Comprehensive Conservative Management and Radiographic Evaluation of Patellofemoral Instability
Key Takeaway
Conservative management of acute patellar dislocation focuses on immediate joint reduction, hemarthrosis aspiration, and structured rehabilitation. Initial treatment involves short-term immobilization and cryotherapy, rapidly progressing to closed-chain quadriceps strengthening. Advanced imaging, including axial radiographs and CT scans for TT-TG distance, dictates the necessity of surgical intervention in cases of recurrent subluxation or persistent patellofemoral malalignment.
Comprehensive Introduction and Patho-Epidemiology
Patellofemoral instability represents one of the most challenging and multifactorial clinical entities encountered in orthopedic surgery. The pathology encompasses a broad continuum ranging from subtle, chronic recurrent subluxation to acute, high-energy traumatic lateral dislocation of the patella. Historically, the management of this condition was plagued by an oversimplification of the underlying biomechanics, often resulting in high failure rates following isolated soft-tissue procedures such as lateral retinacular releases. Modern orthopedic understanding, however, dictates a highly individualized, "à la carte" approach that respects the complex interplay of osseous geometry, ligamentous integrity, and dynamic neuromuscular control. The patellofemoral articulation is inherently discordant; it relies on a delicate balance of static and dynamic restraints that must function synchronously across the entire arc of knee motion.
Epidemiologically, acute patellar dislocations account for approximately 2% to 3% of all knee injuries presenting to emergency departments, with an incidence rate estimated at 5.8 per 100,000 in the general population. However, this incidence skyrockets to 29 per 100,000 in the high-risk demographic of active adolescents aged 10 to 17 years. Females have historically been considered at higher risk due to inherent ligamentous laxity and greater pelvic width increasing the quadriceps angle (Q-angle); however, recent epidemiological data suggest that in the adolescent athletic population, the incidence is nearly equal between sexes. The natural history of a first-time patellar dislocation is notoriously unpredictable, with recurrent instability rates reported between 15% and 44% following conservative management, and escalating to over 50% if the patient is younger than 15 years at the time of the initial injury.
The patho-epidemiology is further complicated by the presence of predisposing anatomic risk factors, often referred to as the "menu à la carte" of patellofemoral dysplasia. These include trochlear dysplasia, patella alta, an excessive Tibial Tubercle-Trochlear Groove (TT-TG) distance, and generalized ligamentous hyperlaxity. The presence of these anatomic variants shifts the etiology from a purely traumatic event to an atraumatic, biomechanically inevitable failure. When these stabilizing mechanisms fail, the patella translates laterally, often resulting in an acute rupture of the medial patellofemoral ligament (MPFL) and impaction of the medial patellar facet against the lateral femoral condyle. This impaction mechanism is responsible for the high incidence of osteochondral fractures, which occur in up to 40% of acute dislocations and significantly alter the treatment algorithm from conservative rehabilitation to acute surgical intervention.
While surgical intervention is increasingly discussed and refined in modern orthopedic literature, a meticulously structured conservative treatment protocol remains the absolute cornerstone of management for first-time acute dislocations devoid of intra-articular loose bodies. Furthermore, non-operative management is the primary modality for many cases of chronic patellofemoral malalignment without gross structural dysplasia. Understanding the epidemiological variables and the precise pathoanatomy of the injury is paramount for the orthopedic surgeon to accurately counsel patients, predict the likelihood of recurrence, and formulate a comprehensive, evidence-based treatment strategy that mitigates the long-term risk of patellofemoral osteoarthritis.
Detailed Surgical Anatomy and Biomechanics
The stability of the patellofemoral joint is dictated by an elegant but unforgiving synergy between static ligamentous restraints, osseous topography, and dynamic muscular forces. The primary static soft-tissue stabilizer is the medial patellofemoral ligament (MPFL). Anatomically, the MPFL is a distinct condensation of capsular fibers within layer two of the medial knee, originating from a highly specific saddle-shaped depression located between the medial epicondyle and the adductor tubercle of the femur. This femoral origin, radiographically identified as Schöttle's point, is critical for achieving isometry during surgical reconstruction. The ligament courses anteriorly to insert on the superomedial border of the patella. Biomechanical studies have unequivocally demonstrated that the MPFL provides 50% to 60% of the total restraint against lateral patellar translation at 0 to 30 degrees of knee flexion, precisely when the patella is least constrained by the bony trochlea.
