high-energy axial loading combined with a hyperextension or hyperflexion vector, generating catastrophic shear and compressive forces across the delicate articular cartilage and subchondral bone.
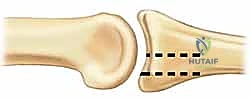
Pilon fractures of the PIP joint, as we frequently encounter them in both athletic and occupational settings, represent severe compression injuries primarily affecting the base of the middle phalanx. Less commonly, these axial crush vectors can involve the distal phalanx or the proximal phalanx of the thumb. These fractures are pathognomonically characterized by a central articular depression and a splaying of the volar and dorsal articular margins. This "die-punch" phenomenon is a direct testament to the immense axial loading force that drives the rigid, bicondylar head of the proximal phalanx deep into the relatively softer, highly cancellous metaphyseal bone of the middle phalanx base. The resulting impaction destroys the native subchondral architecture, rendering simple screw fixation biomechanically impossible.

Injuries to the PIP joint can be broadly categorized based on the specific articular surface that fails under load. Convex-side injuries involve the distal condylar end of the proximal phalanx. These are typically less complex, often presenting as discrete two-fragment shear injuries (e.g., unicondylar or bicondylar fractures), and are generally highly amenable to standard open reduction and internal fixation (ORIF) techniques utilizing mini-fragment screws when surgical intervention is warranted. Conversely, concave-side injuries involve the base of the middle phalanx and are frequently highly comminuted. They present clinically either as discrete fracture-subluxations, outright dislocations, or the devastating pilon fracture pattern we just discussed.
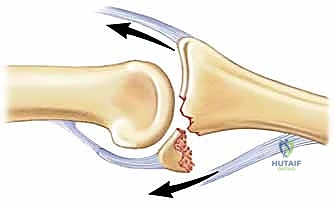
Fracture-subluxations and complete dislocations most commonly involve a dorsal displacement of the primary dorsal fragment of the middle phalanx, leaving a comminuted volar lip fragment tethered to the volar plate. While less common, we also encounter volar and lateral subluxations and dislocations, which carry their own unique challenges regarding central slip avulsions and collateral ligament ruptures. The direction of the displacement is dictated entirely by the vector of the deforming force and the specific sequence of ligamentous failure.


These injuries typically result from a longitudinal, end-on force crushing the middle phalanx base. This mechanism is ubiquitous in sports like cricket, basketball, or baseball, or simply from an uncoordinated fall onto an outstretched digit. Longitudinal fracture extension, sometimes reaching down the majority of the middle phalanx diaphyseal length, can also be associated with these high-energy injuries, further complicating the potential for internal fixation. The propagation of these fracture lines dictates the boundaries of our safe zones for pin placement during external fixation.


Detailed Surgical Anatomy and Biomechanics
To effectively reconstruct the PIP joint, one must possess an intimate understanding of the critical anatomy that governs its inherent stability. The joint is a classic ginglymus (hinge) joint, but with subtle, unforgiving complexities. The distal end of the proximal phalanx presents a convex surface composed of two distinct asymmetric condyles separated by an intercondylar notch. This geometry articulates precisely with the biconcave surface of the proximal end of the middle phalanx, which features a median ridge that tracks within the proximal intercondylar notch, providing intrinsic bony stability against radioulnar translation.

However, the primary stability of this joint relies heavily on its robust ligamentous restraints. The volar plate is a thick, dense fibrocartilaginous structure that is tethered to the proximal phalanx proximally via the checkrein ligaments and inserts broadly and firmly into the volar base of the middle phalanx distally. Its integrity is paramount for preventing dorsal subluxation and hyperextension. The collateral ligaments—comprising the proper collateral ligament (PCL) and the accessory collateral ligament (ACL)—originate eccentrically from the dorsal-lateral aspects of the proximal phalanx condyles and insert into the volar-lateral middle phalanx and the margins of the volar plate, respectively. These structures provide critical mediolateral stability and act as a dynamic tension band throughout the entire arc of motion, tightening in flexion and relaxing slightly in extension due to the cam effect of the condylar head.

Regarding the dynamic tendon attachments, the extensor mechanism's central slip inserts into the dorsal base of the middle phalanx, providing a relatively weak dorsal proximal force vector. In stark contrast, the flexor digitorum superficialis (FDS) tendon slips insert broadly along the volar aspect of the middle phalanx, providing a massive volar distal force. This inherent physiological imbalance dictates that flexor forces typically dominate extensor forces. When the primary volar restraint—the volar plate—fails in the setting of a dorsal fracture-dislocation, these dominant flexor forces, coupled with the joint's inclined geometry, create a powerful lever arm. This lever arm inexorably leads to dorsal subluxation and proximal migration of the main dorsal fracture fragment of the middle phalanx.
Extensive biomechanical research and decades of clinical experience have demonstrated that the PIP joint will generally remain concentrically stable if up to roughly 40% to 42% of the volar half of the middle phalanx articular surface is damaged, provided the remaining dorsal articular surface maintains a congruent arc with the proximal phalanx. This is classically assessed on a true, perfectly superimposed lateral radiograph. The intact dorsal cartilage must perfectly cup the condyles of the proximal phalanx to maintain a stable fulcrum for rotation.

