Tibial Plateau Fractures: Epidemiology, Anatomy, Biomechanics & Surgical Management
Key Takeaway
Tibial plateau fractures are complex intra-articular injuries of the proximal tibia. They are classified by systems like Schatzker and AO/OTA based on morphology. This classification is crucial for surgical planning, aiming to restore articular congruity, mechanical axis alignment, and knee stability, which minimizes post-traumatic osteoarthritis and optimizes functional outcomes.
Introduction and Epidemiology
Tibial plateau fractures are complex intra-articular injuries involving the proximal tibia, characterized by damage to the articular cartilage, subchondral bone, and metaphyseal bone of the knee joint. These fractures represent approximately 1% of all fractures and 8% of fractures in elderly patients, exhibiting a distinct bimodal age distribution. In younger individuals, they typically result from high-energy trauma, such as motor vehicle collisions or falls from significant heights, presenting with severe axial loading combined with varus or valgus stress. These high-energy mechanisms are frequently associated with significant soft tissue injury, including meniscal tears, ligamentous ruptures, and potential neurovascular compromise. In the elderly population, low-energy falls associated with osteopenia or osteoporosis are the predominant etiology, often resulting in depression-type fracture patterns due to decreased subchondral bone density.
The primary goal of surgical management is the anatomic restoration of articular congruity, correction of the mechanical axis, and re-establishment of knee stability. Achieving these objectives facilitates early range of motion, which is critical for cartilage nutrition and minimizing post-traumatic osteoarthritis, ultimately optimizing functional outcomes. Failure to achieve stable anatomic reduction can lead to chronic pain, arthrofibrosis, coronal or sagittal plane instability, and premature joint degeneration necessitating complex arthroplasty.
The Schatzker classification system remains the most widely utilized clinical tool, categorizing tibial plateau fractures based on fracture morphology and condylar involvement:
* Schatzker Type I Lateral tibial plateau fracture pure wedge split
* Schatzker Type II Lateral tibial plateau fracture wedge with depression
* Schatzker Type III Lateral tibial plateau pure depression fracture
* Schatzker Type IV Medial tibial plateau fracture
* Schatzker Type V Bicondylar tibial plateau fracture
* Schatzker Type VI Tibial plateau fracture with metaphyseal diaphyseal dissociation
While the Schatzker system is foundational, the AO OTA classification 41B partial articular and 41C complete articular provides more granular detail regarding fracture morphology. Furthermore, the modern understanding of complex plateau fractures has evolved to include the Three Column Concept introduced by Luo et al. This system divides the tibial plateau into medial, lateral, and posterior columns based on axial computed tomography imaging, fundamentally altering the surgical approach to posterior shearing fractures that are poorly visualized and inadequately addressed through traditional anterior or lateral approaches.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional osteology, ligamentous anatomy, and biomechanics is paramount for successful surgical management and preoperative templating of tibial plateau fractures.
Proximal Tibial Osteology
The superior aspect of the tibia consists of the medial and lateral condyles, separated by the intercondylar eminence. The medial condyle is typically larger, concave, and possesses stronger, denser subchondral bone. It is oval-shaped and acts as the primary weight-bearing surface. Conversely, the lateral condyle is smaller, convex, and more circular, with relatively weaker cancellous bone, making it highly susceptible to depression fractures upon axial loading. The proximal tibia possesses a natural posterior slope averaging 7 to 10 degrees, which must be meticulously recreated during surgical fixation to restore normal knee kinematics and prevent anterior cruciate ligament overload.
Meniscal and Ligamentous Anatomy
The medial and lateral menisci are semi-lunar fibrocartilaginous structures that enhance joint congruity, distribute hoop stresses, and increase the contact area of the tibiofemoral joint. They are frequently injured in tibial plateau fractures, with lateral meniscal tears highly prevalent in Schatzker II fractures. Entrapment of the meniscus within the fracture site is a common impediment to anatomic reduction.