Secondary static restraints include the medial patellomeniscal ligament (MPML) and the medial patellotibial ligament (MPTL), which collectively contribute an additional 20% to 30% of the restraint against lateral translation, particularly at higher flexion angles. The lateral retinaculum, comprising the superficial oblique and deep transverse layers, provides a counter-tension that must be balanced against the medial structures. Over-tightness of the lateral retinaculum can induce a lateral patellar tilt, exacerbating articular overload and functional instability. The osseous geometry of the femoral trochlea serves as the ultimate static stabilizer once the knee flexes past 30 degrees. In a normal knee, the patella engages the trochlear groove, and the lateral trochlear facet acts as a bony buttress against lateral subluxation. Trochlear dysplasia, characterized by a flattened or convex sulcus, obliterates this bony constraint, leaving the patella entirely reliant on the soft-tissue restraints, which inevitably stretch and fail under repetitive load.
The dynamic stabilizers are governed by the extensor mechanism, specifically the balanced vector forces of the vastus medialis obliquus (VMO) and the vastus lateralis (VL). The VMO is unique among the quadriceps musculature; its fibers are oriented at a 50- to 55-degree angle relative to the femoral shaft, inserting directly onto the medial border of the patella. Unlike the vastus intermedius or rectus femoris, the VMO does not primarily extend the knee; rather, it functions as a dynamic medializer, actively pulling the patella into the trochlear groove during early flexion. Following an acute dislocation and the resultant hemarthrosis, the VMO is exquisitely susceptible to reflex arthrogenic muscle inhibition, leading to rapid atrophy and a catastrophic loss of dynamic medial tracking.
Biomechanically, patellofemoral kinematics involve a complex pattern of gliding, tilting, and rotation. As the knee flexes from terminal extension, the patella normally tracks from a slightly lateralized position, engages the trochlea at approximately 20 to 30 degrees, and translates medially before moving slightly lateral again in deep flexion. The joint reaction forces across the patellofemoral articulation are immense, reaching up to 3 times body weight during stair climbing and up to 7 to 8 times body weight during deep squatting. Any alteration in the coronal alignment (such as an increased Q-angle or a TT-TG distance exceeding 20 mm) creates a massive laterally directed vector force. When the knee extends, this lateral vector overcomes the weakened medial restraints, resulting in the classic "J-sign" indicative of severe patellar maltracking and impending subluxation.
Exhaustive Indications and Contraindications
The decision-making process in patellofemoral instability requires a nuanced understanding of when to employ conservative management and when surgical intervention is absolutely mandated to preserve the articular cartilage. The treatment algorithm must be tailored to the patient's chronicity, anatomic risk factors, and activity demands.
Conservative management is the definitive gold standard for first-time acute patellar dislocations in patients with normal or near-normal underlying anatomy. The primary indication for non-operative treatment is a primary dislocation event with a spontaneously reduced patella, an intact extensor mechanism, and, most critically, the absolute absence of osteochondral fractures or intra-articular loose bodies on radiographic imaging. Additionally, patients presenting with chronic, atraumatic patellofemoral pain syndrome or subtle recurrent subluxation who have not yet undergone a rigorous, structured physical therapy program are prime candidates for conservative care. The presence of mild trochlear dysplasia or slightly elevated TT-TG distances (15-19 mm) does not preclude a trial of conservative management, provided the patient is compliant and understands the risk of recurrence.
Conversely, the indications for surgical intervention are clear and must not be delayed when conservative measures have failed or when specific pathoanatomic thresholds are breached. Acute surgical intervention is strictly indicated in the presence of a displaced osteochondral fracture (often originating from the medial patellar facet or the lateral femoral condyle) that requires fixation or removal to prevent rapid joint destruction. Chronic surgical indications include recurrent instability episodes despite a minimum of 3 to 6 months of dedicated, VMO-focused physical therapy. Furthermore, gross anatomic abnormalities dictate surgical correction; a TT-TG distance exceeding 20 mm is a universally accepted indication for a tibial tubercle osteotomy (TTO) to normalize the extensor vector. Severe patella alta (Caton-Deschamps index > 1.2) or high-grade trochlear dysplasia (Dejour Types B, C, D) in the setting of recurrent instability also constitute strong indications for complex bony realignment procedures, often combined with MPFL reconstruction.