However, fellows, I must caution you: in actual clinical practice, dynamic subluxation can occur with as little as 10% to 15% joint surface loss, particularly if the collateral ligament origins are compromised or if the patient exhibits baseline ligamentous laxity. More severe injuries, involving a greater portion of the volar lip (often >50%), are inherently longitudinally unstable. For true pilon fractures, the proximal phalanx condyles are driven deep into the middle phalanx base like a wedge, displacing the central articular surface distally and splaying the margins outward. This destroys the cup-like geometry of the base, resulting in profound proximal migration, diminution or complete obliteration of the joint space, and catastrophic articular incongruity.


Exhaustive Indications and Contraindications
The decision to utilize dynamic external fixation over alternative modalities—such as extension block splinting, formal ORIF, volar plate arthroplasty, or hemi-hamate osteochondral autograft reconstruction—requires nuanced clinical judgment and a deep appreciation for the soft tissue envelope. Dynamic external fixation relies entirely on the principle of ligamentotaxis. By applying controlled longitudinal distraction across the joint, the intact soft tissue envelope (collateral ligaments, volar plate remnants, and extensor/flexor expansions) is placed under tension. This tension indirectly reduces the comminuted articular fragments, pulling them back toward their native anatomical alignment, and maintains the joint space, preventing the proximal phalanx from acting as a destructive battering ram during motion.
The ideal indication for a dynamic external fixator (such as the Suzuki frame, compass hinge, or modified force-couple splints) is an unstable, highly comminuted intra-articular fracture of the PIP joint (typically involving >40% of the articular surface) where the fragments are simply too small, osteopenic, or numerous to hold rigid internal fixation (screws or plates). It is the undisputed gold standard for the "unfixable" pilon fracture. Furthermore, it is highly beneficial for delayed presentations (2-4 weeks post-injury) where early contractures have begun to form, as the frame can gradually distract and reduce the joint over several days, overcoming early soft tissue tethering.


Conversely, dynamic external fixation is relatively contraindicated in simple, large-fragment, two-part shear fractures. These injuries are far better served by precise anatomical reduction and rigid interfragmentary screw fixation, which allows for immediate, unrestricted motion without the burden and pin-tract risks of an external frame. Additionally, dynamic fixation is absolutely contraindicated in patients with severe non-compliance, profound cognitive impairment, or active local soft tissue infections, as pin tract care is a rigorous and necessary component of postoperative management. Without diligent patient participation, the frame becomes a liability rather than a therapeutic asset.
| Parameter | Indications for Dynamic External Fixation | Contraindications for Dynamic External Fixation |
|---|---|---|
| Fracture Pattern | Highly comminuted PIP pilon fractures; Unstable dorsal fracture-dislocations (>40% articular involvement). | Simple 2-part shear fractures; Extra-articular diaphyseal fractures. |
| Fragment Size | Fragments too small/fragile for screws (<1-2mm); "Eggshell" comminution. | Large, singular volar or dorsal lip fragments highly amenable to lag screws. |
| Timing | Acute injuries; Delayed presentations (up to 4-6 weeks) with reducible subluxation via traction. | Chronic, rigid, fixed subluxations (>6-8 weeks) requiring salvage arthroplasty/arthrodesis. |
| Patient Factors | Compliant patient capable of pin site care and rigorous daily active ROM exercises. | Non-compliant patient; Active local infection; Severe psychiatric/cognitive disorders. |
| Bone Quality | Osteopenic bone where internal hardware would inevitably fail or cut out. | Dense, healthy bone supporting rigid internal fixation (relative contraindication). |

Pre-Operative Planning, Templating, and Patient Positioning
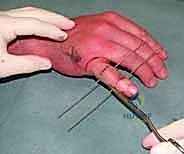
Patients typically present to the clinic or emergency department with a grossly swollen, ecchymotic, and exquisitely tender digit, centered precisely around the PIP joint. Angular deformity or clinically evident dorsal subluxation is often visually apparent or palpable to the discerning examiner. Range of motion is virtually non-existent due to a combination of mechanical osseous block, profound hemarthrosis, and guarding pain. A meticulous neurovascular examination is mandatory, though digital nerve or arterial compromise is thankfully rare in closed injuries.
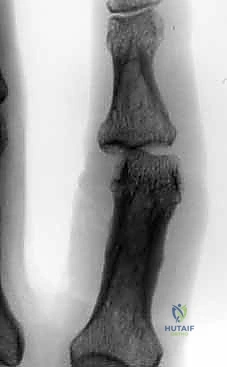
The absolute cornerstone of preoperative diagnosis and surgical templating is high-quality, orthogonal plain radiography. Crucially, we require a true posteroanterior (PA) and a true lateral radiograph centered specifically on the injured PIP joint. Standard "hand series" radiographs are entirely inadequate, as the overlapping digits and divergent x-ray beams obscure the subtle articular congruency of the individual phalanges due to parallax error. On the lateral view, we meticulously assess the "V sign"—a divergence of the joint space indicating dorsal subluxation—and quantify the percentage of volar base involvement. The presence of a V sign confirms that the joint is not concentrically reduced and that the dorsal articular arc is compromised.


