Comprehensive Introduction and Patho-Epidemiology
The terms hammer toe and claw toe describe complex, multi-planar deformities of the lesser digits that are frequently encountered by the practicing orthopedic surgeon. While these terms are occasionally conflated in general medical practice, they represent entirely distinct pathoanatomical entities with divergent etiologies, biomechanical drivers, and surgical reconstructive algorithms. Understanding the nuanced differences between these deformities is paramount, as an inaccurate diagnosis will inevitably lead to an inappropriate surgical strategy and subsequent clinical failure. The lesser toes play a crucial role in the terminal stance phase of the gait cycle, expanding the weight-bearing surface area of the forefoot and assisting in balance and propulsion. Disruption of this delicate anatomical arrangement leads to significant morbidity, functional limitation, and profound pain.
A hammer toe is primarily characterized by an abnormal, isolated flexion posture of the proximal interphalangeal (PIP) joint of one of the lesser four toes. This flexion deformity exists on a spectrum of rigidity and may present as flexible (passively correctable to a neutral anatomical position) or fixed (rigid, with capsuloligamentous contracture preventing passive correction). In severe, chronic cases of hammer toe deformity, the metatarsophalangeal (MTP) joint frequently deforms in the opposite direction, assuming a compensatory extension posture due to the retrograde buckling force exerted by the proximal phalanx. The distal interphalangeal (DIP) joint typically remains supple in the early stages but may secondarily develop a compensatory flexion or extension deformity depending on the chronicity of the condition and the specific footwear utilized by the patient.

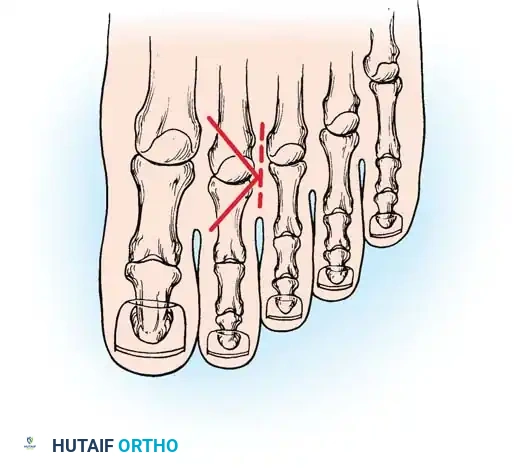
Conversely, a claw toe is defined by a rigid triad of synchronous deformities: hyperextension at the MTP joint, flexion at the PIP joint, and flexion at the DIP joint. Claw toes are frequently bilateral, typically involve all lesser toes simultaneously, and are highly indicative of an underlying systemic neuromuscular disorder. The epidemiology of these deformities reveals a strong predilection for the female population, largely driven by the use of restrictive, narrow toe-box footwear with elevated heels. Hammer toes most commonly affect the second digit, particularly in patients with a Morton's foot structure (a second metatarsal that is longer than the first) or in the presence of severe hallux valgus, where the drifting great toe physically crowds and under-rides or over-rides the adjacent second toe.

To ensure accurate surgical planning, the orthopedic surgeon must meticulously differentiate these deformities based on clinical hallmarks. Etiologically, claw toes are frequently driven by neuromuscular diseases such as Charcot-Marie-Tooth disease, diabetic peripheral neuropathy, spinal dysraphism, or late-stage compartment syndrome. Hammer toes, however, are typically idiopathic or related to extrinsic mechanical factors. Clinically, claw toes usually affect all lesser toes globally, whereas hammer toes typically involve only one or two digits. Furthermore, claw toes universally present with an extension deformity at the MTP joint and a flexion deformity at the DIP joint. In hammer toes, MTP extension is variable, and the DIP joint is generally spared or remains supple.