The ligamentous stabilizers include the medial collateral ligament resisting valgus stress and the lateral collateral ligament resisting varus stress. The anterior and posterior cruciate ligaments dictate sagittal and rotational stability. High-energy plateau fractures, particularly Schatzker IV and fracture-dislocations, carry a high incidence of concurrent cruciate or collateral ligament avulsions or mid-substance ruptures.
Neurovascular Structures
The popliteal artery and vein are located directly posterior to the knee joint capsule. They are tethered at the adductor hiatus proximally and the soleus arch distally, rendering them highly vulnerable to traction injuries in severe hyperextension mechanisms or posterior shearing fractures. The common peroneal nerve courses superficially around the fibular neck. It is highly susceptible to iatrogenic injury during lateral surgical approaches, placement of proximal lateral locking screws, or direct trauma from the initial injury.
Knee Joint Biomechanics
The normal mechanical axis of the lower extremity passes precisely through the center of the knee joint. During the normal gait cycle, the medial plateau bears approximately 60 percent of the axial load in full extension. Joint reaction forces can reach up to three times body weight during normal ambulation and significantly higher during dynamic activities. The menisci are critical load distributors; loss of meniscal integrity exponentially increases peak contact stresses on the articular cartilage, accelerating chondrocyte apoptosis and subsequent osteoarthritis. An uncorrected varus or valgus deformity secondary to a malreduced tibial plateau fracture shifts the mechanical axis, creating asymmetric loading and leading to rapid, predictable joint failure.
Indications and Contraindications
The decision to proceed with operative versus non-operative management hinges on fracture morphology, degree of displacement, associated soft tissue envelope viability, and patient-specific factors including baseline functional status and medical comorbidities.
Operative Versus Non Operative Guidelines
| Parameter | Non Operative Management | Operative Management |
|---|---|---|
| Articular Step Off | Less than 2 to 3 mm | Greater than 3 mm |
| Condylar Widening | Less than 5 mm | Greater than 5 mm |
| Mechanical Axis | Intact coronal and sagittal alignment | Varus or valgus deformity greater than 5 degrees |
| Joint Stability | Stable to varus and valgus stress at 0 and 30 degrees | Instability greater than 10 degrees compared to contralateral knee |
| Fracture Pattern | Non-displaced Schatzker I or III | Schatzker IV, V, VI, and highly displaced I to III |
| Soft Tissue Status | Intact, no compartment syndrome | Open fractures, acute compartment syndrome |
| Patient Factors | Non-ambulatory, severe medical comorbidities precluding anesthesia | Ambulatory patients, healthy enough for surgical intervention |
Contraindications to Immediate Internal Fixation
Absolute contraindications to immediate open reduction and internal fixation include active local infection and critical soft tissue compromise. High-energy injuries frequently present with severe soft tissue swelling, fracture blisters, and compromised microcirculation. Incising through compromised soft tissue carries an unacceptably high risk of wound dehiscence and deep infection. In such scenarios, damage control orthopedics utilizing a spanning external fixator is the standard of care. Surgery is delayed until the soft tissue envelope recovers, clinically indicated by the resolution of edema and the return of skin wrinkles, commonly referred to as the wrinkle sign, which typically occurs 10 to 21 days post-injury.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful outcomes in complex intra-articular trauma.
Imaging and Templating
Standard orthogonal radiographs including anteroposterior, lateral, and oblique views of the knee are mandatory. A traction radiograph can occasionally assist in determining the ligamentotaxis potential of the fracture fragments.
Computed tomography without contrast is the gold standard and absolute requirement for operative planning. Axial, coronal, and sagittal reformats, along with three-dimensional reconstructions, allow the surgeon to map the fracture lines, identify the location of articular depression, and determine the involvement of the posterior column. The CT scan dictates the surgical approach; for instance, a posteromedial fracture line requires a posteromedial approach, as it cannot be reduced or stabilized via an anterolateral incision. Magnetic resonance imaging is rarely indicated in the acute setting unless there is high suspicion of an isolated ligamentous injury that would fundamentally alter the surgical approach, though it is highly sensitive for detecting concurrent meniscal and cruciate pathology.
