Masterclass: Flexor-to-Extensor Tendon Transfer for Flexible Hammer Toe Deformity

Key Takeaway
Join us in the OR for a masterclass on flexor-to-extensor tendon transfer for flexible hammer toe deformity. We'll meticulously cover surgical anatomy, patient positioning, and a step-by-step intraoperative execution. Learn critical pearls, pitfalls, and essential postoperative management for optimal outcomes in this common forefoot pathology.
Comprehensive Introduction and Patho-Epidemiology
Flexible hammer toe deformity represents one of the most ubiquitous and biomechanically complex forefoot pathologies encountered by the orthopedic foot and ankle surgeon. Defined primarily by a flexion deformity at the proximal interphalangeal (PIP) joint and frequently accompanied by a reciprocal hyperextension deformity at the metatarsophalangeal (MTP) joint, this condition fundamentally disrupts the normal kinematic chain of the lesser digits. The distal interphalangeal (DIP) joint may present in a flexed, extended, or neutral posture, depending on the chronicity of the deformity and the specific tendinous imbalances at play. The primary objective of surgical intervention is the restoration of physiological alignment and dynamic balance, thereby alleviating pain, preventing the progression to a rigid deformity, and optimizing the weight-bearing function of the forefoot.
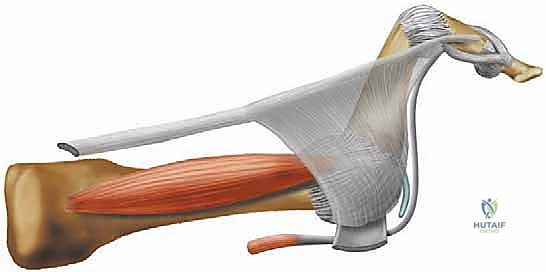
The flexor-to-extensor tendon transfer, historically rooted in the principles described by Girdlestone and Taylor, remains a cornerstone technique in the surgical armamentarium for correcting flexible lesser toe deformities. This procedure is not merely an anatomical repositioning; it is a profound biomechanical realignment. By transferring the deforming force of the flexor digitorum longus (FDL) to the dorsal aspect of the proximal phalanx, the surgeon effectively converts a primary flexor of the PIP joint into a dynamic plantarflexor of the MTP joint. This dynamic stabilization acts to "tape the toe under the skin," neutralizing the hyperextension forces at the MTP joint and allowing the PIP joint to rest in extension.
Epidemiologically, lesser toe deformities disproportionately affect the female population, largely due to the constrictive nature of modern footwear, which frequently features narrow toe boxes and elevated heels. These extrinsic factors force the toes into a buckled position, chronically stretching the plantar plate and shortening the dorsal capsular structures. However, the etiology extends far beyond footwear. Inflammatory arthropathies, such as rheumatoid arthritis, precipitate capsular attenuation and synovial hypertrophy, leading to rapid destabilization. Neuromuscular disorders, including Charcot-Marie-Tooth disease, cerebral palsy, and Friedreich ataxia, induce profound intrinsic-extrinsic muscle imbalances. Furthermore, iatrogenic causes, such as aggressive metatarsal shortening or elevation following osteotomies, can alter the spatial relationship of the metatarsal head, precipitating secondary hammer toe deformities. Understanding this diverse patho-epidemiology is critical, as the underlying cause directly dictates the anticipated success and longevity of the tendon transfer.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of the intricate anatomy of the lesser toes is the bedrock upon which successful surgical correction is built. The stability and function of the lesser digits are governed by a delicate, synergistic balance between extrinsic musculature, intrinsic musculature, and static ligamentous restraints. The extrinsic extensors include the extensor digitorum longus (EDL) and the extensor digitorum brevis (EDB). The EDL tendon is the primary extensor of the MTP joints of the lateral four toes. The EDB, the sole dorsal intrinsic muscle, provides tendinous contributions to the medial four toes. These tendons coalesce and are enveloped by the fibroaponeurotic extensor hood. The proximal segment of this hood, the extensor sling, encircles the MTP joint, attaching to the plantar base of the proximal phalanx and receiving vital contributions from the interossei. The distal segment, the extensor wing, serves as the insertion point for the lumbrical muscles.