Contraindications to surgical intervention are equally important to recognize to prevent disastrous postoperative outcomes. MPFL reconstruction is contraindicated as an isolated procedure in patients with a TT-TG distance > 20 mm or severe patella alta, as the uncorrected bony malalignment will inevitably stretch and rupture the graft. Tibial tubercle osteotomies are strictly contraindicated in skeletally immature patients with open proximal tibial physes due to the high risk of inducing a recurvatum deformity or premature physeal arrest. Furthermore, aggressive realignment procedures are relatively contraindicated in patients with advanced, bone-on-bone patellofemoral osteoarthritis, where a patellofemoral arthroplasty or total knee arthroplasty may be the only viable salvage options.
| Modality / Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Conservative Management | First-time acute dislocation; No loose bodies; Mild subluxation; Normal TT-TG (<15mm). | Displaced osteochondral fracture; Massive intra-articular loose body; Extensor mechanism rupture. | High-demand elite athlete with recurrent instability; Severe Dejour D dysplasia. |
| Isolated MPFL Reconstruction | Recurrent instability; Failed conservative tx; Normal osseous alignment (TT-TG <15mm, normal height). | TT-TG > 20mm; Severe patella alta (Caton-Deschamps > 1.2); Advanced patellofemoral OA. | Open physes (requires specific physeal-sparing techniques); Stiff knee. |
| Tibial Tubercle Osteotomy (TTO) | TT-TG > 20mm; Patella alta; Distal/lateral chondral lesions requiring offloading (Anteromedialization). | Open proximal tibial physis; Active joint infection; Complex regional pain syndrome (CRPS). | Heavy smokers (non-union risk); Poor soft tissue envelope over the anterior tibia. |
| Trochleoplasty | Severe trochlear dysplasia (Dejour B, D) with supratrochlear spur; Recurrent instability despite TTO/MPFL. | Open physes; Thin trochlear cartilage (<3mm); Advanced patellofemoral osteoarthritis. | Inexperienced surgeon; Mild dysplasia (Dejour A). |
Pre-Operative Planning, Templating, and Patient Positioning
A comprehensive pre-operative evaluation, heavily reliant on meticulous radiographic analysis, is mandatory to assess the underlying osseous architecture, identify predisposing dysplastic factors, and formulate a precise surgical or conservative plan. Standard anteroposterior (AP) and true lateral radiographs are routine, but specialized views and advanced cross-sectional imaging are required to truly appreciate patellofemoral tracking, congruence, and rotational profiles.
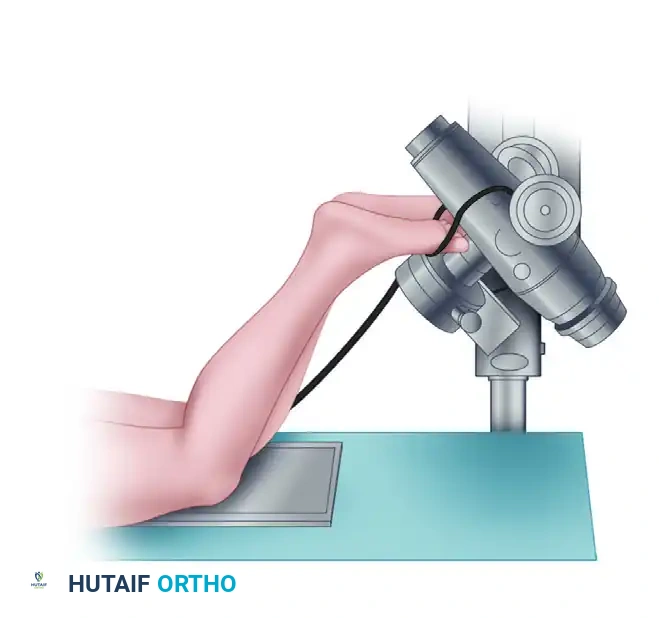
Proper patient positioning is paramount for obtaining reproducible and diagnostically accurate radiographs. The infrapatellar view is utilized to assess the inferior pole of the patella and the patellar tendon footprint.

