Comprehensive Introduction and Patho-Epidemiology
The surgical correction of a severe hammer toe deformity represents a formidable biomechanical and anatomical challenge in the realm of advanced forefoot reconstruction. By precise clinical definition, a severe hammer toe deformity is characterized by a rigid, fixed extension contracture at the metatarsophalangeal (MTP) joint coupled inextricably with a fixed flexion contracture at the proximal interphalangeal (PIP) joint. Because the deformity is rigidly fixed at both distinct centers of rotation, isolated surgical procedures directed solely at the PIP joint—such as traditional arthrodesis or simple resection arthroplasty—will universally fail to correct the global sagittal and coronal alignment of the digit. Both joints require a meticulously planned, systematic, and sequential correction to restore a plantigrade, functional, and pain-free forefoot.
The pathoanatomy underlying this complex deformity is primarily driven by a dynamic, progressive imbalance between the intrinsic and extrinsic musculature of the foot. As the intrinsic muscles (specifically the lumbricals and interossei) fail, attenuate, or are mechanically overpowered, the extrinsic extensor digitorum longus (EDL) exerts an unopposed, continuous extension force on the proximal phalanx via the extensor sling mechanism. Over a prolonged period, this chronic hyperextension leads to severe attenuation, degenerative tearing, and eventual complete rupture of the plantar plate. Concurrently, the collateral ligaments undergo asymmetric contracture, culminating in dorsal subluxation or frank dorsal dislocation of the MTP joint. Simultaneously, the extrinsic flexors—the flexor digitorum longus (FDL) and flexor digitorum brevis (FDB)—exert an unopposed pull on the middle and distal phalanges, dragging the PIP joint into a rigid, unyielding flexion posture.
Epidemiologically, severe hammer toe deformities with concomitant MTP joint dislocation are disproportionately observed in the aging population, with a marked predilection for female patients. This gender disparity is frequently attributed to the long-term use of constrictive, narrow-toebox footwear with elevated heels, which forces the MTP joints into chronic hyperextension while simultaneously crowding the digits. Furthermore, systemic inflammatory arthropathies, most notably rheumatoid arthritis, dramatically accelerate the destruction of the MTP joint capsular structures, leading to rapid and severe multi-digit dislocations. Neuromuscular disorders, such as Charcot-Marie-Tooth disease or diabetic peripheral neuropathy, also frequently present with severe intrinsic minus foot types, precipitating rapid and rigid hammer toe formations.
Understanding the natural history of this deformity is paramount for the operating surgeon. What begins as a flexible, reducible deformity invariably progresses to a rigid, fixed contracture as the periarticular soft tissues undergo fibrotic transformation and the articular cartilage experiences abnormal, asymmetric loading. The retrograde plantarflexion force exerted by the dorsally dislocated proximal phalanx drives the metatarsal head plantarly, resulting in severe, intractable plantar keratosis (IPK) and, in neuropathic patients, deep plantar ulcerations. Thus, the surgical intervention is not merely cosmetic; it is a critical limb-salvage and function-restoring necessity designed to re-establish the normal weight-bearing mechanics of the forefoot.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the dorsal extensor apparatus and the plantar capsulo-ligamentous complex is absolutely mandatory for the operating surgeon attempting to reconstruct a severe hammer toe. The extensor apparatus of the lesser toes is a highly intricate, multi-layered structure that dictates the dynamic balance of the digit. The extensor digitorum brevis (EDB) tendon lies slightly fibular and deep to the more robust extensor digitorum longus (EDL) tendon. The EDB joins the EDL and the extensor expansion at the level of the metatarsal neck. Recognizing this specific anatomical confluence is critical, as the EDB must be surgically addressed and neutralized prior to lengthening the EDL to achieve adequate tendon excursion and eliminate secondary deforming forces.