The extrinsic flexors, comprising the flexor digitorum brevis (FDB) and flexor digitorum longus (FDL), act as the primary deforming forces in the setting of intrinsic weakness. The FDB tendon bifurcates to insert at the base of the middle phalanx, functioning as the primary flexor of the PIP joint. The FDL tendon passes through the bifurcation of the FDB to insert at the base of the distal phalanx, flexing both the PIP and DIP joints. Crucially, both the FDL and FDB are relatively weak flexors of the MTP joint compared to their profound effect on the interphalangeal joints. The intrinsic flexors—the lumbricals and interossei—are the true modulators of toe posture. Originating from the FDL tendons, the lumbricals travel plantar to the deep transverse metatarsal ligament to insert on the medial aspect of the extensor wing. They act to flex the MTP joints and extend the interphalangeal joints. The interossei, traveling dorsal to the deep transverse metatarsal ligament, are weaker extensors of the toes but play a critical role in transverse plane stability.
The static stabilizers form the final line of defense against deformity. The plantar plates are thick, fibrocartilaginous structures originating from the metatarsal neck periosteum and inserting firmly onto the plantar base of the proximal phalanx. They resist dorsal translation and hyperextension of the proximal phalanx. The collateral ligaments, originating from the metatarsal head and inserting into the base of the proximal phalanx and the margins of the plantar plate, provide varus and valgus stability.
The pathogenesis of a hammer toe deformity represents a cascade of biomechanical failures, classically termed an "intrinsic minus" state. When intrinsic muscle function diminishes—whether due to neuropathy, trauma, or chronic attenuation—the extrinsic extensor tendons (EDL, EDB) overpower the MTP joint, driving it into hyperextension. Once the MTP joint is hyperextended, the long flexor tendons (FDL, FDB) are placed under increased tension and gain an overwhelming mechanical advantage at the PIP and DIP joints, driving them into rigid flexion. Furthermore, as the MTP joint hyperextends, the interosseous tendons subluxate dorsally to the axis of rotation of the metatarsal head, converting them from plantarflexors to aberrant dorsiflexors, thereby exacerbating the deformity. The lumbricals, simultaneously stretched and mechanically disadvantaged, lose their ability to extend the PIP joint. Over time, the plantar plate undergoes chronic repetitive microtrauma, eventually attenuating or rupturing, which solidifies the MTP hyperextension and allows the deformity to transition from flexible to rigid.
Exhaustive Indications and Contraindications
The decision to perform a flexor-to-extensor tendon transfer hinges entirely on a meticulous clinical examination, specifically the assessment of deformity flexibility. This procedure is a dynamic soft-tissue balancing technique; therefore, it requires mobile joints to be effective. If the joints are rigidly contracted, soft-tissue transfers alone will fail, necessitating osseous intervention such as arthrodesis or resection arthroplasty.
The primary indication is a symptomatic, flexible hammer toe deformity characterized by dynamic PIP flexion and MTP hyperextension that has proven refractory to conservative management (e.g., shoe wear modifications, orthoses, toe sleeves). It is also highly indicated as an adjunctive procedure during the correction of crossover toe deformities or multidirectional MTP joint instability, where the transferred tendon provides a robust, dynamic plantarflexion force to stabilize the proximal phalanx against the metatarsal head. Furthermore, in cases where a Weil metatarsal shortening osteotomy is performed, a flexor-to-extensor transfer is frequently indicated to counteract the iatrogenic plantarflexion of the intrinsic muscle line of pull, thereby preventing the dreaded "floating toe" complication.
