Comprehensive Introduction and Patho-Epidemiology
The combined hammer toe and mallet toe deformity, frequently presenting with associated double corns, represents a distinct and highly complex biomechanical entity in forefoot pathology. It differs fundamentally from the traditional claw toe deformity in that there is minimal to no extension deformity at the metatarsophalangeal (MTP) joint. Instead, the primary deforming forces are concentrated distally, resulting in rigid, unyielding flexion contractures at both the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. This dual-level contracture fundamentally alters the weight-bearing and shoe-wear mechanics of the forefoot, converting the normally supple digits into rigid levers that are subjected to immense, localized shear and compressive forces.
Because of this rigid, multi-segmental contracture, the affected toe is subjected to abnormal mechanical stresses within the confined space of the shoe toe box. Large, prominent hyperkeratotic lesions—clinically referred to as double corns—typically develop over the dorsal aspects of both the PIP and DIP joints. The management of these lesions requires a deep, three-dimensional understanding of the underlying osseous prominences and the dynamic soft-tissue imbalances driving the deformity. In a landmark retrospective review of combined DIP and PIP resection arthroplasties, Oliver et al. reported a 10% recurrence rate at the PIP joint, which they attributed directly to inadequate bone resection during the index procedure, underscoring the necessity of aggressive osseous decompression.

Epidemiologically, corns (helomata and clavi) represent a hypertrophic response of the stratum corneum—the horny layer of the epidermis—to repetitive mechanical stress. This hyperkeratosis is a physiological defense mechanism gone awry, driven by the unyielding pressure of a phalangeal condyle beneath the skin and the rigid constraints of footwear externally. Over time, this localized thickening becomes an avascular, dense plug of keratin that focuses pressure directly onto the underlying sensitive dermal layers and periosteum, generating exquisite pain. The prevalence of these lesions is markedly higher in populations with structural forefoot abnormalities, such as hallux valgus, inflammatory arthropathies, and neuromuscular disorders that disrupt the delicate balance of the intrinsic and extrinsic musculature.
The clinical burden of these combined deformities is substantial, particularly in patients with compromised sensibility or peripheral perfusion. In the neuropathic or diabetic foot, what begins as a simple mechanical hyperkeratosis can rapidly degenerate into a full-thickness ulceration. The dense keratin plug acts as a foreign body, causing pressure necrosis of the underlying subcutaneous tissue. Left untreated, this cascade reliably progresses to deep space infection, septic arthritis of the interphalangeal joints, and osteomyelitis, rendering a seemingly benign structural deformity a true limb-threatening emergency.
Detailed Surgical Anatomy and Biomechanics
The osseous anatomy of the lesser toes dictates the specific locations and presentations of hyperkeratotic lesions. Each lesser toe typically comprises a proximal, middle, and distal phalanx, with the exception of the fifth toe, which frequently presents as a two-boned variant due to synostosis of the middle and distal phalanges. The phalangeal heads are bicondylar, with the lateral and medial condyles often exhibiting asymmetric prominence. Specifically, the dorsolateral aspect of the PIP joint of the fifth toe and the lateral flare of the base of the fourth proximal phalanx are notorious for their prominent profiles, making them prime epicenters for pressure-induced pathology.
The soft-tissue constraints and musculotendinous balance of the lesser toes involve a complex interplay between the extrinsic and intrinsic muscle groups. The extrinsic extensors (extensor digitorum longus and brevis) insert via the extensor hood mechanism, primarily extending the MTP joint. The extrinsic flexors (flexor digitorum longus and brevis) insert on the distal and middle phalanges, respectively. The intrinsic muscles (lumbricals and interossei) pass plantar to the MTP joint axis but dorsal to the interphalangeal joint axes, functioning to flex the MTP and extend the PIP and DIP joints. A combined hammer and mallet toe deformity arises when this delicate balance is disrupted, typically driven by an overpowering of the extrinsic flexors over a weakened or mechanically disadvantaged intrinsic system, leading to isolated PIP and DIP flexion without MTP hyperextension.