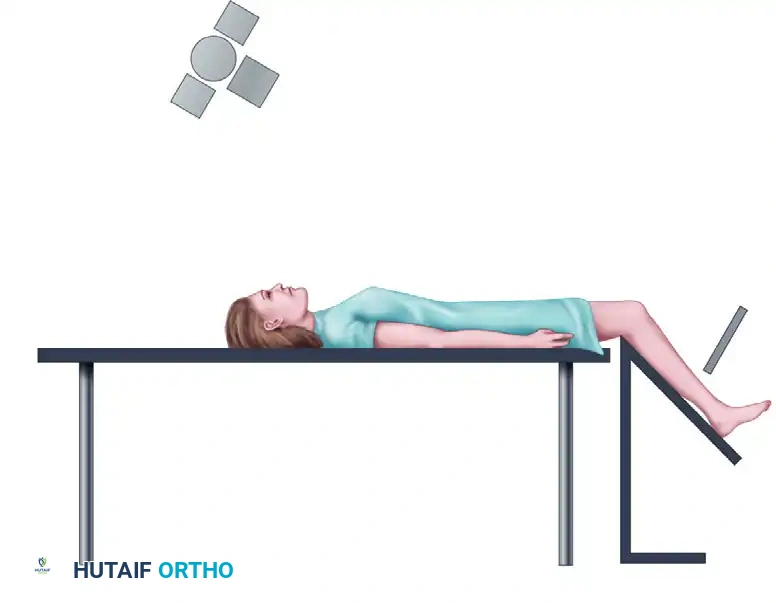
The axial view is critical for assessing the dynamic tracking of the patella within the trochlear groove, typically obtained with the knee flexed to 30 or 45 degrees.
The skyline view provides a tangential perspective of the patellofemoral articulation, allowing the surgeon to evaluate the medial and lateral facets, the depth of the trochlear sulcus, and the presence of marginal osteophytes.
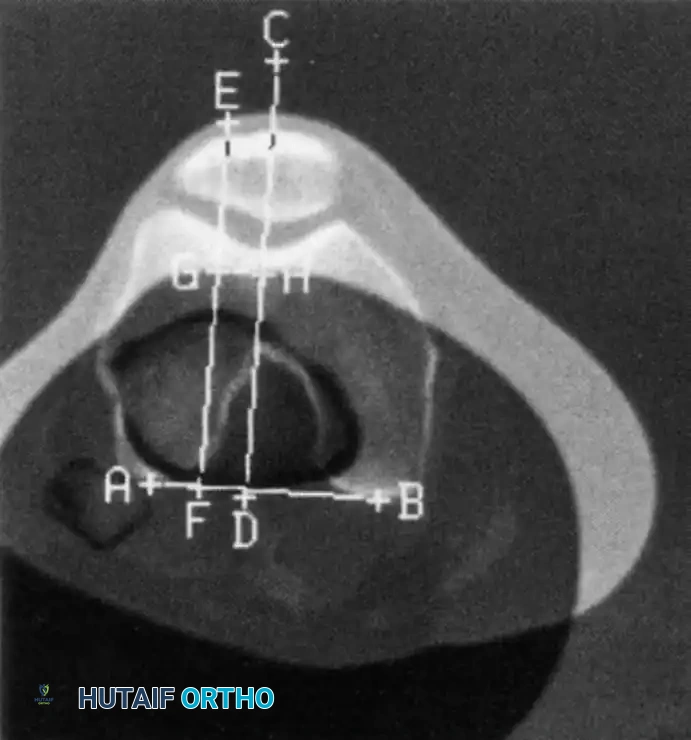
Once the appropriate views are obtained, the surgeon must analyze the images for signs of malalignment, tilt, and dysplasia. On an axial or skyline view, the patella should sit symmetrically within the trochlea. A lateral tilt indicates tightness of the lateral retinaculum and potential insufficiency of the medial restraints.