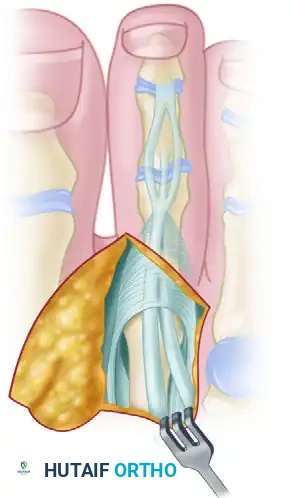
Diagram illustrating the anatomic relationship between the EDB (fibular/deep) and the EDL.
The MTP joint capsule itself presents a highly variable and often treacherous pathology in the setting of severe, chronic deformity. In a healthy joint, the capsule is a thin, pliable synovial layer that allows for smooth, uninhibited gliding. However, in chronic deformities characterized by recurrent synovial inflammatory episodes—frequently encountered in rheumatoid arthritis or severe degenerative joint disease—the capsule undergoes profound fibrotic transformation. It thickens into a dense, unyielding fibrous encapsulation that rigidly tethers the joint in hyperextension. The dorsal capsule blends intimately with the extensor sling, creating a continuous fibrotic band that must be meticulously released to achieve any degree of plantarflexion.
The collateral ligament complex of the MTP joint is composed of the proper collateral ligaments (PCL) and the accessory collateral ligaments (ACL). The PCL originates from the dorsal-lateral aspect of the metatarsal head and inserts onto the plantar-lateral base of the proximal phalanx, primarily resisting varus/valgus deviation. The ACL originates slightly more plantarly and inserts directly into the plantar plate, suspending the plate beneath the metatarsal head. In a severe extension contracture, both the PCL and ACL become severely contracted and shortened. When the toe is forced into extension, these ligaments act as rigid tethers, preventing the proximal phalanx from gliding plantarly over the metatarsal condyles.
The plantar plate is the primary static stabilizer of the MTP joint in the sagittal plane. It is a thick, fibrocartilaginous structure that originates from the plantar metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. It serves as the insertion point for the plantar fascia via the natatory ligaments, forming the critical "windlass mechanism" described by Hicks. In severe hammer toe deformities, the plantar plate is invariably stretched, attenuated, or completely torn from its phalangeal insertion. Understanding that the plantar plate is structurally compromised dictates that any surgical correction must not only release the dorsal tethers but also account for the loss of plantar stability, often necessitating temporary K-wire fixation to allow the plantar structures to scar and heal in a shortened, functional position.
Exhaustive Indications and Contraindications
The decision to proceed with surgical correction of a severe hammer toe and MTP joint deformity must be predicated on a thorough clinical and radiographic evaluation. Surgery is rarely indicated for purely cosmetic reasons; rather, it is reserved for patients experiencing significant pain, functional limitation, or impending soft tissue compromise that has proven completely refractory to conservative measures such as extra-depth footwear, custom orthoses with metatarsal offloading pads, and toe crests.
The primary indication for this complex reconstruction is a fixed extension contracture of the MTP joint (typically exceeding 20 degrees) coupled with a fixed flexion contracture of the PIP joint. Patients frequently present with overlying painful adventitial bursitis, hyperkeratotic lesions, or frank dorsal ulcerations over the PIP joint due to direct shoe pressure. Furthermore, the presence of an intractable plantar keratosis (IPK) beneath the affected metatarsal head is a strong indication for surgery. This IPK is the direct mechanical result of retrograde plantarflexion forces from the dislocated proximal phalanx driving the metatarsal head into the plantar skin during the stance phase of gait.