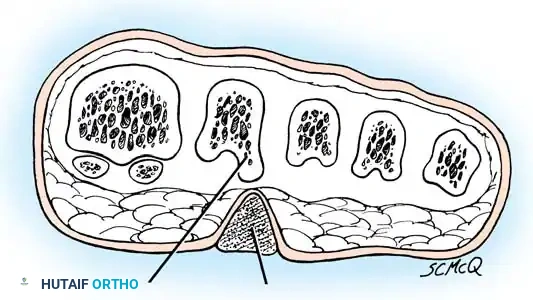
Biomechanically, the interdigital spaces are subjected to a unique set of forces that predispose them to soft corns (heloma molle). The "pincer" effect is the primary biomechanical driver in the fourth web space. This occurs when the lateral side of the base of the fourth proximal phalanx abuts the medial condyle of the head of the fifth proximal phalanx. This bony impingement is frequently exacerbated by an abnormally short fifth metatarsal or a concomitant hallux valgus deformity, which laterally displaces the lesser toes and increases adduction pressure from the shoe. The resulting friction in the moist, confined environment of the web space leads to maceration and the characteristic soft, boggy appearance of an interdigital corn.

Plantar corns, or intractable plantar keratoses (IPK), represent another biomechanical failure, typically occurring beneath the metatarsal heads. The fibular condyle of the lesser metatarsal heads projects more plantarward than the tibial side, creating a focal point of high pressure during the propulsive phase of gait. If the metatarsal parabola is disrupted—such as a long second metatarsal or a hypermobile first ray that transfers load laterally—the localized pressure beneath these condyles exceeds the viscoelastic tolerance of the plantar fat pad. This results in an invaginated plug of dense keratin that acts like a stone in the shoe, causing severe, localized plantar forefoot pain.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for combined hammer and mallet toe deformities with associated corns must be grounded in a thorough exhaustion of conservative modalities. Nonoperative management remains the first-line treatment and includes aggressive shoe wear modification (wide, deep toe boxes), digital sleeves with medical-grade paraffin (Silipos), and meticulous web space hygiene using drying agents and lamb’s wool spacers. Surgery is strictly indicated when these measures fail to relieve intractable pain, when the deformity prevents the patient from wearing standard, commercially available footwear, or when there is impending or recurrent skin breakdown that threatens the viability of the digit.
Specific morphological presentations dictate nuanced surgical indications. Hard corns (heloma durum) that are rigidly fixed and exquisitely tender require osseous decompression, typically via condylectomy or formal resection arthroplasty of the PIP joint. Soft corns (heloma molle) located in the fourth web space that fail to respond to drying agents and spacers necessitate the surgical removal of the underlying bony conflict (the "pincer" effect) or a partial syndactylization to obliterate the friction interface. Plantar corns (intractable plantar keratoses) that are refractory to offloading orthotics require metatarsal osteotomies or plantar condylectomies to elevate and decompress the offending metatarsal head.
Contraindications to elective forefoot reconstruction must be rigorously respected to avoid catastrophic complications. Absolute contraindications include active, untreated infection (unless the surgery is a therapeutic debridement or amputation for an infected corn), severe peripheral vascular disease (PVD) with inadequate absolute toe pressures or transcutaneous oxygen tension (TcPO2 < 30 mmHg), and an inadequate soft-tissue envelope that precludes primary healing. Relative contraindications include poorly controlled diabetes mellitus (HbA1c > 8.0%), heavy tobacco use, and patient non-compliance, as the postoperative rehabilitation phase requires strict adherence to weight-bearing restrictions and splinting protocols.
In the diabetic or immunocompromised patient, the presence of an infected soft corn radically alters the treatment algorithm. This is no longer an elective deformity correction; it is a limb-salvage scenario. An infected soft corn can rapidly progress to deep space infection, tracking along the flexor tendon sheaths, leading to osteomyelitis and catastrophic tissue loss. In these instances, primary closure is absolutely contraindicated, and the surgical focus shifts entirely to aggressive radical debridement, open drainage, and potential ray resection, guided by deep tissue cultures and targeted antimicrobial therapy.
