Congenital Arteriovenous Fistulas & Hand Lesions: Surgical Guide
Key Takeaway
Congenital arteriovenous fistulas and tumor-like lesions of the hand require meticulous surgical management. This comprehensive guide details the pathophysiology, diagnostic imaging, and step-by-step operative techniques for arteriovenous fistulas, pyogenic granulomas, gouty tophi, and traumatic neuromas. Emphasizing evidence-based approaches, it provides orthopedic surgeons with critical insights into microvascular dissection, nerve transposition, and soft tissue reconstruction to optimize functional outcomes and minimize postoperative complications.
CONGENITAL ARTERIOVENOUS FISTULA
Congenital arteriovenous fistulas (CAVFs) of the upper extremity represent a complex hemodynamic and structural anomaly resulting from the embryological failure of the common vascular anlage to differentiate into distinct, mature arterial and venous channels. This arrest in vascular organogenesis yields persistent, abnormal shunts between the high-pressure arterial system and the low-pressure venous circulation, bypassing the capillary beds.
Pathophysiology and Biomechanics
The presence of these anomalous shunts drastically alters local and regional hemodynamics. The shunting of arterial blood directly into the venous system leads to localized venous hypertension, venous engorgement, and secondary varicosities. Biomechanically, the diversion of flow can induce a "steal phenomenon," wherein the distal capillary beds are deprived of adequate perfusion, leading to distal tissue ischemia, delayed wound healing, and chronic secondary ulceration.
Furthermore, the increased regional blood flow often stimulates asymmetric limb hypertrophy—both in soft tissue and bone—a hallmark of conditions such as Parkes Weber syndrome. Unlike glomus tumors, which are exquisitely painful due to their rich sympathetic innervation, uncomplicated CAVFs are typically painless. However, secondary ischemic ulcerations or localized infections can incite severe pain.
Diagnostic Evaluation
Clinical suspicion should be high in patients presenting with unilateral upper extremity varicosities, localized elevated skin temperature, palpable thrills, or continuous machinery murmurs. Minor trauma in these patients often results in disproportionate bleeding or recalcitrant ulceration.
Definitive diagnosis and surgical planning rely heavily on advanced imaging:
* Digital Subtraction Angiography (DSA): The gold standard. It reveals the precise architectural anatomy, demonstrating proximal arterial dilation, rapid and abnormal filling of the distal arterial tree, early venous opacification, and the exact location of the fistulous nidus.
* Magnetic Resonance Angiography (MRA): Provides excellent soft-tissue contrast to evaluate the extent of muscle and bone involvement without ionizing radiation.
Clinical Pearl: Always differentiate a congenital arteriovenous fistula from an acquired traumatic fistula. Congenital lesions typically feature a diffuse nidus with multiple micro-fistulous connections, whereas traumatic fistulas usually present as a single, distinct communication between a major artery and vein.
Surgical Management
The surgical eradication of CAVFs is notoriously challenging due to the microscopic and diffuse nature of the anomalous communications.
Indications for Surgery:
* Impending or active tissue necrosis (gangrene).
* Recalcitrant ischemic ulceration.
* High-output cardiac failure (rare in isolated upper extremity lesions but possible in extensive shunts).
* Severe functional impairment or uncontrollable hemorrhage.
Surgical Approach and Technique:
1. Preoperative Embolization: Often performed 24 to 48 hours prior to surgical resection to occlude major feeding vessels, thereby reducing intraoperative hemorrhage and shrinking the nidus.
2. Positioning and Tourniquet: The patient is positioned supine with the arm on a hand table. A pneumatic tourniquet is applied but may be left uninflated initially to allow visual and palpable identification of the pulsatile fistulous tracts. Once mapped, the arm is exsanguinated and the tourniquet inflated to provide a bloodless field.
3. Dissection: Utilizing loupe magnification or an operating microscope, the surgeon must meticulously trace and ligate all feeding arteries and draining veins immediately adjacent to the nidus.
4. Resection: The entire vascular malformation must be excised en bloc if possible. Partial excision inevitably leads to rapid recurrence and exacerbation of collateral flow.
5. Soft Tissue Reconstruction: Extensive resections often leave significant soft-tissue defects. Primary closure is rarely possible without undue tension. Staged procedures utilizing negative pressure wound therapy (NPWT), followed by full-thickness skin grafting or regional/free flap coverage, are frequently required.
PYOGENIC GRANULOMA (LOBULAR CAPILLARY HEMANGIOMA)
Despite its historical misnomer, a pyogenic granuloma is neither infectious (pyogenic) nor granulomatous. It is a benign, rapidly growing vascular proliferation of granulation tissue, formally classified as a lobular capillary hemangioma.