Detailed Surgical Anatomy and Biomechanics
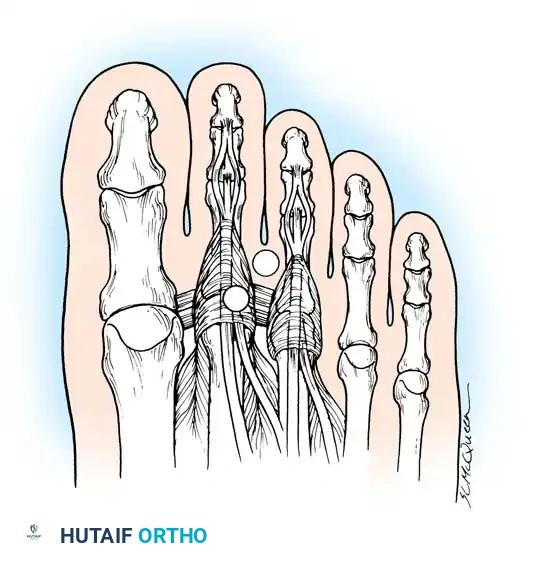
The structural integrity and dynamic function of the lesser toes rely on a highly intricate balance between the extrinsic musculature (originating in the leg) and the intrinsic musculature (originating within the foot), all acting upon a complex capsuloligamentous framework. The primary extrinsic extensors are the extensor digitorum longus (EDL) and the extensor digitorum brevis (EDB). The EDL tendons insert via a trifurcated extensor hood mechanism; the central slip attaches to the base of the middle phalanx, while the lateral bands converge to insert on the base of the distal phalanx. The extrinsic flexors consist of the flexor digitorum longus (FDL), which inserts on the distal phalanx, and the flexor digitorum brevis (FDB), which bifurcates to insert on the middle phalanx. The intrinsic muscles—the lumbricals and the dorsal and plantar interossei—are the critical stabilizers of the MTP joint.
The Intrinsic Minus Foot and Claw Toe Biomechanics
Claw toes represent the classic, quintessential manifestation of an "intrinsic minus" foot. The intrinsic muscles of the foot pass plantar to the axis of rotation of the MTP joint, acting as the primary flexors of the MTP joint and, via their attachments to the extensor wing and sling, as extensors of the interphalangeal (IP) joints. When a systemic neuromuscular disease causes denervation and subsequent loss of intrinsic muscle function, a profound and destructive biomechanical imbalance occurs. The EDL is left entirely unopposed and aggressively hyperextends the MTP joint. Simultaneously, the FDL and FDB exert an unopposed flexion force on the PIP and DIP joints.
A critical clinical pearl in understanding claw toe pathoanatomy is recognizing the functional length-tension relationship of the extrinsic extensors. Although the long extensors of the toes possess the anatomical capacity to extend the IP joints when the MTP joint is held in neutral, they completely lose their mechanical excursion and tension once the MTP joint hyperextends. Consequently, the EDL can no longer extend the IP joints. This mechanical disadvantage allows the powerful FDL (inserting at the base of the distal phalanx) to accentuate and lock in the clawing deformity, creating a rigid, non-yielding structure that is highly susceptible to dorsal ulceration.
Idiopathic Hammer Toe Biomechanics
While the etiology of claw toes is deeply rooted in intrinsic denervation, the vast majority of hammer toes exhibit absolutely no underlying intrinsic muscle imbalance. Seminal electromyographic (EMG) studies conducted by Mann and Inman evaluated the phasic activity of the intrinsic muscles during the normal human gait cycle. Their exhaustive research demonstrated that there is zero intrinsic muscle activity during the first 35% of the gait cycle or during periods of quiet, static standing. Because the hammering of the toes is typically accentuated by standing, the complete absence of intrinsic activity during this phase strongly implies that intrinsic weakness is not the primary biomechanical driver of hammer toe deformities.
Instead, hammer toes are driven by a combination of extrinsic compression, anatomical predispositions, and localized trauma. Long-term use of poorly fitting shoes with a narrow, restrictive toe box physically forces the digits into a buckled, non-anatomical posture. Over years of cyclic loading, this leads to adaptive shortening of the plantar capsule at the PIP joint and elongation of the dorsal structures, culminating in fixed contractures. Anatomical predispositions, such as a "two-bone toe" (congenital synostosis of the PIP or DIP joint), a disproportionately long second ray, or severe hallux valgus, can cause lateral pressure and mechanical buckling of the adjacent second toe. Furthermore, previous trauma, such as unrecognized fractures or localized inflammatory arthropathies like Rheumatoid Arthritis, can disrupt the delicate balance of the extensor hood mechanism, leading to subluxation and eventual deformity.