| Category | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Status | Intractable pain failing >6 months of conservative care; Impending ulceration; Recurrent infections. | Active local infection (for elective correction); Poorly controlled diabetes (HbA1c > 8.0%). |
| Vascular Status | Palpable pedal pulses; ABI > 0.8; TcPO2 > 40 mmHg. | Severe PVD; Absent pulses with ABI < 0.5; TcPO2 < 30 mmHg; Ischemic rest pain. |
| Lesion Type | Rigid hard corns; Recurrent soft corns; Intractable plantar keratosis (IPK); Neurovascular corns. | Simple callosities responsive to paring; Plantar warts (verruca plantaris - requires dermatologic tx). |
| Patient Factors | Compliant with post-op protocols; Realistic expectations regarding swelling and cosmesis. | Active smoking (relative); Non-ambulatory status (unless for infection control); Severe psychiatric illness. |


Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a meticulous clinical examination to differentiate the precise etiology of the forefoot pain. The surgeon must carefully palpate the bony prominences to map the exact location of the osseous conflict. The Kelikian push-up test is utilized to determine the flexibility or rigidity of the MTP and interphalangeal joints, which dictates whether a soft-tissue procedure (e.g., flexor tenotomy) will suffice or if definitive bone resection is required. Furthermore, the surgeon must definitively differentiate neurovascular corns from plantar warts; gentle paring of the lesion with a #15 scalpel is diagnostic. Paring a wart reveals vertical blood vessels presenting as punctate bleeding points, whereas paring a corn reveals layers of clear, avascular keratin or, in the case of a neurovascular corn, blood vessels parallel to the plantar surface.