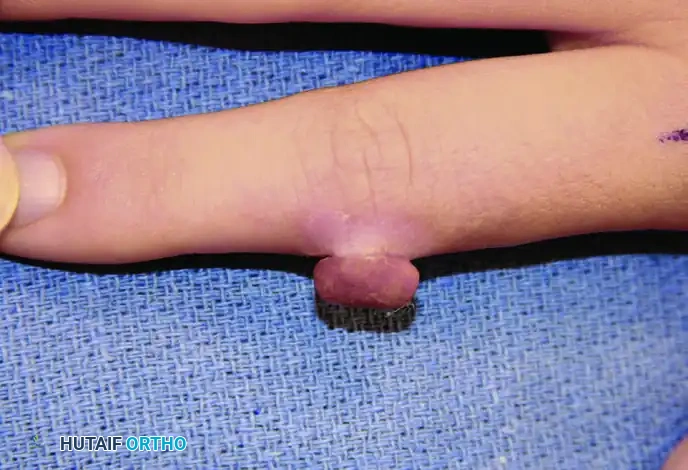
Clinical Presentation
These lesions frequently erupt on the digits following minor, often unnoticed, penetrating trauma or localized infection. They present as friable, erythematous, pedunculated, or sessile nodules that overhang the surrounding normal epidermis. Due to their unstable, highly vascular nature, they are prone to profuse, recurrent bleeding with minimal provocation.

Surgical Excision Technique
Conservative measures (e.g., silver nitrate cauterization) are associated with unacceptably high recurrence rates. Definitive management requires surgical excision.
- Anesthesia: A digital block using 1% lidocaine without epinephrine is typically sufficient.
- Excision: A simple shave excision is inadequate. The surgeon must perform a full-thickness elliptical excision that encompasses the entire exophytic lesion, the surrounding collarette of hyperplastic skin, and, crucially, the deep vascular base extending into the subcutaneous tissue.
- Closure: The defect is closed primarily with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 nylon). If the defect is too large for primary closure without tension, a small full-thickness skin graft (harvested from the hypothenar eminence or volar wrist crease) should be applied.
Surgical Warning: All excised pyogenic granulomas must be sent for histopathological examination to rule out amelanotic melanoma or squamous cell carcinoma, which can perfectly mimic this benign lesion clinically.
FOREIGN BODY GRANULOMA
A foreign body granuloma represents a chronic, localized inflammatory response to retained exogenous material (e.g., wood splinters, glass, metallic fragments, or retained suture material).
Pathophysiology
When the immune system cannot enzymatically degrade or phagocytose the foreign material, macrophages fuse to form multinucleated foreign-body giant cells. Fibroblasts are subsequently recruited, encapsulating the offending agent within a dense, firm, fibrous capsule.
Diagnosis and Management
Diagnosis is primarily clinical, driven by a meticulous history of penetrating trauma. While radiopaque materials (glass, metal) are easily identified on standard radiographs, radiolucent materials (wood, thorns) require high-resolution ultrasonography or MRI for localization.
Surgical Extirpation:
Surgical removal is curative. Under regional anesthesia and tourniquet control, an incision is made over the palpable mass. The fibrous capsule is incised, and the granulomatous tissue, along with the centralized foreign nidus, is completely excised. Thorough irrigation and debridement of the surrounding reactive tissue are mandatory before primary closure.
GOUTY ARTHROPATHY AND TOPHACEOUS DEPOSITS
Gout is a systemic disorder of purine metabolism characterized by hyperuricemia and the subsequent precipitation of monosodium urate (MSU) crystals within joints, ligaments, tendons, tendon sheaths, and subcutaneous tissues.
Pathophysiology and Radiographic Findings
In advanced, poorly controlled gout, massive tophaceous deposits accumulate. These crystals trigger a profound inflammatory cascade, activating osteoclasts and inhibiting osteoblasts, leading to aggressive, localized bone resorption.
Radiographically, this manifests as well-defined, "punched-out" lytic lesions in the metaphysis and diaphysis, often with sclerotic margins and overhanging edges of cortical bone (Martel's sign). The sheer magnitude of bone destruction can easily mimic a primary lytic bone tumor or chronic osteomyelitis.

Clinically, acute flares present with intense erythema, calor (heat), swelling, and exquisite tenderness, closely mimicking an acute pyogenic infection. Aspiration and polarized light microscopy (revealing negatively birefringent needle-shaped crystals) definitively establish the diagnosis.
Surgical Management
While gout is primarily managed medically, surgical intervention is indicated in specific scenarios:
* Severe pain and functional limitation due to mechanical block.
* Impending or actual skin necrosis and ulceration over a massive tophus.