Exhaustive Indications and Contraindications
The decision to proceed with surgical reconstruction of a hammer toe or claw toe deformity must be predicated on a thorough clinical evaluation and a clear understanding of the patient's symptoms, functional demands, and medical comorbidities. Surgical intervention is indicated strictly for symptomatic deformities that have failed a comprehensive trial of non-operative management. Pain typically localizes to three distinct areas of pathological pressure: the dorsal PIP joint (where a hard corn or heloma durum develops due to friction against the shoe vamp), the tip of the distal phalanx (where a painful end corn develops due to an end-bearing posture), and the plantar metatarsal head (where dorsal subluxation of the proximal phalanx draws the plantar plate distally, exposing the metatarsal head to increased plantar pressure and leading to an intractable plantar keratosis).
In patients with diminished protective sensation, such as those with long-standing diabetes mellitus, advanced peripheral neuropathy, or myelomeningocele, these areas of focal pressure can rapidly and silently progress to full-thickness ulceration, deep space infection, and contiguous osteomyelitis. In this highly vulnerable patient population, surgical intervention is often considered prophylactic rather than purely elective. The goal is to salvage the digit, eradicate the bony prominence, and prevent the cascade of events that ultimately leads to major lower extremity amputation.
Cosmetic dissatisfaction, in the absolute absence of pain or functional impairment, is a strict and absolute contraindication to surgical intervention. The risks of surgery, including neurovascular compromise, infection, stiffness, and the dreaded "floating toe" complication, far outweigh any perceived aesthetic benefit. Furthermore, patients with severe peripheral arterial disease lacking adequate perfusion for incisional healing must undergo vascular optimization prior to any consideration of elective forefoot reconstruction.
| Clinical Parameter | Indications for Surgical Intervention | Contraindications to Surgical Intervention |
|---|---|---|
| Symptomatology | Intractable pain failing conservative care (shoe modification, padding). | Purely cosmetic concerns without pain or functional deficit. |
| Cutaneous Integrity | Recurrent heloma durum, intractable plantar keratosis (IPK), impending ulceration. | Active, untreated cellulitis or deep space soft tissue infection. |
| Neuropathic Status | Prophylactic correction in insensate feet to prevent ulceration/osteomyelitis. | Severe, unmanageable Charcot neuroarthropathy in the acute inflammatory phase. |
| Vascular Status | Adequate perfusion (ABI > 0.8, palpable pulses, biphasic Doppler). | Severe peripheral arterial disease (ABI < 0.5), absent pulses, non-healing ischemic ulcers. |
| Deformity Type | Both flexible (soft tissue procedures) and rigid (osseous procedures) deformities. | Inability to comply with strict post-operative weight-bearing and pin care protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful lesser toe reconstruction. The clinical evaluation must begin with a thorough assessment of the flexibility of the deformity. The Kelikian push-up test is an invaluable clinical maneuver; by applying upward pressure to the plantar aspect of the metatarsal head, the surgeon can determine if the MTP and PIP deformities passively correct. If the deformity corrects, it is deemed flexible, and soft-tissue procedures (such as tendon transfers) may suffice. If the deformity remains rigid, osseous resection or arthrodesis is mandated. Furthermore, the MTP joint must be assessed for instability using the Lachman (drawer) test. Tenderness directly over the dorsofibular capsule and fibular collateral ligament of the second MTP joint strongly indicates MTP synovitis and an impending crossover toe deformity, which must be differentiated from a simple interdigital neuroma.
Radiographic evaluation requires standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. The surgeon must scrutinize the AP radiograph to assess the metatarsal parabola (the relative lengths of the metatarsals). A disproportionately long second metatarsal is a frequent driver of second MTP joint instability and hammer toe formation, often necessitating a Weil distal metatarsal shortening osteotomy. The lateral radiograph is critical for evaluating the congruency of the MTP joint and identifying dorsal subluxation or frank dislocation of the proximal phalanx. The presence of degenerative joint disease at the PIP or MTP joints will also dictate the choice between resection arthroplasty and formal arthrodesis.
Patient positioning for lesser toe reconstruction is typically supine. A small bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the foot into a neutral, perfectly vertical alignment that facilitates dorsal surgical approaches. A pneumatic tourniquet is highly recommended to provide a bloodless surgical field, which is critical for identifying the delicate neurovascular bundles and the intricate layers of the extensor hood. The tourniquet may be placed at the thigh, calf, or ankle, depending on surgeon preference and the patient's vascular status. Anesthesia is typically achieved via a regional popliteal sciatic nerve block combined with a saphenous nerve block, or a highly localized ankle block, often supplemented with monitored anesthesia care (MAC) or general anesthesia.