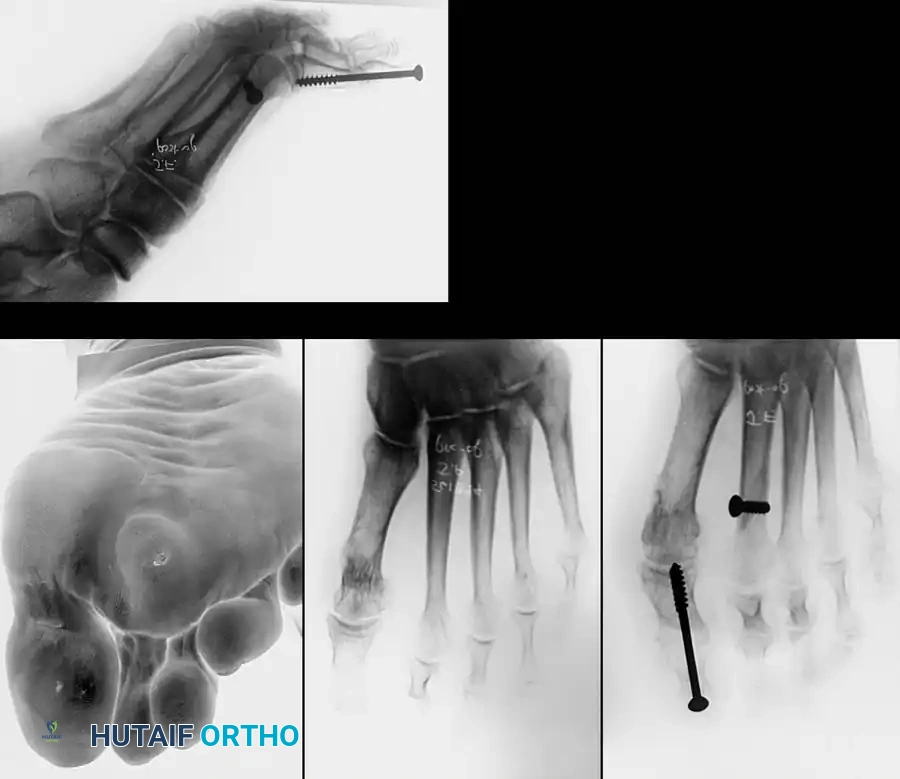
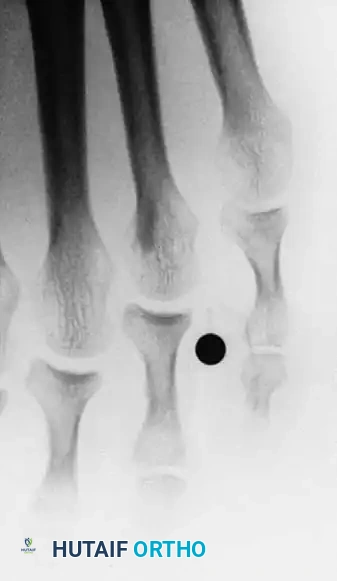
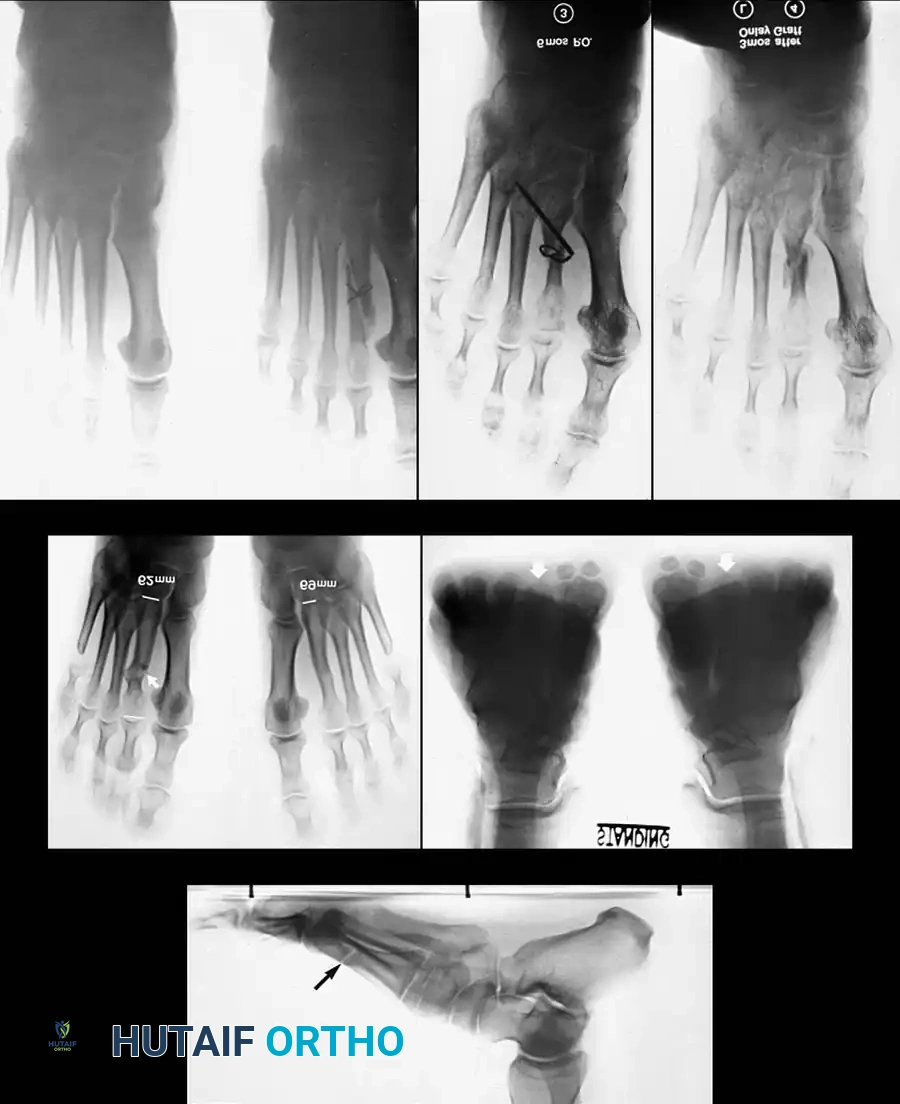
Radiographic evaluation is mandatory and must include weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. These images allow the surgeon to assess the metatarsal parabola, identify joint subluxations, and evaluate the specific bony exostoses causing the corns. In the setting of a fourth web space soft corn, the AP and oblique views are critical for identifying the apposition of the base of the fourth proximal phalanx and the head of the fifth proximal phalanx. Additionally, the surgeon should evaluate the length of the fifth metatarsal, as an abnormally short fifth metatarsal frequently exacerbates the pincer effect in the web space.
Preoperative templating involves determining the precise amount of bone resection required to achieve adequate decompression without rendering the toe flail. For a rigid combined hammer and mallet toe, the surgeon must plan for a resection arthroplasty of the PIP joint and potentially the DIP joint. If a syndactylization is planned for a recurrent soft corn, the skin incisions must be mapped to ensure adequate excision of the macerated web space skin while preserving sufficient viable tissue for a tension-free closure. The surgeon must also counsel the patient extensively regarding the expected cosmetic outcome, emphasizing that the primary goal is a painless, functional, and shoe-able foot, not necessarily a perfectly straight or aesthetically flawless digit.