The Span Scan and Plan Protocol
For high-energy bicondylar fractures or those with severe soft tissue injury, the standard treatment algorithm is Span, Scan, and Plan.
1. Span: Immediate application of a knee-spanning external fixator to restore length, alignment, and rotation, while providing skeletal stability to allow soft tissue resuscitation.
2. Scan: Obtaining a high-resolution CT scan after the limb is out to length in the external fixator.
3. Plan: Utilizing the CT data to select appropriate surgical approaches, implant types, and bone graft requirements once the soft tissues permit definitive fixation.
Patient Positioning and Operating Room Setup
The patient is typically positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, ensuring the patella points directly toward the ceiling. A radiolucent triangle or ramp is placed under the knee to allow for varying degrees of flexion, which relaxes the gastrocnemius muscle and facilitates posterior fracture reduction.
A sterile tourniquet is applied to the proximal thigh but should be used judiciously to minimize ischemic complications and post-operative neuropraxia. The fluoroscopy unit must enter from the contralateral side of the table, allowing for unobstructed anteroposterior and lateral imaging throughout the procedure. For isolated posterior shear fractures requiring a direct posterior approach, the patient may be positioned prone, requiring meticulous padding of all bony prominences.
Detailed Surgical Approach and Technique
The surgical approach must be tailored to the specific fracture morphology dictated by preoperative CT imaging. The overarching principles include anatomic reduction of the articular surface, elevation of depressed fragments, filling of metaphyseal voids with bone graft or substitutes, and stable internal fixation utilizing buttress plating principles.
Anterolateral Surgical Approach
The anterolateral approach is the workhorse for Schatzker types I, II, and III fractures, providing excellent exposure of the lateral tibial plateau.
1. Incision: A longitudinal or slightly curved incision is made centered over Gerdy's tubercle, extending proximally toward the lateral epicondyle and distally along the anterior tibial crest.
2. Superficial Dissection: The iliotibial band is incised in line with its fibers. The anterior compartment fascia is released off Gerdy's tubercle, and the tibialis anterior muscle is elevated off the proximal lateral tibia.
3. Arthrotomy: A submeniscal arthrotomy is performed. The coronary ligament is incised, and the lateral meniscus is tagged with non-absorbable sutures and elevated superiorly. This provides direct visualization of the lateral articular surface.
4. Reduction: For split-depression fractures, the lateral split fragment is opened like a book. A cortical window may be created distally if necessary. A bone tamp is introduced beneath the depressed articular segment, and the cartilage is elevated anatomically under direct vision and fluoroscopic guidance.
5. Grafting: The resulting metaphyseal void is structurally supported using autograft, allograft, or synthetic bone substitutes (e.g., calcium phosphate cement) to prevent post-operative subsidence.
6. Fixation: The lateral split is reduced and provisionally held with Kirschner wires. A pre-contoured lateral proximal tibial locking plate is applied. Subchondral rafting screws are placed parallel to the joint line to support the elevated articular cartilage. Distal fixation is achieved with bicortical screws in the diaphysis.
Posteromedial Surgical Approach
The posteromedial approach is essential for Schatzker type IV fractures and the medial component of Schatzker type V and VI fractures.
1. Positioning and Incision: With the leg externally rotated and slightly flexed, a longitudinal incision is made along the posteromedial border of the proximal tibia.
2. Internervous Plane: The dissection proceeds between the medial head of the gastrocnemius (innervated by the tibial nerve) posteriorly and the pes anserinus tendons (innervated by the femoral nerve) anteriorly.
3. Deep Dissection: The saphenous nerve and great saphenous vein are identified and protected anteriorly. The medial gastrocnemius is retracted laterally, protecting the popliteal neurovascular bundle. The popliteus muscle may be partially elevated off the posterior tibia to expose the fracture.
4. Fixation: Medial plateau fractures typically involve a shear mechanism and require anti-glide buttress plating. A plate is placed on the posteromedial apex of the fracture and under-contoured slightly to provide a buttress effect against the apical displacement of the medial condyle.