Step-by-Step Surgical Approach and Fixation Technique
The surgical algorithm for hammer toe and claw toe deformities is strictly dictated by the flexibility of the deformity and the specific joints involved. The overarching goal is to restore a plantigrade, pain-free digit that fits comfortably within standard footwear. The procedures range from isolated soft-tissue rebalancing to complex osseous resections and joint realignments.
Soft-Tissue Procedures: Flexor-to-Extensor Transfer
Advocated historically by Girdlestone and Taylor, and later refined by Mann and Coughlin, the flexor-to-extensor tendon transfer (FDL transfer) is ideal for young patients (typically under 30 years of age) presenting with dynamic, flexible hammer toes and a normal medial longitudinal arch. This procedure operates on the elegant biomechanical principle of converting a primary deforming force (the FDL) into a corrective force. By transferring the FDL from the plantar aspect of the distal phalanx to the dorsal extensor hood, the transferred tendon acts to plantarflex the MTP joint and extend the PIP joint, thereby restoring the intrinsic balance of the digit.

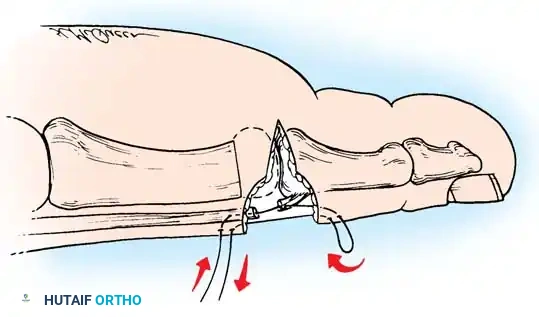
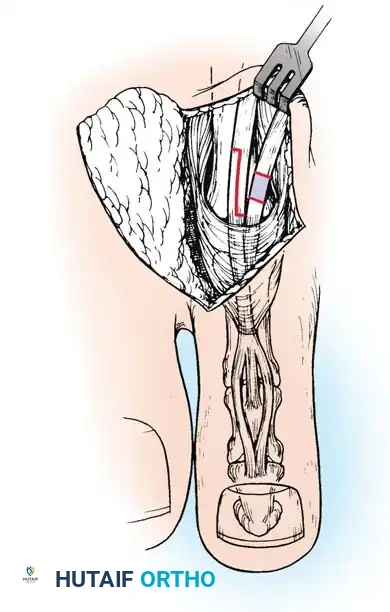
The technique begins with a longitudinal or transverse incision over the plantar aspect of the PIP joint, allowing identification and tenotomy of the FDL tendon just proximal to its insertion. The tendon is then split longitudinally into two slips. A dorsal incision is made over the proximal phalanx, and the two slips of the FDL are routed dorsally along the medial and lateral borders of the proximal phalanx. The slips are then interwoven into the dorsal extensor hood and sutured to themselves under physiological tension while the ankle is held in neutral and the toe is held in slight plantarflexion. A critical surgical pitfall must be noted: Myerson and Shereff have questioned the anatomical role of the FDL in causing PIP flexion contractures, emphasizing that this soft-tissue procedure must never be used in isolation if any rigid osseous contracture is present at the PIP joint.
Bone and Joint Procedures: PIP Resection Arthroplasty
For moderate, fixed deformities, resection of the head and neck of the proximal phalanx (the DuVries arthroplasty) remains the gold standard. While some authors advocate for formal PIP joint arthrodesis (fusion) using intramedullary implants, clinical studies by Lehman and Smith have demonstrated that up to 52% of patients are dissatisfied with a completely rigid, fused toe, as it fails to conform to the constraints of modern footwear. Resection arthroplasty allows for the development of a fibrous pseudoarthrosis, providing the toe with limited, comfortable mobility that molds harmoniously to adjacent digits.