Contraindications must be strictly observed to prevent catastrophic surgical failures. The absolute contraindication is a rigid, fixed deformity of the PIP or MTP joint. In such scenarios, the transferred tendon cannot overcome the osseous and severe capsular contractures, and attempting to do so will result in persistent deformity and recurrent pain. Severe spasticity, such as that seen in unmanaged cerebral palsy or severe stroke sequelae, is a relative to absolute contraindication, as unpredictable muscle firing will overpower the transfer. Active localized or systemic infection, severe peripheral vascular disease (where digital ischemia is a risk), and profound peripheral neuropathy (where the patient lacks protective sensation and cannot participate in rehabilitation) represent significant contraindications.
| Category | Specific Conditions | Rationale / Clinical Context |
|---|---|---|
| Primary Indications | Flexible Hammer Toe | Dynamic correction of PIP flexion and MTP hyperextension. |
| Flexible Claw Toe | Restores intrinsic balance; often combined with MTP releases. | |
| Dynamic Crossover Toe | Stabilizes the MTP joint against dorsal and transverse subluxation. | |
| Adjunct to Weil Osteotomy | Prevents the "floating toe" phenomenon by providing dynamic plantarflexion. | |
| Absolute Contraindications | Rigid/Fixed Deformity | Soft tissue transfer cannot overcome osseous/capsular contracture; requires arthrodesis. |
| Active Infection | High risk of deep space infection and failure of tendon integration. | |
| Severe Ischemia (PVD) | Surgical trauma and tourniquet use may precipitate digital necrosis or gangrene. | |
| Relative Contraindications | Severe Spasticity | Unpredictable muscle tone will overpower the tendon transfer over time. |
| Profound Neuropathy | Lack of protective sensation increases risk of unrecognized postoperative complications. | |
| Prior FDL Resection | Absence of the necessary donor tendon; requires alternative salvage techniques. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning begins with a rigorous physical examination to quantify the flexibility of the deformity. The "push-up test" (or Kelikian push-up test) is paramount. By applying upward pressure to the plantar aspect of the metatarsal head, the surgeon assesses the reciprocal response of the digits. If the MTP joint plantarflexes and the PIP joint extends to a neutral, physiological alignment, the deformity is deemed flexible, and the patient is an ideal candidate for a tendon transfer. If the deformity only partially corrects, it is semi-flexible, likely requiring concomitant aggressive capsular releases. If it remains unchanged, the deformity is rigid. MTP joint stability is further evaluated using the dorsal drawer (Lachman) test, graded from Stage 0 (stable) to Stage 3 (fixed dislocation). A meticulous neurovascular examination is mandatory, documenting palpable pulses, capillary refill, and protective sensation. Correcting a chronic deformity places previously contracted neurovascular bundles under acute tension; pre-existing compromise significantly elevates the risk of postoperative ischemic necrosis.
Radiographic evaluation requires standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. On the AP view, the surgeon must scrutinize the MTP joints for transverse plane deviation, joint space narrowing, and the "gun barrel" sign, which indicates severe dorsal subluxation or dislocation of the proximal phalanx over the metatarsal head. The lateral view is critical for assessing the degree of MTP hyperextension and PIP flexion, as well as evaluating the metatarsal cascade. While MRI is rarely indicated for a standard hammer toe, it may be utilized if a concomitant plantar plate tear or subtle intermetatarsal neuroma is suspected, though clinical examination usually suffices. Pre-operative templating involves anticipating the need for concurrent procedures, such as a Weil osteotomy for an excessively long metatarsal or a PIP resection arthroplasty if intraoperative assessment reveals unexpected rigidity.