For highly complex pilon injuries, I strongly advocate for a limited-field-of-view computed tomography (CT) scan with sub-millimeter slice thickness and 3D reconstructions. This allows for precise mapping of the articular fragments, particularly identifying the location of the central depressed "die-punch" fragment and assessing the integrity of the dorsal cortex, which will serve as the foundation for our distal fixation pins. The CT scan is invaluable for confirming that there is sufficient intact diaphyseal bone in the middle phalanx to safely anchor the distal components of the external fixator without propagating fracture lines.

In the operating theater, patient positioning and anesthesia are critical for success. The patient is positioned supine with the affected extremity extended on a radiolucent hand table. While regional anesthesia (such as an axillary or supraclavicular brachial plexus block) is standard, I increasingly favor Wide Awake Local Anesthesia No Tourniquet (WALANT). Utilizing a local injection of lidocaine with epinephrine allows the patient to remain comfortably awake and entirely pain-free while avoiding the ischemic pain of a tourniquet. The profound advantage of WALANT in dynamic external fixation is that once the frame is applied, the surgeon can ask the patient to actively flex and extend the digit. This provides immediate, real-time visual and fluoroscopic confirmation that the joint remains concentrically reduced throughout the entire functional arc of motion, without the confounding variable of muscle paralysis.


Step-by-Step Surgical Approach and Fixation Technique
The fundamental goal of the dynamic external fixator is to recreate the precise rotational axis of the PIP joint, apply longitudinal distraction to achieve ligamentotaxis, and permit immediate active motion. We will describe the construction of a modified pins-and-rubber-band traction system, heavily inspired by the classic Suzuki frame, which remains the workhorse for these injuries due to its versatility and low profile.
Establishing the Isocentric Axis of Rotation
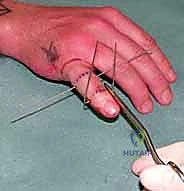
The most critical step of the entire procedure is the accurate placement of the central axis pin. The anatomical center of rotation of the PIP joint lies in the center of the condylar head of the proximal phalanx. Using a mini C-arm fluoroscope positioned parallel to the floor (allowing the surgeon to operate without fighting the machine), a true lateral view of the proximal phalanx is obtained. The condyles must be perfectly superimposed, appearing as a single, perfect circle on the monitor. If you see two distinct condylar outlines, you are not perfectly lateral, and your axis pin will be skewed, leading to eccentric motion and joint binding.

Once the perfect lateral is achieved, a 1.14 mm (0.045 inch) Kirschner wire (K-wire) is introduced precisely at the center of this circle. This wire is driven transversely from lateral to medial (or medial to lateral, depending on surgeon preference and access), ensuring it is strictly perpendicular to the longitudinal axis of the proximal phalanx in both the coronal and sagittal planes. This pin serves as the primary fulcrum for the dynamic frame. Any deviation from the true anatomical axis will result in a cam effect during flexion, either over-distracting the joint or causing catastrophic re-impaction of the articular fragments.

Pin Placement and Frame Construction
Following the successful placement of the axis pin, attention is turned to the distal fixation. A second 1.14 mm K-wire is placed transversely through the diaphysis of the middle phalanx, distal to the fracture extent. It is imperative to review the preoperative CT scan to ensure this pin does not inadvertently propagate a longitudinal split. This pin should be placed parallel to the axis pin in the coronal plane.


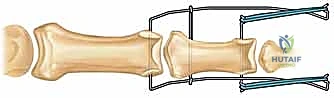
Next, the traction construct is fabricated. We utilize a third K-wire (often slightly thicker, 1.25 mm, for added rigidity) to create the dynamic traction bow. This wire is bent into a U-shape, with the width meticulously measured to clear the soft tissues of the digit by at least 5 mm on each side to accommodate postoperative swelling. The ends of this U-shaped wire are bent into small hooks or loops. The proximal ends of the U-wire are then secured to the axis pin in the proximal phalanx. This can be achieved by bending the axis pin itself to capture the U-wire, or by using small acrylic resin blocks or specialized clamps, depending on the specific commercial or custom system being utilized.

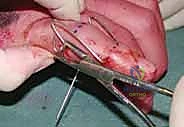
The distal middle phalanx pin is similarly bent at 90 degrees on both sides, extending distally to create hooks. It is crucial that the wire bending is performed with specialized heavy-duty wire benders to ensure sharp, precise angles without placing undue torque on the bone, which could cause iatrogenic fractures. The sharp ends of all K-wires must be cut and capped to protect the patient and the therapist from injury.


Achieving Ligamentotaxis and Intraoperative Assessment
With the bony anchors in place, the dynamic element is introduced. Sterile orthodontic rubber bands are applied between the hooks of the distal middle phalanx pin and the hooks of the U-shaped traction bow. The tension of these rubber bands provides the longitudinal traction necessary for ligament
Clinical & Radiographic Imaging Archive