Contraindications must be rigorously respected to prevent catastrophic postoperative complications, including digital ischemia, nonunion, and deep infection. Severe peripheral arterial disease is an absolute contraindication; a preoperative Ankle-Brachial Index (ABI) of less than 0.4 or absent palpable pedal pulses combined with poor capillary refill mandates vascular surgery consultation prior to any elective orthopedic intervention. Active localized soft tissue infection or untreated osteomyelitis also absolutely precludes elective reconstruction. Relative contraindications include poorly controlled diabetes mellitus (HbA1c > 8.0%), heavy tobacco use, and severe psychiatric non-compliance, all of which significantly elevate the risk of wound dehiscence and hardware failure.
| Category | Specific Condition | Rationale / Surgical Implication |
|---|---|---|
| Absolute Indications | Fixed MTP extension > 20° with pain | Deformity is rigid; conservative care will fail to restore alignment. |
| Absolute Indications | Dorsal MTP dislocation with IPK | Retrograde metatarsal head pressure causes severe plantar pain/ulcer risk. |
| Absolute Indications | Impending/active ulceration over PIP | Shoe pressure threatens joint space; requires immediate decompression. |
| Relative Indications | Flexible deformity failing orthotics | May be treated with lesser soft-tissue procedures (e.g., flexor tenotomy). |
| Absolute Contraindications | Severe Vascular Disease (ABI < 0.4) | High risk of digital gangrene and amputation following tourniquet/incision. |
| Absolute Contraindications | Active local infection / Osteomyelitis | Hardware placement will sequester infection; requires eradication first. |
| Relative Contraindications | Uncontrolled Diabetes (HbA1c > 8.0%) | Impaired wound healing, increased risk of deep space infection. |
| Relative Contraindications | Heavy active smoking | Microvascular compromise; significantly delays bone and soft tissue healing. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful surgical outcome. The clinical evaluation must include a dynamic assessment of the foot and ankle. The Silfverskiöld test is mandatory to evaluate for isolated gastrocnemius contracture versus a combined Achilles tendon contracture, as an unrecognized equinus deformity will place excessive retrograde pressure on the forefoot, virtually guaranteeing a recurrence of the MTP joint pathology. The Kelikian push-up test—applying upward pressure on the plantar aspect of the metatarsal heads—allows the surgeon to assess the rigidity of the MTP and PIP joints. In a severe, fixed deformity, the push-up test will fail to reduce the digit to a plantigrade position.
Standard weight-bearing radiographs, including anteroposterior (AP), lateral, and sesamoid axial views, are critical. On the AP radiograph, the surgeon must evaluate the metatarsal parabola (Maestro criteria) to identify any abnormally long metatarsals that may be contributing to the deformity. A long second metatarsal is a classic predisposing factor for second MTP joint instability and crossover toe deformity. The lateral radiograph is essential for quantifying the degree of dorsal MTP subluxation or frank dislocation, as well as assessing the bone quality (osteopenia) which may dictate the choice of fixation.
Surgical templating involves determining the anticipated amount of metatarsal shortening required if a Weil osteotomy is planned. The goal is to restore a harmonious metatarsal cascade. The surgeon must calculate the exact millimeter resection required to decompress the joint without causing excessive shortening, which would result in transfer metatarsalgia to the adjacent rays. If multiple digits are involved, the overall cascade must be templated to ensure a smooth, parabolic curve from the first to the fifth metatarsal.
Patient positioning is typically supine on a standard radiolucent operating table. A small bump is placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral, upward-facing position. A well-padded pneumatic tourniquet is applied. The choice of tourniquet location (thigh, calf, or ankle) depends on surgeon preference and the extent of the planned procedure. For isolated forefoot reconstruction, a calf or ankle tourniquet inflated to 250 mmHg provides an excellent, bloodless surgical field while minimizing thigh tourniquet-related discomfort and deep vein thrombosis risk. Intravenous prophylactic antibiotics (typically a first-generation cephalosporin) are administered 30 minutes prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
1. Incision and Exposure
The procedure commences at the metatarsophalangeal joint. The surgical approach must provide extensile, unhindered exposure to the extensor apparatus, the dorsal MTP joint capsule, and the metatarsal head without compromising the fragile vascular supply to the dorsal skin flaps. Meticulous soft tissue handling is paramount.