Patient positioning and operating room setup are critical for procedural efficiency and optimal outcomes. The patient is placed in the supine position. A bump may be placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a perfectly neutral position relative to the ceiling, which is particularly helpful for lateral column procedures.

The operative extremity must be prepped and draped to above the knee. Crucially, the foot must be positioned at the very edge of the operating table, or the distal end of the table must be removed or lowered. This allows the surgeon to stand directly at the foot of the bed, providing an unobstructed, axial view of the metatarsal cascade and facilitating comfortable manipulation of the digits. A pneumatic tourniquet is highly recommended to ensure a bloodless field, which is essential for identifying the delicate fascial planes and tendinous slips. Depending on surgeon preference and concomitant procedures, an ankle, calf, or thigh tourniquet may be utilized, typically inflated to 250-300 mmHg after exsanguination with an Esmarch bandage.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Exposure
The surgical approach for a flexor-to-extensor tendon transfer can be performed via a single dorsal longitudinal incision, a transverse dorsal incision, or a dual-incision technique (plantar and dorsal). For the purpose of this masterclass, we will detail the highly versatile dorsal longitudinal approach, which provides exceptional visualization of the extensor mechanism, the MTP joint, and the PIP joint.
A longitudinal incision is made centered over the dorsal aspect of the proximal phalanx, extending from the MTP joint to the distal interphalangeal (DIP) joint. The incision is carried through the epidermis and dermis. Meticulous blunt dissection utilizing tenotomy scissors is employed to spread the subcutaneous tissues, carefully identifying and retracting the dorsal cutaneous nerve branches and dorsal venous tributaries. The extensor apparatus is systematically exposed.

At this juncture, if MTP joint hyperextension is present, a Z-lengthening or transverse tenotomy of the EDL tendon is performed. Following this, a dorsal capsulotomy of the MTP joint is executed. If the joint remains tight, sequential release of the collateral ligaments is performed by passing a localized blade between the metatarsal head and the base of the proximal phalanx, carefully detaching the ligaments from their metatarsal origins until the proximal phalanx can be smoothly plantarflexed.
Tendon Harvest and Preparation
Attention is then directed to the harvesting of the FDL tendon. Through the dorsal incision, the surgeon dissects bluntly along the lateral and medial margins of the proximal phalanx to access the plantar compartment. Alternatively, a small transverse plantar incision at the proximal flexion crease of the toe can be utilized for direct access.

The flexor tendon sheath is identified and incised longitudinally. The FDL tendon is identified; it is the deeper, more central tendon that passes through the bifurcation of the FDB tendon. The FDL tendon is traced as far distally as possible, ideally to its insertion at the base of the distal phalanx. A small right-angle retractor or a Freer elevator is used to hook the FDL tendon. The tendon is then transected sharply at its distal insertion. Maintaining tension on the proximal stump of the FDL, the surgeon delivers the tendon into the dorsal wound (if working from a plantar incision) or pulls it proximally within the dorsal wound.

The harvested FDL tendon must now be prepared for transfer. The tendon naturally possesses a central raphe or longitudinal cleavage plane. Using a #15 scalpel blade, the surgeon carefully splits the FDL tendon longitudinally along this raphe, dividing it into two equal medial and lateral slips. This split is carried proximally to the level of the MTP joint, ensuring adequate length for the subsequent transfer around the proximal phalanx.
Tendon Transfer and Routing
With the FDL tendon split into two robust slips, the routing phase begins. The objective is to pass these slips from the plantar aspect of the foot, dorsally around the medial and lateral cortices of the proximal phalanx, to meet over the dorsal extensor hood.
Using a curved hemostat or a specialized tendon passing forceps, the surgeon creates a tunnel hugging the periosteum of the proximal phalanx. The forceps are passed from dorsal to plantar, carefully avoiding the neurovascular bundles which lie slightly more plantar and lateral/medial.

The lateral slip of the split FDL is grasped and pulled dorsally along the lateral border of the proximal phalanx. The process is repeated on the medial side, grasping the medial slip and pulling it dorsally along the medial border. Both slips are now positioned dorsally, effectively creating a tendinous sling cradling the plantar aspect of the proximal phalanx.
Tensioning and Fixation
The tensioning of the transfer is the most critical step of the procedure, dictating the ultimate biomechanical success. The ankle must be held in a strictly neutral position (90 degrees). The MTP joint is manually held in approximately 10 to 15 degrees of plantarflexion, and the PIP joint is held in full extension.

