Excision of Wrist Ganglia and Hand Cysts: Surgical Guide

Key Takeaway
The surgical management of hand and wrist cysts requires a meticulous understanding of carpal anatomy and joint biomechanics. Whether performing an open excision of a volar wrist ganglion, an arthroscopic resection of a dorsal ganglion, or addressing distal interphalangeal mucous cysts, precise stalk excision and capsular management are paramount. This guide details evidence-based surgical techniques, portal placements, and postoperative rehabilitation protocols to minimize recurrence and optimize functional outcomes.
INTRODUCTION TO WRIST AND HAND CYSTS
Tumorous conditions of the hand and wrist are predominantly benign, with ganglion cysts representing the most common soft-tissue masses encountered by the orthopedic surgeon. Arising from myxoid degeneration of connective tissue or via a one-way check-valve mechanism from an adjacent joint or tendon sheath, these lesions require precise surgical management to alleviate pain, restore biomechanics, and minimize the risk of recurrence.
This comprehensive masterclass details the operative management of volar and dorsal wrist ganglia, alongside specialized approaches for epidermoid inclusion cysts, sebaceous cysts, and mucous cysts of the distal interphalangeal (DIP) joint.
EXCISION OF A VOLAR WRIST GANGLION
Volar wrist ganglia typically originate from the radiocarpal joint or the scaphotrapezial-trapezoid (STT) joint. They frequently present intimately associated with the radial artery and the flexor carpi radialis (FCR) tendon. Surgical excision demands meticulous dissection to protect the palmar cutaneous branch of the median nerve and the radial artery.
Surgical Approach and Stalk Resection
The procedure is performed under regional or general anesthesia with a well-padded proximal tourniquet. A longitudinal or curvilinear incision is made over the mass, avoiding perpendicular crossing of the wrist flexion creases.
🔪 Surgical Warning: The radial artery often drapes directly over the dome of a volar ganglion. The surgeon must perform careful subadventitial dissection to mobilize the artery away from the cyst wall. Never blindly puncture or aggressively retract the vascular bundle.
Once the radial artery and the FCR tendon are retracted, the cyst is traced down to its capsular origin. The stalk is typically found at the radioscaphocapitate (RSC) or long radiolunate (LRL) ligaments. A small window of the joint capsule surrounding the stalk is excised to ensure complete removal of the check-valve mechanism.
Closure and Postoperative Care
After meticulous hemostasis is achieved—often requiring bipolar electrocautery to avoid thermal injury to adjacent neurovascular structures—irrigate the wound copiously with sterile saline.
Close the wound with a running 4-0 or 5-0 subcuticular monofilament suture. This closure should be reinforced with a skin adhesive and Steri-Strips before any local block anesthetic (such as bupivacaine) is administered to the surgical site to prevent distortion of the wound edges. Apply a soft, lightly compressive sterile dressing to minimize postoperative edema and hematoma formation.
Postoperative Protocol:
* Immobilization: A volar wrist splint is applied and worn continuously for 2 weeks.
* Suture Removal: Sutures (if non-absorbable) are removed at the 2-week postoperative mark.
* Rehabilitation: Active range-of-motion (ROM) exercises are initiated immediately following splint removal to prevent capsular stiffness and tendon adhesions.
ARTHROSCOPIC RESECTION OF A DORSAL WRIST GANGLION
Dorsal wrist ganglia predominantly arise from the scapholunate (SL) interval, specifically originating from the dorsal capsuloscapholunate septum (DCSS). Arthroscopic resection has become a gold-standard alternative to open excision, offering decreased postoperative stiffness, smaller incisions, and a faster return to baseline function.
Indications and Setup
Arthroscopic resection is indicated for symptomatic dorsal ganglia that have failed conservative management (e.g., aspiration, immobilization).
Patient Positioning and Anesthesia:
* Use an axillary regional block or general anesthesia.
* Apply a proximal pneumatic tourniquet to allow for bloodless, clear exposure of the joint.
* Apply longitudinal distraction using finger traps attached to the index, long, and ring fingers.
* Apply countertraction of 3 to 4 kg at the upper arm using a padded boom or counter-weight system.
Surgical Technique (Osterman and Raphael; Luchetti et al.)
💡 Clinical Pearl: The success of arthroscopic ganglionectomy relies entirely on the adequate resection of the capsular stalk. Failure to resect a 1-cm window of the dorsal capsule significantly increases the recurrence rate.
- Portal Placement: Make two primary portals for access to the radiocarpal joint.
- Diagnostic Arthroscopy: Place a 1.9-mm or 2.7-mm arthroscope into the 3-4 portal to examine the joint. If this portal does not offer clear exposure of the dorsal capsule and SL interval, move the arthroscope to the 4-5, 1-2, or 6R portals.
- Identification of the Stalk: Locate the scapholunate interosseous ligament. Direct the arthroscope dorsally to view the ganglion or its capsular stalk.
- Probing: Introduce an arthroscopic probe through an accessory portal (or the 3-4 portal if the scope is repositioned) to palpate the scapholunate ligament and the dorsal capsule. This determines the consistency of the ligament and confirms the exact location of the ganglion's stalk.
- Capsular Resection: Use a 2.0-mm or 2.9-mm full-radius shaver or an end-cutting resector to excise a 1-cm diameter area of the dorsal capsule and the stalk.
- Extensor Tendon Visualization: As the dorsal capsule is resected, the overlying extensor tendons (typically the Extensor Digitorum Communis) will become visible. When the extensor tendon is seen, stop the capsular resection immediately. Do not damage this tendon.
- Ligament Preservation: If an intraligamentous ganglion is found, exercise extreme caution to avoid damaging the structural integrity of the scapholunate ligament during resection, which could precipitate a dorsal intercalated segment instability (DISI) deformity.
- Midcarpal Assessment: Occasionally, midcarpal portals (radial midcarpal [RMC] or ulnar midcarpal [UMC]) are necessary to locate the ganglion and identify its stalk if it extends distally.
- Conversion to Open: Convert to an open procedure without hesitation if there is any doubt about the complete arthroscopic resection of the stalk.
- Closure: Close the portals with a single simple stitch or Steri-Strips, or leave them open to allow for the drainage of irrigation fluid. Apply a palmar wrist splint in a neutral position.
Postoperative Care:
The wrist is mobilized twice a day out of the splint to encourage early gliding. The splint is permanently removed after 1 week. Formal physiotherapy is continued for 2 weeks to restore terminal flexion and extension. The patient is strictly advised to avoid strenuous work or heavy lifting for at least 3 weeks after arthroscopy.
EPIDERMOID CYST (INCLUSION CYST)
Epidermoid cysts, also known as inclusion cysts, are unique tumorous lesions of the hand. It is now generally accepted that epidermoid cysts develop from the traumatic implantation of epithelial cells (stratum corneum) into the deep subcutaneous tissues or bone.
Clinical Presentation and Pathophysiology
The patient history usually involves a penetrating wound—such as a needle prick, thorn puncture, or crush injury—around the palm or fingertip several months or even years before the mass becomes clinically apparent.
Figure 77-27 A: Epidermoid inclusion cyst presenting as a bulbous mass after a puncture wound to the index finger.
Clinically, it presents as a hard, rubbery, nontender subcutaneous mass. Because the implanted epithelial cells continue to produce keratin, the cyst slowly expands.
Radiographic Evaluation
The distal phalanx is the most common osseous site for an epidermoid cyst. When the cyst occurs at the base of a fingernail and invades the distal phalanx, it closely mimics the radiographic appearance of an enchondroma or a glomus tumor.