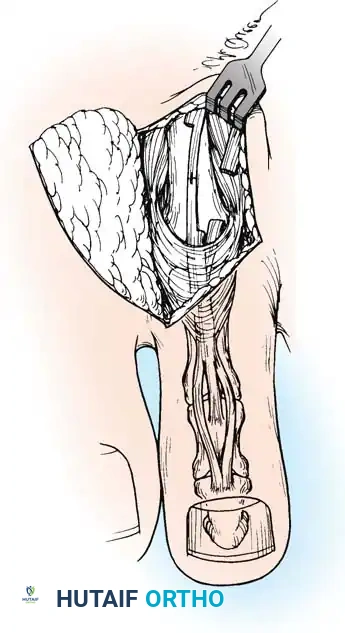
Step 1: Incision and Exposure
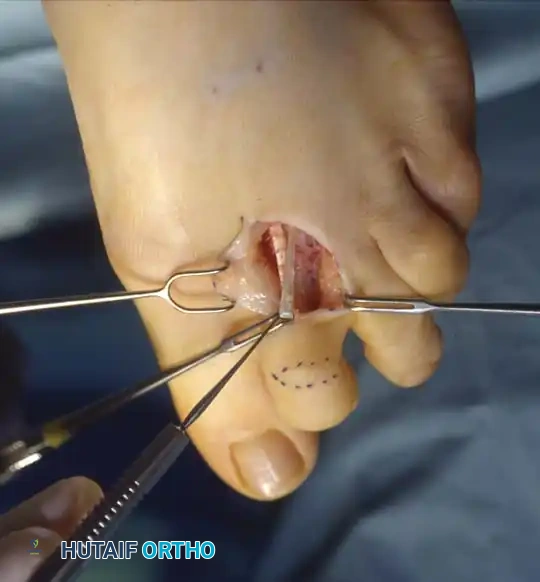
Make a precise elliptical incision over the dorsal aspect of the PIP joint. The ellipse should measure approximately 5 to 6 mm in width, with a 2- or 3-mm lateral extension on either side. This specific geometry facilitates a subsequent dermodesis (skin shortening), which acts as an adjunctive dynamic splint. Remove the elliptical skin island carefully, preserving the underlying superficial venous network where possible, and achieve meticulous hemostasis using bipolar electrocautery to prevent post-operative hematoma.

Step 2: Capsulotendinous Resection
Excise a slightly smaller segment of the underlying extensor tendon and dorsal capsule of the PIP joint. It is critical to leave a 2-mm remnant of the extensor tendon attached to the dorsal base of the middle phalanx to facilitate later repair. The proximal stump of the extensor tendon will naturally retract beneath the proximal skin flap but can be easily retrieved with fine forceps.
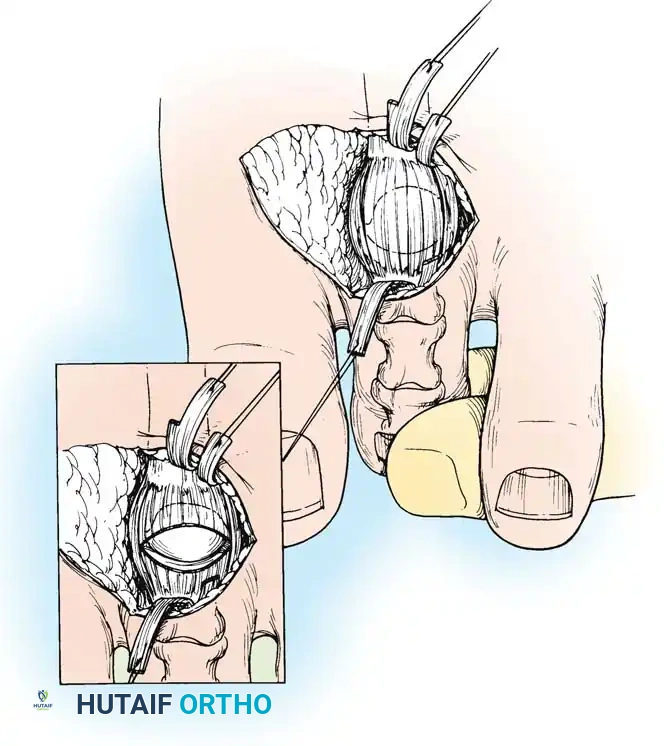
Step 3: Collateral Ligament Release
Apply firm longitudinal traction to the distal and middle phalanges while simultaneously flexing the PIP joint to approximately 20 degrees. Using a #15 blade, section the collateral ligaments from outside-in. The surgeon must carefully place the blade between the skin and the ligament, turning the cutting edge inward toward the joint space to avoid inadvertent injury to the neurovascular bundles running laterally. Once the collaterals are fully released, the PIP joint can be acutely flexed to 90 degrees, fully exposing the condyles of the proximal phalanx.