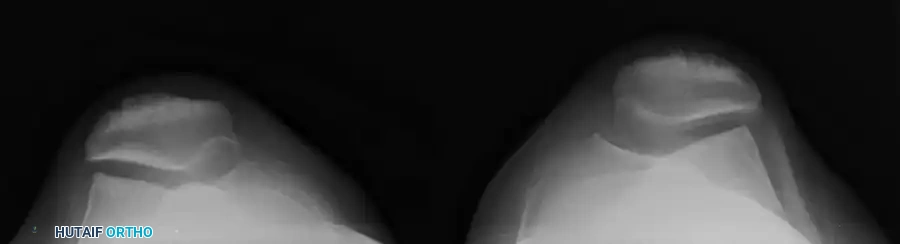
The morphology of the femoral sulcus is a primary determinant of patellar stability. The Merchant view is particularly useful for demonstrating a wide, flattened sulcus angle, which predisposes the patient to lateral subluxation.

An analysis of patellofemoral congruence is highly indicated. The measurements described by Merchant et al. remain the gold standard for quantifying patellar subluxation. A congruence angle greater than +16 degrees is highly indicative of pathologic lateral patellar subluxation.
While plain radiographs provide excellent baseline data, Computed Tomography (CT) is the definitive modality for quantifying the lateralization of the tibial tubercle relative to the femoral trochlea. The TT-TG distance is measured by superimposing axial cuts of the deepest part of the trochlear groove and the center of the tibial tubercle insertion.
A normal TT-TG distance is less than 15 mm. A measurement exceeding 20 mm is considered highly abnormal and represents a significant biomechanical vector pulling the patella laterally, necessitating a bony realignment procedure.
For surgical patient positioning, the patient is placed supine on a radiolucent operating table. A proximal thigh tourniquet is applied but generally not inflated unless necessary to optimize visualization during specific osteotomy steps. A lateral post is positioned at the level of the tourniquet, and a foot roll is utilized to allow the knee to rest comfortably at 90 degrees of flexion while permitting full, unencumbered range of motion from 0 to 120 degrees. The contralateral leg is secured in a well-padded holder. Fluoroscopy must be brought in from the contralateral side, and the surgeon must confirm that perfect true lateral fluoroscopic images of the operative knee can be obtained before prepping and draping, as identifying Schöttle's point for MPFL reconstruction relies entirely on absolute radiographic precision.
Step-by-Step Surgical Approach and Fixation Technique
When conservative management has been exhausted and surgical intervention is indicated, the operative approach must meticulously address the specific pathoanatomy identified during the pre-operative workup. The most common surgical algorithm for recurrent patellofemoral instability in the setting of a normal TT-TG distance involves an isolated MPFL reconstruction. If the TT-TG exceeds 20 mm, a Tibial Tubercle Osteotomy (TTO), specifically an anteromedialization (Fulkerson osteotomy), is performed concurrently.
The procedure begins with a comprehensive diagnostic arthroscopy. Standard anterolateral and anteromedial portals are established. The surgeon meticulously evaluates the articular surfaces of the patella and trochlea, documenting the size and depth of any chondral lesions. Loose bodies are extracted. The dynamic tracking of the patella is observed as the knee is taken through a range of motion; in an unstable knee, the patella will dramatically subluxate laterally as the knee approaches terminal extension. Once the intra-articular pathology is addressed, the arthroscope is removed, and the open portions of the procedure commence.
For the MPFL reconstruction, a gracilis or semitendinosus autograft is typically harvested, though allograft is an acceptable alternative to minimize donor site morbidity. A 2-cm longitudinal incision is made over the superomedial border of the patella. The medial patellar facet is exposed, and two suture anchors are placed at the junction of the superior and middle thirds of the patella, replicating the native MPFL footprint. Alternatively, transosseous tunnels can be utilized. The graft is secured to the patella. Next, attention is turned to the femoral attachment. A 2-cm incision is made between the adductor tubercle and the medial epicondyle. Using strict true lateral fluoroscopy, Schöttle's point is identified: 1 mm anterior to the posterior cortex extension line, 2.5 mm distal to the posterior origin of the medial femoral condyle, and proximal to the level of the posterior point of Blumensaat's line. A Beath pin is drilled transversely across the femur, and a 7-mm or 8-mm reamer is used to create a socket.