Make a straight or slightly angled longitudinal incision centered over the fibular aspect of the metatarsophalangeal joint. Placing the incision slightly fibular to the midline helps avoid the primary dorsal cutaneous nerve branches and provides excellent access to the fibular-sided extensor digitorum brevis.

Diagrammatic representation of the incision placement over the fibular aspect of the MTP joint.

Clinical photograph demonstrating the planned surgical incision.
Carefully deepen the incision through the dermis using a No. 15 blade. As you dissect through the subcutaneous tissues, you will invariably encounter branches of the dorsal venous arch returning from the toe. These vessels must be meticulously isolated and cauterized using bipolar electrocautery, or gently retracted with fine skin hooks to expose the underlying extensor tendons. Failure to achieve absolute hemostasis at this stage will result in a bloody, obscured surgical field that makes identification of the delicate extensor expansion and capsular structures exceedingly difficult. Retract the skin flaps using blunt Senn retractors, ensuring full-thickness flaps to prevent marginal skin necrosis.
2. Extensor Tendon Management
With the subcutaneous tissues retracted, identify the extensor digitorum longus (EDL) and the extensor digitorum brevis (EDB). The EDB is located slightly fibular and deep to the EDL. Trace both tendons distally to the neck of the metatarsal, precisely where the EDB merges with the EDL to form the extensor expansion.
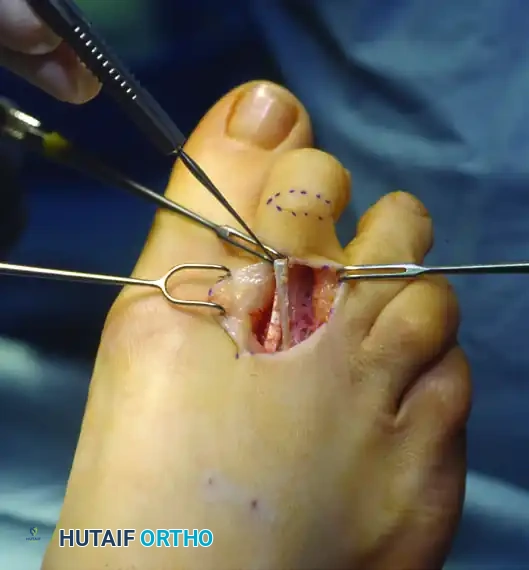
Clinical exposure of the extensor tendons prior to surgical lengthening.
Before this confluence, dissect the EDB away from the EDL using sharp and blunt dissection. Perform a tenectomy by sharply excising a 2- to 3-mm segment of the extensor digitorum brevis. This critical step eliminates the secondary, often overlooked, deforming extension force that can cause postoperative recurrence if left intact.
Next, address the primary deforming force: the EDL.
1. Perform a formal Z-plasty lengthening of the extensor digitorum longus. The use of a small, precise blade (such as a No. 67 Beaver blade or a No. 11 blade) is highly recommended to avoid fraying the tendon fibers.
2. From the proximal extent of the surgical exposure, make a longitudinal split down the exact center of the EDL tendon, continuing distally until the EDL joins with the extensor expansion over the MTP joint.
3. Exit the longitudinal incision at a right angle at the distal junction (extensor expansion).
4. Sever the tendon proximally at a right angle in the opposite direction to complete the "Z" configuration.
5. Lift the tendon away from any remaining underlying soft tissue or capsular attachments. This maneuver effectively lengthens the EDL by 8 to 12 mm, dramatically reducing the dynamic extension force on the proximal phalanx.