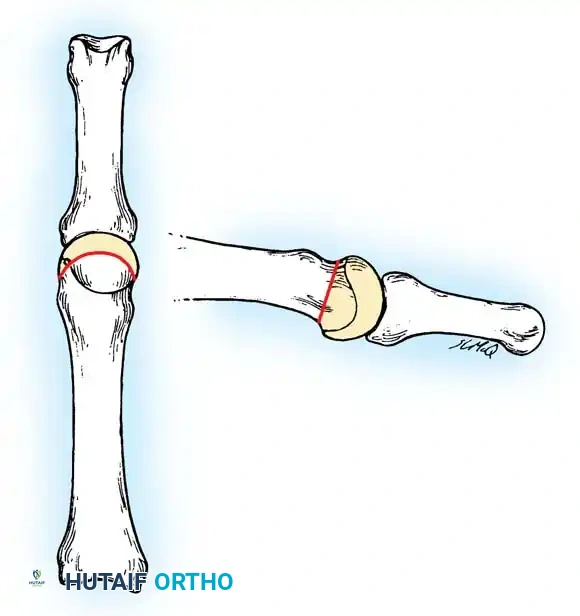
Step 4: Osseous Resection
Using a microsagittal saw or a sharp double-action bone cutter, resect the head and surgical neck of the proximal phalanx. Ensure the cut is perfectly perpendicular to the long axis of the phalangeal shaft to prevent asymmetric loading and recurrent angular deformity. Following the primary resection, use a fine rongeur or a bone rasp to smooth any sharp cortical edges that could irritate the overlying soft tissues or compromise the skin closure.



Step 5: Closure and Dermodesis
Approximate the extensor tendon ends using a 4-0 absorbable suture. Close the skin with a non-absorbable suture (e.g., 4-0 nylon) using a horizontal mattress technique. Because an ellipse of skin was removed during the approach, closing this defect creates a powerful dermodesis—a skin tightening effect that acts as a dynamic splint to hold the toe in extension during the healing phase.
Management of Severe Deformity and MTP Joint Subluxation
When the hammer toe or claw toe is accompanied by a fixed MTP extension contracture or frank dorsal subluxation, PIP resection alone will unequivocally fail. The MTP joint must be systematically decompressed through a sequential release. The surgeon begins with a Z-lengthening of the EDL tendon and a tenotomy of the EDB tendon. Next, a dorsal capsulotomy of the MTP joint is performed. If the joint remains subluxated, the surgeon must release the medial and lateral collateral ligaments off the metatarsal head. A McGlamry elevator is then swept proximally beneath the metatarsal head to release any dense plantar plate adhesions.
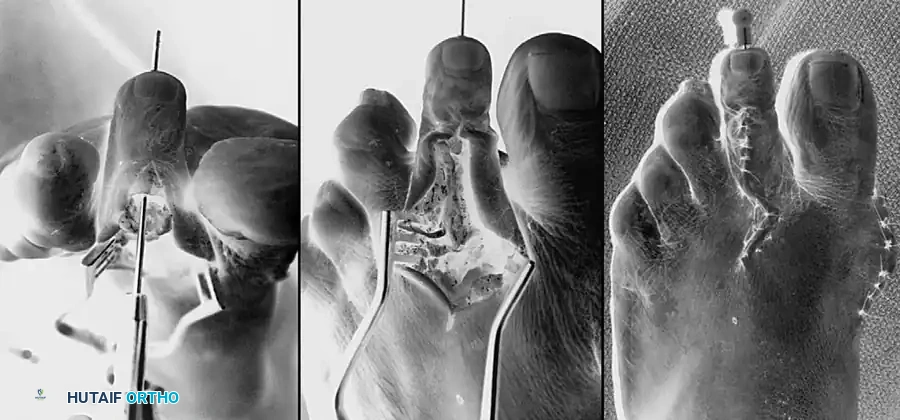
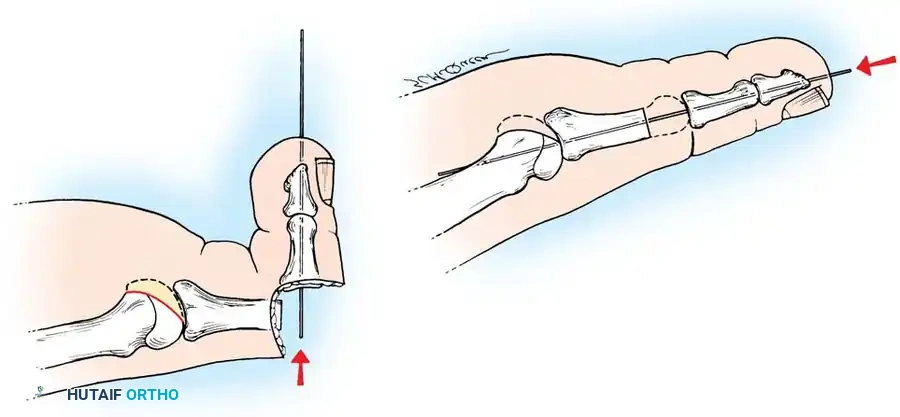
If the MTP joint remains irreducible despite comprehensive soft-tissue release, a Weil distal metatarsal osteotomy is indicated. This involves an intra-articular, extra-capsular osteotomy running parallel to the plantar aspect of the foot, allowing the metatarsal head to translate proximally, effectively decompressing the joint and relaxing the intrinsic musculature. Fixation is typically achieved with a single 0.045-inch or 0.062-inch Kirschner wire driven antegrade across the PIP joint and retrograde across the MTP joint, or via dedicated intra-medullary compression screws.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, reconstruction of lesser toe deformities is associated with a distinct set of potential complications. The orthopedic surgeon must be prepared to identify and manage these adverse events promptly to ensure optimal patient outcomes. The most common complication is recurrence of the deformity, which typically arises from inadequate initial osseous resection, failure to address concurrent MTP joint pathology, or premature removal of Kirschner wire fixation.