The graft is passed between the second and third fascial layers of the medial knee, ensuring it remains extra-articular. The free ends of the graft are shuttled into the femoral socket. Tensioning is the most critical step of the procedure. The knee is flexed to 30 degrees, ensuring the patella is engaged in the trochlea. The graft is tensioned to restore normal medial restraint—crucially, it must not be over-tensioned. The MPFL is a checkrein, not a primary medializer; over-tensioning will cause catastrophic medial patellofemoral overload and rapid cartilage destruction. Once appropriate tension and isometric behavior are confirmed throughout the range of motion, the graft is secured in the femur with a bio-absorbable interference screw.
If a TTO is indicated, an 8-cm longitudinal incision is made just lateral to the tibial crest. The anterior compartment musculature is elevated off the lateral tibia. Using an oscillating saw, an oblique osteotomy is performed starting proximal to the tibial tubercle and exiting distally. For a Fulkerson anteromedialization, the saw blade is angled from anteromedial to posterolateral. The tubercle pedicle is mobilized, shifted medially and anteriorly by the pre-operatively calculated distance (usually 10-15 mm), and temporarily pinned. Patellar tracking is reassessed. Once optimal tracking is achieved, the osteotomy is rigidly fixed using two or three 4.5-mm fully threaded cortical lag screws directed from anterior to posterior, ensuring bicortical purchase.
Complications, Incidence Rates, and Salvage Management
The management of patellofemoral instability is fraught with potential complications, both in the conservative and operative realms. Recognizing these pitfalls early is essential for implementing effective salvage strategies and preventing long-term morbidity. The most common complication of non-operative management is recurrent instability. Despite rigorous physical therapy, up to 40% to 50% of young, active patients will experience a subsequent dislocation, leading to progressive chondral sheer injuries and the eventual development of patellofemoral osteoarthritis.
Surgical complications are often related to technical errors during reconstruction or failure to address underlying bony malalignment. The most devastating complication following MPFL reconstruction is non-anatomic femoral tunnel placement. If the femoral tunnel is placed too proximal, the graft will tighten excessively in flexion, leading to severe loss of knee flexion, medial patellar facet overload, and iatrogenic chondromalacia. If placed too distal, the graft will be loose in extension, failing to prevent lateral subluxation. Over-tensioning the graft, even if anatomically placed, occurs in up to 10% of cases and results in chronic medial-sided pain and accelerated joint degeneration. Patellar fractures are a catastrophic complication associated with creating transosseous tunnels or placing large anchors in the patella, occurring in 1% to 3% of cases.
Complications specific to Tibial Tubercle Osteotomies include delayed union or non-union (occurring in 2% to 5% of cases, particularly in smokers), proximal tibial fractures if the osteotomy cut is propagated too far proximally into the joint, and prominent hardware requiring subsequent removal. Deep vein thrombosis (DVT) and pulmonary embolism (PE) are rare but serious risks, necessitating appropriate chemical prophylaxis based on patient risk factors.
Salvage management for failed patellofemoral surgery is incredibly complex. A failed MPFL reconstruction due to malposition requires a revision reconstruction with meticulous fluoroscopic localization of the true anatomic footprint, often necessitating bone grafting of the previous tunnels. If recurrent instability persists due to unrecognized severe trochlear dysplasia (Dejour Types B or D), a complex trochleoplasty may be required to deepen the sulcus, though this procedure carries a high risk of stiffness and chondrolysis. In patients with end-stage patellofemoral osteoarthritis resulting from years of instability or iatrogenic overload, patellofemoral arthroplasty (in isolated disease) or total knee arthroplasty remains the definitive salvage procedure.