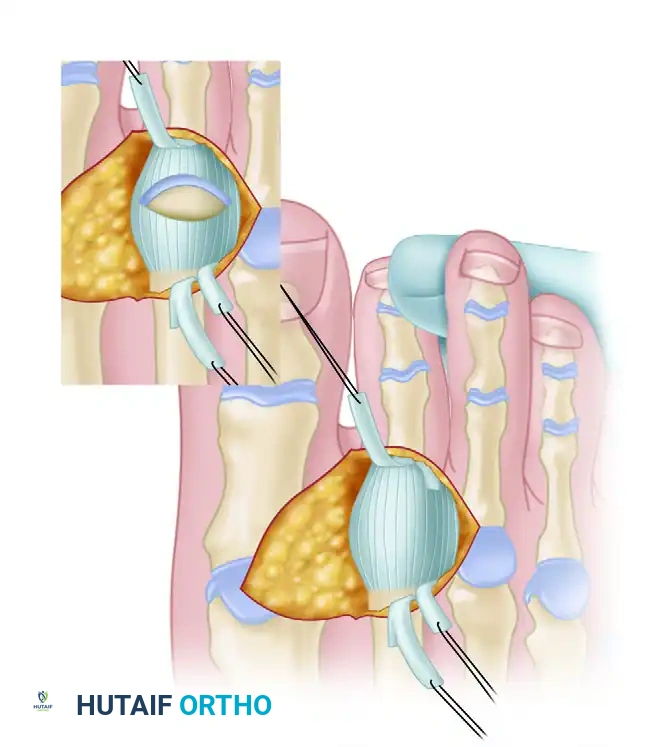
Diagram of the Z-plasty lengthening of the extensor digitorum longus.
Clinical execution of the EDL Z-plasty, demonstrating the achieved length.
3. Intraoperative Assessment and Sequential Release
The cornerstone of correcting severe MTP joint extension contractures is the strict adherence to a sequential soft tissue release. The surgeon must continuously reassess the resting posture of the toe after each individual anatomic structure is released. Over-releasing can lead to a destabilized, non-purchasing "floating toe," while under-releasing guarantees rapid recurrence of the deformity.
Scenario A: Mild Residual Contracture
If the extension contracture is now less than 20 to 30 degrees, and there is absolutely no dorsal subluxation of the proximal phalanx on the metatarsal head, firmly flex the toe 30 to 40 degrees. Load the foot by holding the ankle at 90 degrees (neutral) to simulate weight-bearing. If the toe rests in a neutral position at the MTP joint under these conditions, no further capsular release is required. The EDL will be sutured in its lengthened position only after the PIP joint deformity has been fully corrected.
Scenario B: Moderate Residual Contracture (The Dorsal Capsulotomy)
If the toe still rests in 10 to 20 degrees of extension after the Z-plasty, a formal dorsal capsulotomy is strictly indicated.
1. Firmly flex the toe 40 to 50 degrees. This acute flexion pulls the extensor expansion distally and places the dorsal capsule under maximum tension, providing superior exposure.
2. Using a No. 15 blade, perform a transverse dorsal capsulotomy just proximal to the joint line, ensuring complete release of the dorsal fibrotic tether.
3. Return the ankle to 90 degrees and observe the resting posture. If the posture is acceptable (neutral to 10 degrees of MTP extension), proceed to PIP correction.

Clinical photograph demonstrating the transverse dorsal capsulotomy performed with the toe in acute flexion.
Scenario C: Severe Residual Contracture (Collateral Ligament Release)
If the toe still exhibits an unacceptable extension posture or remains dorsally subluxated despite the capsulotomy, the collateral ligaments are acting as the primary rigid tethers.
1. Acutely flex the toe to place the collateral ligaments under maximum tension.
2. Using a small blade, carefully incise the collateral ligaments on both the medial and lateral sides of the metatarsal head. The blade should sweep from dorsal to plantar along the epicondyles.
3. Surgical Warning: Carry the incision down to, but strictly not through, the plantar plate of the metatarsophalangeal joint. Transecting the plantar plate will destroy the final static stabilizer, leading to catastrophic, uncorrectable dorsal instability.
4. This comprehensive release should allow the toe to assume a neutral to slightly flexed position at the MTP joint, allowing for complete reduction of the articular surfaces.