One of the most frustrating complications for both the patient and the surgeon is the "floating toe" syndrome. This occurs when the toe fails to purchase the ground during the stance phase of gait. It is typically the result of over-lengthening the metatarsal during a Weil osteotomy, excessive resection of the proximal phalanx, or iatrogenic disruption of the plantar plate and intrinsic musculature. Vascular compromise, though rare, is a catastrophic complication. A "white toe" indicates arterial insufficiency, often due to excessive tension on the neurovascular bundles following deformity correction, whereas a "blue toe" indicates venous congestion. Immediate management requires removal of all dressings, placing the foot in a dependent position, and potentially removing the K-wire or slightly flexing the toe to relieve tension.
| Complication | Estimated Incidence | Salvage Management and Corrective Strategy |
|---|---|---|
| Recurrent Deformity | 10% - 15% | Revision osseous resection, formal PIP arthrodesis, or FDL tendon transfer. |
| Floating Toe Syndrome | 5% - 12% | Plantar plate repair, flexor-to-extensor transfer, or revision metatarsal osteotomy. |
| Pin Tract Infection | 2% - 5% | Oral antibiotics, aggressive local pin care, early K-wire removal if deep infection suspected. |
| Vascular Compromise (Ischemia) | < 1% | Dependent positioning, warming, removal of K-wire, immediate vascular surgery consultation. |
| Non-union (in Arthrodesis) | 5% - 10% | Often asymptomatic; if painful, revision arthrodesis with robust bone grafting and rigid internal fixation. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol is critical for maintaining the surgical correction and optimizing functional recovery. The rehabilitation process is generally divided into three distinct phases, tailored to the specific procedures performed and the patient's overall compliance.
Phase 1: Immediate Post-Operative Period (Weeks 0-2)
Immediately following surgery, the foot is placed in a bulky, compressive dressing to minimize edema and protect the surgical incisions. If Kirschner wires were utilized, the tips are typically capped or bent to prevent migration and snagging on clothing. The patient is instructed to remain strictly heel-weight bearing or flat-foot weight bearing in a rigid, postoperative surgical shoe. Elevation of the operative extremity above the level of the heart is mandatory for the first 48 to 72 hours to mitigate swelling and reduce throbbing pain. The first post-operative visit occurs at 10 to 14 days, during which the bulky dressing is removed, the incisions are inspected, and sutures are removed if the wounds are adequately healed.
Phase 2: Pin Management and Transition (Weeks 3-6)
During this phase, the patient continues to weight-bear in the rigid postoperative shoe. Daily pin care is instituted, typically involving cleansing the pin sites with a dilute povid
Clinical & Radiographic Imaging Archive