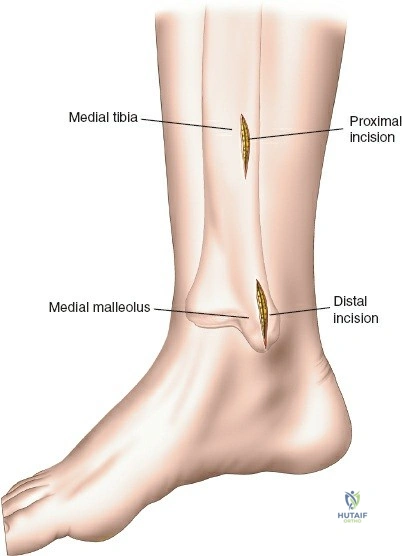
Dual Incision Technique for Bicondylar Fractures
For Schatzker V and VI fractures requiring both medial and lateral fixation, a dual incision technique is utilized. A critical principle is maintaining an adequate skin bridge between the anterolateral and posteromedial incisions to prevent skin necrosis. The skin bridge must be a minimum of 7 centimeters wide. The medial side is typically addressed first to restore the medial column, which serves as the foundation for the lateral articular reduction.
Management of Intra Articular Soft Tissues
Thorough inspection of the joint is mandatory. Entrapped menisci must be extricated from fracture lines. Peripheral meniscal tears should be repaired using standard inside-out or all-inside techniques to restore hoop stresses. Meniscectomy should be strictly avoided if possible, as it significantly accelerates post-traumatic arthritis in the setting of a compromised articular surface. Cruciate ligament avulsions with large bony fragments can be repaired acutely with suture anchors or lag screws; however, mid-substance tears are typically addressed in a delayed fashion after fracture union and rehabilitation, if symptomatic instability persists.
Complications and Management
Surgical management of tibial plateau fractures carries a significant risk profile, particularly in high-energy injuries. Anticipation, early recognition, and aggressive management of complications are critical.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Compartment Syndrome | 5 to 10 percent | High-energy crush injuries, severe edema, bleeding into fascial compartments. | Emergent four-compartment fasciotomy. Delayed primary closure or split-thickness skin grafting once swelling subsides. |
| Deep Surgical Site Infection | 5 to 20 percent | Open fractures, early surgery through compromised soft tissue, smoking, diabetes. | Aggressive surgical debridement, hardware retention if stable, targeted intravenous antibiotics. If hardware is loose or union is achieved, hardware removal and antibiotic spacer placement. |
| Post Traumatic Osteoarthritis | 20 to 40 percent | Initial articular cartilage damage, residual articular step-off, meniscectomy, mechanical axis malalignment. | Conservative management initially (NSAIDs, injections, bracing). Definitive salvage is Total Knee Arthroplasty (TKA). TKA in this setting is complex, often requiring stems and augments. |
| Peroneal Nerve Palsy | 1 to 3 percent | Initial varus thrust injury, iatrogenic traction during lateral approach, lateral plate impingement. | Observation for neuropraxia. Ankle-foot orthosis (AFO) for foot drop. If no recovery by 6 to 12 months, consider tendon transfer (e.g., posterior tibial tendon transfer) or nerve exploration. |
| Nonunion or Malunion | 2 to 5 percent | Inadequate fixation, infection, smoking, premature weight-bearing leading to varus collapse. | Revision ORIF with autogenous bone grafting for nonunion. Corrective osteotomy for malunion. Arthroplasty for severe intra-articular malunion in older patients. |
| Hardware Prominence | 10 to 15 percent | Lack of soft tissue coverage over the anterolateral or medial proximal tibia. | Hardware removal after radiographic and clinical confirmation of solid fracture union (typically 12 to 18 months post-operatively). |
Post Operative Rehabilitation Protocols
Rehabilitation following surgical fixation of tibial plateau fractures requires a delicate balance between protecting the articular reduction and initiating early motion to prevent arthrofibrosis and promote cartilage healing. Protocols must be individualized based on fracture severity, fixation stability, and patient compliance.