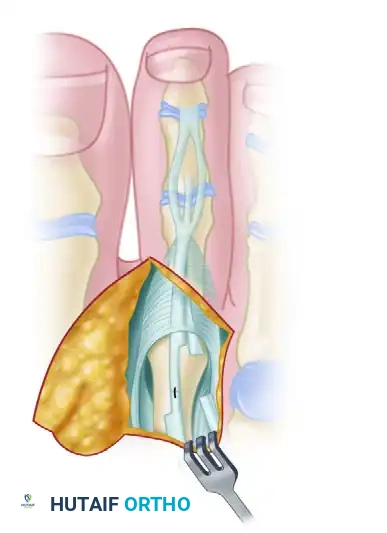
Diagram showing the release of the collateral ligaments down to the plantar plate.

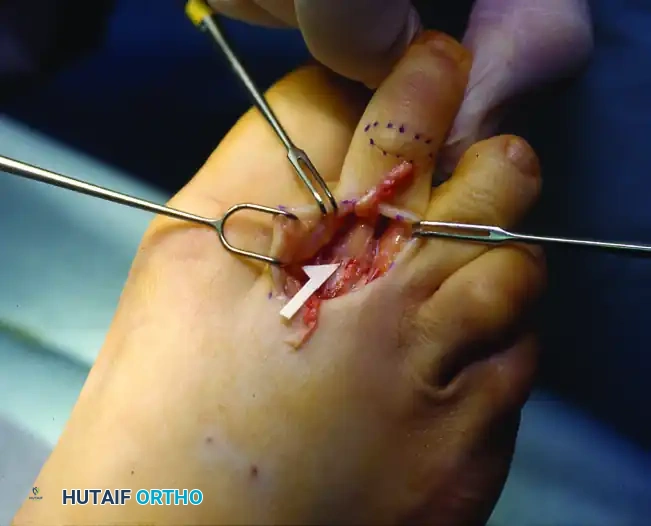
Clinical photograph of the collateral ligament release, allowing for complete reduction of the MTP joint.
4. Correction of Severe Deformity with Frank Dislocation (Osseous Decompression)
Severe deformity accompanied by chronic, frank dislocation of the metatarsophalangeal joint is notoriously difficult to correct and maintain. The soft tissue envelope is severely contracted dorsally and completely attenuated plantarly. While all aforementioned sequential soft tissue steps (EDB tenotomy, EDL Z-plasty, dorsal capsulotomy, collateral ligament release) must be meticulously performed, soft tissue release alone is vastly insufficient. The joint space has permanently contracted. Attempting to forcefully lever the proximal phalanx back over the metatarsal head will result in excessive intra-articular pressure, severe postoperative stiffness, vascular compromise, and inevitable recurrence. Osseous decompression of the metatarsophalangeal joint is absolutely mandated.
Decompression must be achieved strictly on the metatarsal side of the joint. Resecting the base of the proximal phalanx is historically described but is heavily discouraged in modern reconstructive surgery. Removing the phalangeal base destroys the critical insertion of the intrinsic musculature and the plantar plate (the windlass mechanism). This renders the digit a flail appendage, making it exceedingly difficult to maintain position, and highly increases the probability of a transfer lesion (a metatarsal head plantar callus developing laterally due to the total loss of the toe's weight-bearing function).
Instead, decompression is accomplished via:
1. Metatarsal Head Contouring (Arthroplasty): Reshaping the metatarsal head using a microsaw or rongeur to reduce its dorsal-plantar and medial-lateral dimensions. This removes the mechanical block to reduction, allowing the phalanx to glide back into place without tension.
2. Shortening (Weil) Osteotomy: This is the gold standard for severe dislocations. A distal oblique osteotomy of the metatarsal neck/head is performed parallel to the plantar surface of the foot. This allows the metatarsal head to slide proximally along the osteotomy plane, effectively shortening the bone and decompressing the joint space without negatively altering the plantar pressure mechanics. The osteotomy is secured with a single small fragment screw (e.g., 2.0mm twist-off screw).