| Complication | Incidence Rate | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Instability | 10% - 20% (Post-op) | Missed TT-TG >20mm; Femoral tunnel placed too distal; Graft stretching. | Revision MPFL; Addition of TTO if bony malalignment was missed; Trochleoplasty. |
| Loss of Flexion / Stiffness | 5% - 15% | Femoral tunnel placed too proximal; Graft over-tensioning; Prolonged immobilization. | Aggressive PT; Arthroscopic lysis of adhesions; Open graft release or lengthening. |
| Patellar Fracture | 1% - 3% | Multiple/large transosseous drill holes; Eccentric anchor placement; Trauma. | Open Reduction Internal Fixation (ORIF) with tension band wiring or cannulated screws. |
| TTO Non-union | 2% - 5% | Smoking; Inadequate rigid fixation; Poor vascularity of the bony pedicle. | Revision ORIF with autologous bone grafting; Smoking cessation protocol. |
| Medial Patellar Overload | 5% - 10% | Severe over-tensioning of the MPFL graft at the time of surgery. | Arthroscopic evaluation; Graft release; Lateral retinacular reefing if over-released. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following either an acute dislocation (managed conservatively) or surgical stabilization is a highly structured, multiphase process designed to protect healing tissues while progressively restoring dynamic neuromuscular control. Prolonged immobilization is strictly avoided to prevent arthrofibrosis and profound quadriceps atrophy.
Phase I: Maximum Protection and Early Motion (Weeks 0 to 2)
In the immediate post-injury or post-operative phase, the primary goals are to control the massive inflammatory response, manage the hemarthrosis, and mitigate arthrogenic muscle inhibition. The knee is placed in a hinged brace locked in full extension for weight-bearing ambulation. Crutches are utilized to allow 50% weight-bearing, progressing to full weight-bearing as tolerated by quadriceps control. Range of motion (ROM) exercises are initiated immediately but are strictly limited from 0 to 90 degrees to prevent excessive tension on the healing MPFL or surgical graft. Quadriceps-setting exercises, straight-leg raises (SLR) in the brace, and ankle pumps are performed multiple times daily. Cryotherapy is applied aggressively.
Phase II: Progressive ROM and Early Strengthening (Weeks 2 to 6)
Once the acute effusion has subsided and the patient demonstrates a lag-free SLR, the brace is unlocked for ambulation. The goal is to achieve full, symmetric ROM by week 6. Rehabilitation heavily emphasizes closed-kinetic-chain (CKC) exercises. Open-chain quadriceps exercises (e.g., seated leg extensions) are strictly contraindicated, as they place maximal joint reaction forces on the patellofemoral articulation at terminal extension, precisely when the patella is least constrained. CKC exercises, such as wall slides and mini-squats (limited to 0 to 45 degrees), increase tibiofemoral compressive forces, paradoxically stabilizing the patellofemoral joint and recruiting hamstring co-contraction. Stationary cycling with a high seat is initiated to promote cartilage nutrition and ROM.
Phase III: Advanced Strengthening and Proprioception (Weeks 6 to 12)
During this phase, the focus shifts to maximizing vastus medialis obliquus (VMO) recruitment, core stability, and proprioception. The brace is typically discontinued. Advanced CKC exercises, including forward and lateral step-ups, lunges, and single-leg squats, are incorporated. Balance training using a BAPS board or Bosu ball is critical for restoring the neuromuscular feedback loops disrupted during the initial injury. Light jogging may be initiated toward the end of this phase, provided the patient has 80% quadriceps strength relative to the contralateral limb and absolutely no effusion.
Phase IV: Return to Play and Sport-Specific Agility (Months 3 to 6)
The final phase bridges the gap between clinical rehabilitation and athletic performance. Plyometric training, cutting drills, and sport-specific agility maneuvers are aggressively pursued. The patient may be cleared to return to full athletic activity only when quadriceps and hamstring muscle strength is at least 90% of the contralateral limb (verified via isokinetic testing), the Limb Symmetry Index (LSI) on hop testing is > 90%, and the patient demonstrates no apprehension during dynamic movements. A patellar stabilizing brace featuring a lateral J-buttress is often prescribed for the first season back to sports to provide mechanical medialization and enhanced proprioceptive feedback.
Summary of Landmark Literature and Clinical Guidelines
The evolution of patellofemoral instability management is deeply rooted in several landmark biomechanical and clinical studies that have shaped current orthopedic guidelines. Understanding this literature is essential for any surgeon treating this complex joint.
The fundamental understanding of MPFL anatomy and biomechanics was solidified by the work of Amis et al. and Sallay et al. Sallay's seminal paper demonstrated that the MPFL is torn in over 90% of acute patellar dislocations, typically at its femoral origin, fundamentally shifting the treatment paradigm away from isolated lateral releases toward anatomic medial-sided repair or