* Compression neuropathies (e.g., carpal tunnel syndrome caused by flexor tenosynovial tophi).
* Joint destruction requiring arthrodesis or arthroplasty.
Surgical Technique:
1. Approach: Incisions must be planned carefully, as the skin overlying large tophi is often attenuated, ischemic, and prone to postoperative necrosis.
2. Debridement: Tophi are meticulously enucleated. The chalky, toothpaste-like urate deposits are curetted from the bone and soft tissues.
3. Tendon Preservation: When debriding intratendinous tophi, extreme care must be taken to preserve the continuity of the tendon and its paratenon. Aggressive resection can lead to iatrogenic tendon rupture.
4. Closure: Dead space must be minimized. If the overlying skin is non-viable, it must be excised, and the wound left to heal by secondary intention or covered with a local flap.
TRAUMATIC NEUROMA
A traumatic neuroma is not a true neoplasm; rather, it is a disorganized, hyperplastic proliferation of axons, Schwann cells, and perineurial fibroblasts that occurs following the complete or partial transection of a peripheral nerve.
Pathophysiology
Following nerve injury, the distal segment undergoes Wallerian degeneration. The proximal stump attempts to regenerate, sending out axonal growth cones. If these regenerating fibers cannot bridge the gap to the distal stump—due to scar tissue, wide separation, or amputation—they coil into a tangled, bulbous mass at the distal end of the proximal nerve segment.
Clinical Evaluation
Neuromas are typically invisible to the naked eye but are exquisitely tender. They are most problematic when located superficially, such as a digital nerve neuroma adhering to an amputation stump lacking adequate subcutaneous padding. Diagnosis is confirmed by eliciting a localized Tinel's sign—sharp, radiating, electric-shock-like pain upon tapping the suspected area with a firm, pinpoint object (e.g., a pencil point).
Surgical Management
The goal of surgery is not to prevent neuroma formation (which is a physiological inevitability of a cut nerve) but to relocate the neuroma to a protected, asymptomatic environment.
Surgical Techniques:
1. Resection and Transposition: The neuroma is sharply excised back to healthy fascicular tissue. The proximal nerve stump is then mobilized and buried deep within a well-vascularized muscle belly (e.g., transposing a superficial radial nerve neuroma into the brachioradialis) or implanted into a drilled hole in adjacent bone. This shields the regenerating nerve ending from mechanical stimulation.
2. Centrocentral Anastomosis: If two adjacent neuromas exist, they can be resected and the proximal stumps coapted to one another, creating a closed loop that inhibits further axonal outgrowth.
3. Targeted Muscle Reinnervation (TMR): In amputees, the proximal nerve stump can be transferred to a nearby redundant motor branch of a muscle, providing the regenerating axons with a physiological target and significantly reducing phantom limb and neuroma pain.
Surgical Pitfall: Simply resecting a neuroma and leaving the stump in the same subcutaneous bed guarantees recurrence of symptoms. The nerve ending must be transposed to a protected environment.
RARE NEUROPATHIES AND CALCINOSIS
Déjérine-Sottas Disease
Déjérine-Sottas disease (Charcot-Marie-Tooth disease type 3) is a rare, severe, early-onset hypertrophic interstitial neuropathy. It is characterized by extensive demyelination and remyelination, leading to "onion bulb" formations of Schwann cells. In the upper extremity, it may present as a palpable, tender, localized enlargement of a peripheral nerve, most commonly at the wrist, mimicking a localized tumor or severe compressive neuropathy. Surgical intervention is rarely indicated unless severe, localized compression requires decompression.
Calcinosis Circumscripta
Calcinosis circumscripta involves the deposition of insoluble calcium phosphate lobules within the skin and subcutaneous tissues. The exact pathological mechanism remains elusive, though it is frequently associated with autoimmune connective tissue disorders, particularly the CREST variant of scleroderma (where it is preceded by years of Raynaud's phenomenon).
Deposits densely aggregate over pressure points, such as the volar fingertips, causing severe pain and mechanical interference with grip. The calcific nodules may eventually erode through the ischemic skin, leading to chronic, draining ulcerations and secondary osteomyelitis of the distal phalanx.
Surgical Considerations:
Surgical extirpation is indicated when deposits cause intractable pain, functional deficit, or skin breakdown. However, the surgeon must exercise extreme caution. The surrounding soft tissues in these patients are typically profoundly ischemic due to underlying microvascular disease (Raynaud's). Extensive surgical dissection frequently results in catastrophic wound breakdown, delayed healing, and skin necrosis. Therefore, surgery should be strictly limited to the conservative, partial excision of the most prominent, symptomatic calcific lobules, prioritizing the preservation of the delicate vascular supply to the skin flaps.
You Might Also Like