Patient positioning is supine on the operating table. The choice of anesthesia depends on the extent of the planned procedures and patient comorbidities. For isolated digital procedures, a local digital block using a mixture of short- and long-acting local anesthetics (without epinephrine) is often sufficient. For multi-digit reconstructions or metatarsal osteotomies, a regional ankle block or general anesthesia is preferred. A sterile digital tourniquet, such as a rolled Penrose drain or a commercial digital tourniquet, is applied at the base of the toe to provide a bloodless surgical field. The surgeon must strictly monitor tourniquet time, ensuring it does not exceed 20-30 minutes, to prevent irreversible ischemic injury to the digit.

Step-by-Step Surgical Approach and Fixation Technique
Resection Arthroplasty for Hard Corns and Combined Deformities
The surgical management of a hard corn, particularly over the dorsolateral aspect of the PIP joint of the fifth toe, requires meticulous technique to ensure complete eradication of the bony prominence. Following the administration of a digital block and application of a sterile tourniquet, a dorsolateral longitudinal incision is made, carefully skirting the medial border of the corn. The incision begins 5 to 6 mm proximal to the nail fold and extends proximally for approximately 1.5 cm. The dissection is deepened through the subcutaneous tissue, with strict attention paid to identifying and retracting the dorsal cutaneous nerve branches to prevent painful postoperative neuromas.
The extensor tendon is identified and retracted medially, or longitudinally split, to expose the PIP joint capsule. A transverse capsulotomy is performed to expose the head of the proximal phalanx and the base of the middle phalanx. Using a small sagittal saw or a sharp rongeur, the bony prominence on the dorsolateral aspect of the condyle of the proximal phalanx is resected. For rigid combined hammer and mallet toe deformities, a simple condylectomy is often insufficient and carries a high recurrence rate. In these cases, a formal resection arthroplasty (hammer toe repair) is executed by resecting the entire head and neck of the proximal phalanx.
Intraoperative assessment of the resection is critical. Visual inspection alone is notoriously deceptive in the confined space of the digit; the surgeon must meticulously palpate the resected area to ensure absolutely no sharp bony prominences remain. If the DIP joint is also rigidly contracted (mallet deformity), a similar resection arthroplasty of the middle phalangeal head is performed via a separate dorsal transverse or longitudinal incision. Following adequate bone resection, the toe is stabilized. While some surgeons rely on soft-tissue closure and postoperative taping, the use of a 0.045-inch or 0.062-inch smooth Kirschner wire driven from distal to proximal across the DIP and PIP joints provides superior stabilization of the pseudoarthrosis during the initial healing phase.

Bony Decompression and Partial Syndactylization for Soft Corns
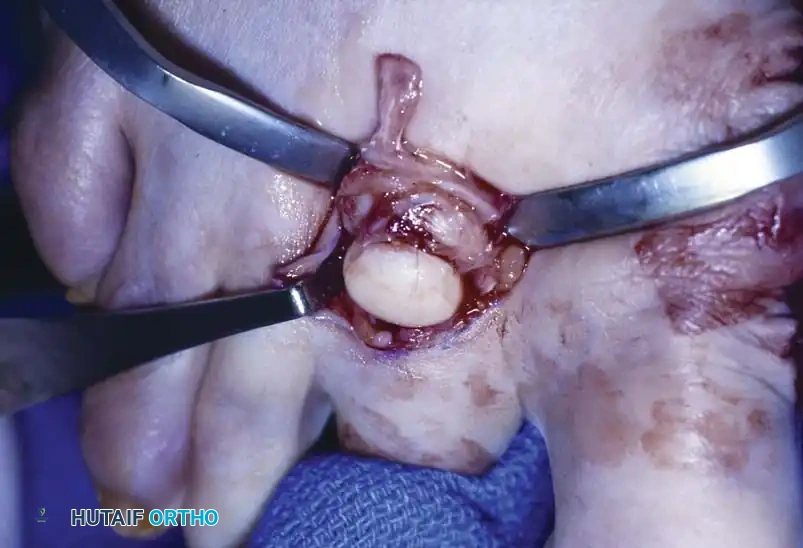
Soft corns in the fourth interdigital space are addressed by eliminating the underlying "pincer" effect. A dorsal longitudinal incision is made extending into the plantar portion of the interdigital space. If the center of the hyperkeratotic area is biased toward the fourth toe, the lateral flare of the base of the proximal phalanx of the fourth toe is resected flush with the diaphysis. If the lesion is biased toward the fifth toe, the medial portion of the head of the proximal phalanx of the fifth toe is resected. The web space is then palpated dynamically; if residual impingement exists when the toes are compressed together, the opposite bony offender must also be resected.