Phase One Early Protection and Motion
Spanning from post-operative day one to six weeks. The primary goal is wound healing, edema control, and restoration of passive range of motion.
* Weight Bearing: Strict non-weight bearing (NWB) or touch-down weight bearing (TDWB) with bilateral crutches or a walker.
* Bracing: A hinged knee brace locked in extension for ambulation and sleep to protect soft tissues and prevent flexion contractures.
* Range of Motion: Continuous passive motion (CPM) machines may be utilized. Active-assisted and passive range of motion exercises are initiated immediately, aiming for 0 to 90 degrees of flexion by week four.
* Strengthening: Isometric quadriceps sets, straight leg raises in the brace, and ankle pumps to prevent deep vein thrombosis.
Phase Two Progressive Loading
Spanning from six to twelve weeks post-operatively. Progression is contingent upon radiographic evidence of early callus formation and maintenance of articular reduction.
* Weight Bearing: Gradual progression of weight-bearing, typically advancing 25 percent of body weight per week, aiming for full weight-bearing by 10 to 12 weeks.
* Range of Motion: The hinged knee brace is unlocked for ambulation. The goal is to achieve full, symmetric range of motion (0 to 130+ degrees).
* Strengthening: Initiation of closed kinetic chain exercises (e.g., mini-squats, leg press) as weight-bearing status allows. Stationary cycling is excellent for both motion and early strengthening.
Phase Three Advanced Strengthening and Return to Function
Spanning from three to six months and beyond.
* Weight Bearing: Full, unrestricted weight-bearing.
* Strengthening: Advanced progressive resistance training focusing on quadriceps, hamstrings, and gluteal musculature. Proprioceptive and balance training.
* Return to Activity: Return to high-impact activities or heavy manual labor is typically restricted until 6 to 9 months post-operatively, requiring symmetric strength and absence of pain or effusion.
Summary of Key Literature and Guidelines
The surgical management of tibial plateau fractures has been heavily influenced by several landmark academic publications and clinical trials.
The foundational framework for classification and initial treatment algorithms was established by Schatzker et al. in their seminal 1979 paper. This classification highlighted the distinct differences in fracture morphology and energy mechanisms between medial and lateral plateau injuries, establishing the necessity of operative intervention for displaced intra-articular fractures.
The evolution of soft tissue management was profoundly shaped by Egol et al., who popularized the staged treatment protocol for high-energy proximal tibia fractures. Their research demonstrated that utilizing a temporary spanning external fixator followed by delayed definitive open reduction and internal fixation significantly reduced the incidence of catastrophic wound complications and deep infections compared to early, aggressive single-stage surgery.
Regarding bicondylar tibial plateau fractures (Schatzker V and VI), the Canadian Orthopaedic Trauma Society (COTS) conducted a landmark multicenter randomized controlled trial comparing dual plating with fine-wire circular external fixation (Ilizarov methodology). Published in the Journal of Bone and Joint Surgery, the study found similar functional outcomes between the two groups at two years. However, the dual plating group exhibited a higher rate of early soft tissue complications and reoperations, while the circular fixator group experienced higher rates of superficial pin tract infections. This study solidified the role of both techniques, emphasizing that treatment must be tailored to the surgeon's expertise and the patient's soft tissue envelope.
More recently, the anatomical understanding of fracture patterns has been revolutionized by Luo et al., who introduced the Three-Column Classification based on axial CT imaging. Published in the Journal of Orthopaedic Trauma, this concept demonstrated that a significant percentage of complex fractures involve a posterior coronal shear component. This paradigm shift has mandated the increased utilization of posteromedial and direct posterior surgical approaches, as traditional anterolateral plating is biomechanically insufficient to stabilize posterior column depression and shear.
Current academic guidelines strongly emphasize anatomic articular reduction, restoration of the mechanical axis, rigid fixation allowing early motion, and meticulous respect for the soft tissue envelope as the non-negotiable tenets of tibial plateau fracture management.