Figure 77-27 B: Anteroposterior radiograph demonstrating a soft tissue mass and well-circumscribed central bony erosion of the distal phalanx.
On radiographs, the cortex appears expanded, and a central lytic lesion is typically the only bony reaction. Unlike malignant lesions, there is usually a distinct sclerotic margin indicating a slow-growing, benign process.
Surgical Management
Surgical removal of the cyst is curative. The approach must allow for complete excision of the cyst wall to prevent recurrence.
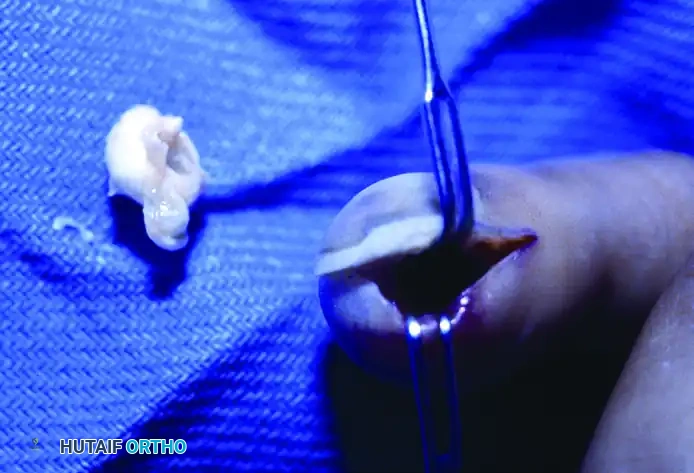
Figure 77-27 C: Intraoperative view demonstrating the meticulous excision of the epidermoid cyst.
If the bone is involved, thorough curettage of the lytic cavity is mandatory. Following curettage, bone grafting (using local bone dust, allograft, or a small autograft from the distal radius) is recommended to restore the structural integrity of the distal phalanx and prevent pathologic fracture.
SEBACEOUS CYST
Sebaceous cysts are exceedingly rare in the hand. This is due to the anatomical fact that the palmar skin and the volar surfaces of the digits contain no sebaceous glands.
When a cyst is encountered in the subcutaneous tissues of the hand with mobile overlying skin, it can easily be confused with a sebaceous cyst; however, it is almost always an epidermoid inclusion cyst. True sebaceous cysts may occasionally be found on the dorsal aspect of the hand or proximal digits where hair follicles and associated sebaceous glands are present. Excision follows standard principles of complete capsular removal.
MUCOUS CYST
Mucous cysts are specialized ganglion cysts that occur frequently on the dorsum of the digits, specifically over the distal interphalangeal (DIP) joints. They are predominantly seen in women between the fifth and seventh decades of life.
Pathophysiology and Biomechanics
Mucous cysts are thought to result from the myxomatous degeneration of the connective tissue surrounding the DIP joint. They are intimately associated with underlying osteoarthritis of the DIP joint and frequently present alongside Heberden nodes.
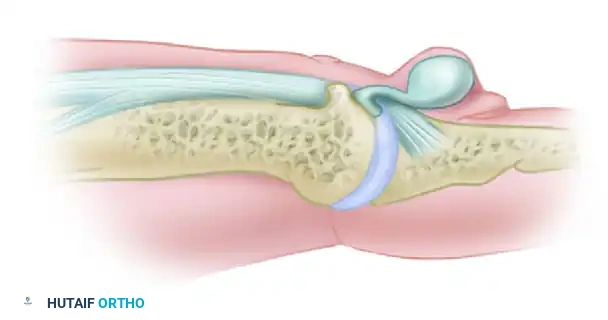
Figure 77-28 (Dorsal View): Relationship between the mucous cyst and the marginal osteophyte of the distal interphalangeal joint.
The cyst communicates directly with the joint space. While this thin communication stalk may become pinched off over time, at some stage in its development, it is in direct communication with the synovial fluid of the joint.