For recurrent, intractable interdigital corns, or when the web space skin is severely compromised, a partial simple syndactylization is the definitive procedure. The incision design is critical: a dorsal longitudinal incision extends into the plantar interdigital space, with the two limbs diverging onto the adjacent plantar sides of the opposing toes. This specific placement retains a cosmetic dorsal cleft. The intervening skin, including the corn and any macerated tissue, is sharply excised.

Following the necessary bony resections (as described above), the syndactylization is closed. Closure begins proximally in the web space and extends distally. The deep subcutaneous tissues are approximated with absorbable sutures to eliminate dead space, and the dorsal and plantar skin edges are meticulously aligned and sutured with non-absorbable monofilament. This procedure completely obliterates the friction interface between the toes, offering a highly reliable, permanent solution to the interdigital soft corn.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the correction of combined hammer/mallet toes and associated corns can occur and must be managed aggressively. Recurrence of the deformity and the hyperkeratotic lesions is the most common complication. Oliver et al. reported a 10% recurrence rate at the PIP joint, which is almost universally attributed to inadequate primary bone resection. If a simple condylectomy fails, salvage management requires returning to the operating room for a formal, aggressive resection arthroplasty of the proximal phalangeal head and neck, coupled with stabilization via K-wire fixation or a digital implant.
Infection and wound healing issues present a significant challenge, particularly in the diabetic or vasculopathic population. The thin soft-tissue envelope of the digits provides minimal barrier to infection. A superficial wound dehiscence can rapidly progress to deep space infection and osteomyelitis of the retained phalangeal segments. In these scenarios, the presence of an infected soft corn with lytic changes on radiography mandates immediate surgical intervention. Salvage involves aggressive sharp debridement of all necrotic bone and soft tissue, prolonged culture-directed intravenous antibiotic therapy, and frequently, partial or complete ray amputation to achieve a definitive cure and prevent proximal spread.

Vascular compromise, presenting as a "white toe" immediately postoperatively, is a surgical emergency. This can result from excessive traction on the neurovascular bundles during severe deformity correction, overly tight closure, or arterial tethering by a K-wire. Immediate management involves placing the foot in a dependent position, applying warm compresses to the ipsilateral popliteal fossa to induce reflex vasodilation, loosening all dressings, and removing any sutures that may be causing tension. If the digit remains ischemic, any indwelling K-wires must be backed out or removed entirely. If perfusion is not restored, an immediate vascular surgery consultation is required, though the prognosis for the digit in prolonged ischemia is poor, often culminating in amputation.
Over-resection of the proximal phalanx can lead to a "flail toe"—a shortened, unstable, and functionally useless digit that retracts dorsally or deviates laterally. This complication causes significant patient dissatisfaction due to both functional impairment and poor cosmesis. Salvage of a flail toe is exceptionally difficult. Options include syndactylization of the flail digit to the adjacent stable toe to provide soft-tissue support, or, in severe cases, bone grafting and formal arthrodesis of the PIP joint, though the latter is technically demanding given the compromised soft-tissue envelope and poor bone stock.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management |
|---|---|---|---|
| Recurrent Corn/Deformity | 5 - 10% | Inadequate bone resection; unrecognized dynamic imbalance. | Revision resection arthroplasty; aggressive condylectomy; K-wire stabilization. |
| Flail Toe / Instability | 2 - 5% | Over-resection of proximal phalangeal head/neck; failure to splint. | Syndactylization to adjacent digit; bone block arthrodesis. |
| Vascular Compromise | < 1% | Excessive tension; K-wire tethering; unrecognized PVD. | Remove dressings/sutures/pins; dependent positioning; potential amputation. |
| Deep Infection / Osteomyelitis | 1 - 3% (Higher in DM) | Operating through macerated/ulcerated tissue; poor hygiene. | Radical debridement; IV antibiotics; partial/complete ray amputation. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is phased and requires
Clinical & Radiographic Imaging Archive