With the toe held in this overcorrected position, the two slips of the FDL are pulled dorsally and crossed over the proximal phalanx and the extensor hood. The tension applied should be firm but not strangulating.

The slips are then sutured to each other, to the underlying extensor mechanism (EDL/extensor hood), and to the periosteum of the proximal phalanx using multiple interrupted sutures of 3-0 or 4-0 non-absorbable braided material (e.g., Ethibond or FiberWire). The surgeon must ensure the repair is robust enough to withstand early postoperative mobilization.
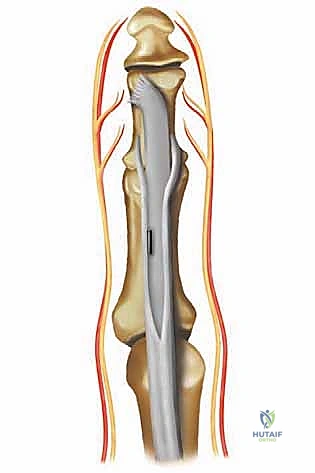
While a purely flexible deformity corrected with a tendon transfer may not strictly require osseous stabilization, it is standard academic practice to temporarily pin the toe to protect the soft tissue repair during the initial healing phase. A 0.045-inch or 0.062-inch Kirschner wire (K-wire) is driven antegrade from the PIP joint out the tip of the toe, then driven retrograde across the PIP joint, the proximal phalanx, and across the MTP joint into the metatarsal shaft. The pin is left protruding from the tip of the toe and capped. The tourniquet is deflated, hemostasis is meticulously achieved, and the skin is closed with 4-0 or 5-0 non-absorbable monofilament sutures in a simple interrupted or horizontal mattress fashion. A bulky, compressive soft dressing is applied.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following flexor-to-extensor tendon transfers can occur and must be anticipated. The most frequent complication is the "floating toe" phenomenon, where the toe fails to purchase the ground during the stance phase of gait. This is often due to inadequate tensioning of the transfer, over-lengthening of the EDL, or concurrent aggressive metatarsal shortening (Weil osteotomy) without sufficient plantarflexion correction. Recurrent deformity is another significant risk, particularly if the procedure was erroneously performed on a semi-rigid or rigid deformity, or if the patient has an underlying progressive neuromuscular disorder.
Postoperative stiffness of the PIP and MTP joints is nearly universal to some degree, secondary to surgical scarring and prolonged immobilization. While mild stiffness is often well-tolerated and may even prevent recurrence, severe stiffness can be painful and limit footwear options. Vascular compromise is the most devastating acute complication. Aggressive correction of a chronic deformity can place the digital arteries under extreme tension, leading to vasospasm or intimal tear. If the toe appears dusky, white, or lacks capillary refill upon tourniquet deflation and pinning, the K-wire must be immediately withdrawn to reduce tension. If perfusion does not return, all sutures must be released, and the toe allowed to assume a slightly deformed but perfused position.
Infection, while relatively rare (1-3%), can occur, particularly around the percutaneous K-wire (pin tract infection). Superficial infections are managed with oral antibiotics and local wound care, while deep space infections require immediate hardware removal, surgical debridement, and intravenous antibiotics.
| Complication | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|
| Floating Toe | 10% - 15% | Conservative: Metatarsal pads, taping. Surgical: Revision transfer, MTP plantar capsulorrhaphy, or flexor tendon tethering. |
| Recurrent Deformity | 5% - 10% | Indicates failure of soft tissue balancing. Salvage requires osseous intervention: PIP arthrodesis and MTP capsular release. |
| Joint Stiffness | 20% - 30% | Aggressive physical therapy, passive stretching. Severe cases may require surgical arthrolysis (rarely indicated). |
| Vascular Compromise | < 1% | Immediate removal of K-wire, release of surgical tension, application of warm saline, dependent positioning. Amputation if irreversible. |
| Pin Tract Infection | 2% - 5% | Oral antibiotics, more frequent dressing changes. Early removal of the K-wire if the infection tracks deeply. |
| **Nerve Injury (Neuroma |