Figure 77-28 (Lateral View): The marginal osteophyte produces attrition of the extensor tendon expansion with motion, while the cyst displaces the germinal matrix of the nail.
The overlying skin often becomes so thin and translucent due to the pressure of the expanding cyst that clear, viscous mucoid fluid can be seen within. If left untreated, the cyst can cause pressure necrosis of the overlying skin, leading to spontaneous rupture, which carries a high risk of secondary septic arthritis of the DIP joint. Furthermore, pressure on the germinal matrix of the nail bed frequently causes longitudinal grooving or deformity of the fingernail.
Radiographic Evaluation
Anteroposterior, lateral, and oblique radiographic views of the affected digit almost always show an osteophyte near the cyst at the dorsal base of the distal phalanx or the head of the middle phalanx. Identifying this osteophyte is a critical step in preoperative planning.
Surgical Excision and Reconstruction
Successful surgical management requires a tripartite approach: excision of the cyst, excision of the stalk, and debridement of the underlying osteophyte.
🔪 Surgical Warning: Failure to excise the underlying marginal osteophyte is the leading cause of mucous cyst recurrence. The osteophyte acts as a mechanical irritant to the joint capsule, perpetuating the check-valve mechanism.

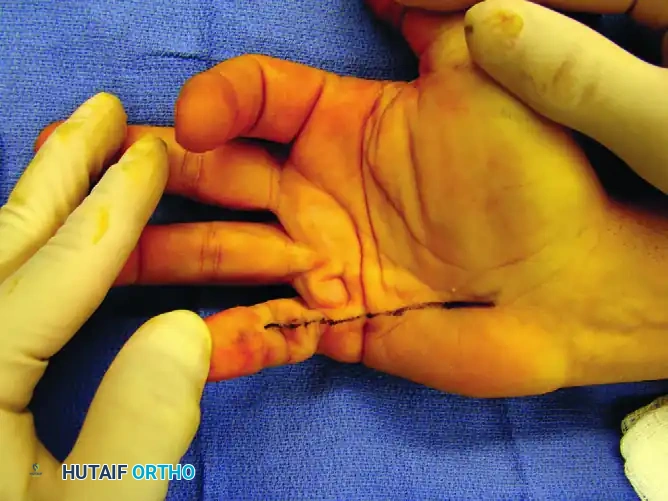
Figure 77-29 A: Mucous cyst with the planned surgical excision margins outlined. Note the proximity to the eponychial fold.
Surgical Steps:
1. Incision: A T-shaped, H-shaped, or curved incision is made over the DIP joint, carefully elevating the skin flaps. If the skin is paper-thin and intimately involved with the cyst wall, it must be excised en bloc with the cyst.
2. Cyst and Stalk Excision: The cyst is carefully dissected away from the extensor terminal tendon. The stalk is traced down to the DIP joint capsule.
3. Osteophyte Resection: The joint capsule is opened, and a rongeur or a small high-speed burr is used to aggressively resect the dorsal marginal osteophytes. The joint is then copiously irrigated.
4. Soft Tissue Coverage: Because the overlying skin frequently requires excision, primary closure may not be possible without undue tension.
* A small split-thickness or full-thickness skin graft is occasionally required. The skin graft is easily removed freehand from a variety of sites from the same arm (e.g., the hypothenar eminence or the proximal volar forearm).
* Alternatively, many surgeons prefer to rotate a small local skin flap (such as a rhomboid flap or a rotation-advancement flap) over the defect to provide robust, vascularized coverage.

Figure 77-29 B: Postoperative appearance after healed skin grafting, demonstrating excellent contour and resolution of the nail deformity.
Postoperatively, the DIP joint is immobilized in full extension for 10 to 14 days to allow for graft incorporation and wound healing, after which active flexion exercises are commenced to restore digit function.
You Might Also Like