Diagram demonstrating the initial assessment for metatarsal head contouring in a dislocated MTP joint.

Diagram showing the completed resection and contouring of the metatarsal head, allowing for tension-free reduction of the proximal phalanx.
5. Final Closure and Fixation
Once the MTP joint is fully reduced and osseously decompressed, surgical attention is turned to the PIP joint. The fixed flexion contracture at the PIP joint is typically addressed via a resection arthroplasty (resecting the head of the proximal phalanx) or a formal arthrodesis (using K-wires or intramedullary implants), depending on surgeon preference, patient activity level, and the rigidity of the deformity.
Only after the PIP joint is rigidly stabilized should the EDL be repaired. Suture the EDL in its new, lengthened position using a 3-0 or 4-0 absorbable suture (e.g., Vicryl). It is absolutely critical to ensure the ankle is held at exactly 90 degrees during this repair to set the appropriate resting tension of the extensor apparatus.
The reduced MTP joint and corrected PIP joint are universally stabilized with a smooth 0.045-inch or 0.062-inch Kirschner wire. The wire is driven retrograde from the tip of the toe, centrally across the distal and proximal interphalangeal joints, across the reduced MTP joint, and deeply into the metatarsal shaft. This K-wire acts as an internal splint, neutralizing deforming forces while the soft tissues heal. A meticulously applied compressive forefoot dressing is then utilized to maintain alignment, splint the digit, and control postoperative edema.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and adherence to sequential release protocols, complications following the correction of severe hammer toe and MTP joint deformities remain a significant clinical reality. The complex interplay of altered biomechanics, compromised soft tissue envelopes, and patient non-compliance creates an environment ripe for postoperative challenges. A comprehensive understanding of these potential pitfalls is essential for the operating surgeon to counsel patients accurately and to intervene rapidly when complications arise.
One of the most frequent and frustrating complications is the "floating toe" syndrome. This occurs when the toe fails to purchase the ground during the stance phase of gait, resting in a persistently elevated position. The etiology is typically iatrogenic: over-lengthening of the extensor apparatus, excessive release of the plantar plate or collateral ligaments, or failure to address intrinsic muscle weakness. While asymptomatic in some patients, a severe floating toe can cause shoe-wear difficulty and transfer metatarsalgia to adjacent rays. Salvage management often requires a flexor-to-extensor tendon transfer (Girdlestone-Taylor procedure) to actively plantarflex the proximal phalanx and restore ground purchase.
Recurrent deformity is another major concern, particularly in cases of severe, chronic dislocation where the soft tissues have lost their innate elasticity. Under-releasing the dorsal contracture, failing to adequately decompress the joint via an osseous procedure (like a Weil osteotomy), or premature removal of the K-wire fixation can all lead to rapid recurrence. If the deformity recurs and becomes rigid and painful, salvage options become limited. A revision Weil osteotomy with more aggressive shortening, or in severe, end-stage cases, a syndactylization to the adjacent stable digit or even amputation may be considered as a last resort.
Vascular compromise is the most devastating immediate postoperative complication. The "white toe" indicates arterial insufficiency, often caused by excessive tension on the digital arteries following the reduction of a chronically shortened toe, or vasospasm from aggressive dissection. Immediate management includes removing all compressive dressings, placing the foot in a dependent position, and slightly bending the K-wire to relieve tension. If perfusion does not return, the K-wire must be removed entirely, allowing the toe to shorten and restoring blood flow. The "blue toe" indicates venous congestion, which is typically managed by elevation and loosening of tight bandages.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Floating Toe | 10% - 15% | Over-release of plantar plate, excessive EDL lengthening, intrinsic weakness. | Flexor-to-extensor tendon transfer (Girdlestone-Taylor); plantar plate repair. |
| Recurrent Deformity | 5% - 12% | Under-release of dorsal structures, inadequate osseous decompression, early pin removal. | Revision soft tissue release; revision Weil osteotomy; syndactyly. |
