Arthroscopic Femoroacetabular Impingement: A Masterclass in Hip Preservation

Key Takeaway
Welcome, fellows, to an immersive masterclass in arthroscopic femoroacetabular impingement (FAI) management. We'll navigate comprehensive surgical anatomy, meticulous preoperative planning, and precise intraoperative execution. Learn to identify and address cam and pincer lesions, perform labral repair, and reshape the femoral head-neck junction. This session emphasizes critical pearls, pitfalls, and integrated postoperative protocols for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Femoroacetabular impingement (FAI) represents a profound paradigm shift in our understanding of hip preservation and the etiology of premature hip osteoarthritis. Historically relegated to an ambiguous category of "idiopathic" hip pain, FAI is now universally recognized by orthopedic surgeons as a dynamic, structural conflict—a precise mechanical mismatch between the proximal femur and the acetabular rim. If left unaddressed, this relentless abutment inexorably leads to progressive chondral delamination, labral tearing, and ultimately, end-stage osteoarthritis requiring arthroplasty. The foundational work by Ganz and colleagues elucidated that osteoarthritis of the hip is rarely truly idiopathic; rather, it is frequently the terminal result of subtle morphological abnormalities triggering decades of abnormal contact stresses.
The epidemiology of FAI reveals a strong predilection for young, active populations, though it is increasingly recognized across all demographics. The prevalence of asymptomatic cam morphology in the general population is surprisingly high, approaching 30% in some cohorts, and even higher in elite athletes participating in sports requiring repetitive hip flexion and internal rotation (e.g., ice hockey, soccer, martial arts). This suggests that while morphology is a prerequisite, the syndrome of FAI requires the convergence of susceptible anatomy, specific kinematic demands, and resultant tissue failure. Furthermore, we must maintain a high index of suspicion for underlying pediatric hip pathologies that subtly alter joint mechanics, such as mild slipped capital femoral epiphysis (SCFE), Legg-Calvé-Perthes disease, or residual acetabular dysplasia.
Our definitive goal with arthroscopic management is not merely palliative pain relief, but the meticulous restoration of normal hip mechanics. By reshaping the osseous anatomy to eliminate impingement and surgically repairing the vital capsulolabral stabilizers, we aim to alter the natural history of the joint, preserve the native articular cartilage, and extend the functional lifespan of the hip. Arthroscopy has evolved from a diagnostic tool to a sophisticated therapeutic intervention, allowing for comprehensive joint reconstruction with minimized morbidity.
Pathomechanics of Pincer and Cam Impingement
The pathomechanics of FAI are classically dichotomized into pincer and cam mechanisms, though isolated presentations are exceedingly rare; the vast majority of our surgical patients present with a mixed impingement pattern. Understanding the distinct biomechanical consequences of each is critical for targeted surgical intervention.
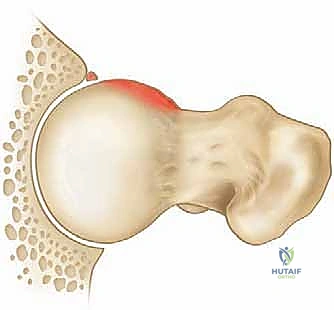
Cam impingement is fundamentally a problem of femoral head asphericity. The abnormal, non-spherical prominence at the anterolateral femoral head-neck junction acts as a literal "cam," jamming into the confined space of the acetabulum during terminal hip motion, particularly in flexion and internal rotation. This creates massive shear forces directed against the anterosuperior acetabular cartilage. The predictable consequence is an outside-in delamination of the articular cartilage from the subchondral bone, often leaving the labrum initially intact but destabilized, eventually leading to labral detachment or complex tearing. Common etiologies include the "pistol grip" deformity, subclinical SCFE, femoral retroversion, and malunited femoral neck fractures.
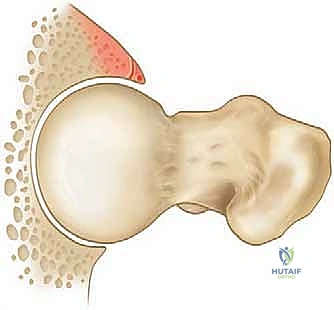
Conversely, pincer impingement represents an "overcoverage" phenomenon, where an abnormal, prominent acetabular rim prematurely contacts a morphologically normal femoral head-neck junction. This abnormal contact creates a linear crushing force directly against the acetabular labrum. The pathology here typically manifests as labral bruising, intrasubstance tearing, and eventual ossification of the labrum itself, effectively extending the bony rim and exacerbating the impingement. Furthermore, the levering effect of the femoral neck against the anterior rim can subluxate the femoral head posteriorly, creating a classic "contrecoup" chondral lesion on the posteroinferior acetabulum. Pincer morphology is frequently driven by a deep acetabulum (coxa profunda, protrusio acetabuli) or focal anterior overcoverage due to acetabular retroversion.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical approach, a profound, three-dimensional command of hip anatomy is non-negotiable. The hip joint is a masterpiece of evolutionary engineering, balancing immense weight-bearing stability with a vast, multi-planar range of motion. We must navigate this space with extreme precision, respecting the delicate interplay between osteology, capsuloligamentous restraints, and neurovascular networks.
The osteology dictates the mechanical boundaries of the joint. The normal acetabulum is anteverted approximately 12 to 16.5 degrees and abducted roughly 40 degrees. It is designed to perfectly cradle the femoral head, distributing loads across the sourcil—the crescent-shaped, superior weight-bearing zone of dense subchondral bone. The proximal femur must possess a spherical head and a concave neck to allow impingement-free clearance. The normal femoral neck-shaft angle ranges from 120 to 135 degrees, with an anteversion of 12 to 15 degrees. Deviations such as coxa vara or femoral retroversion drastically reduce the clearance space, precipitating impingement even in the absence of a discrete cam lesion.

The capsuloligamentous complex of the hip is robust and biomechanically vital. The capsule is reinforced by three primary ligaments: the iliofemoral (the strongest ligament in the human body, resisting extension and external rotation), the pubofemoral (resisting abduction and extension), and the ischiofemoral (resisting internal rotation). Deep to these lies the zona orbicularis, a circumferential collar of capsular fibers acting as a locking ring around the femoral neck, crucial for distraction stability. Iatrogenic injury or failure to repair these structures during arthroscopy, particularly the iliofemoral ligament, is a leading cause of devastating postoperative microinstability and catastrophic subluxation.

The acetabular labrum is a continuous fibrocartilaginous ring spanning the acetabular rim, bridged inferiorly by the transverse acetabular ligament. It is not merely a bumper; it deepens the socket by 21%, increases the surface area by 28%, and critically, creates a highly pressurized fluid seal. This "suction seal" effect maintains a layer of synovial fluid between the articular surfaces, distributing loads evenly and protecting the underlying cartilage from focal point-loading. Loss of this seal due to tearing or aggressive surgical resection accelerates joint degeneration exponentially.

Neurovascular Considerations and Portal Anatomy
The vascular supply to the proximal femur is the most critical anatomical constraint during femoral osteoplasty. The retinacular vessels, primarily the lateral epiphyseal vessels, provide the terminal blood supply to the femoral head. They originate from the medial circumflex femoral artery, ascend the posterior and superior aspects of the femoral neck within the synovial reflections (retinacula of Weitbrecht), and penetrate the femoral head just distal to the articular cartilage.

Aggressive resection of the femoral neck, particularly in the posterosuperior quadrant, risks transecting these vessels, leading to iatrogenic avascular necrosis (AVN) of the femoral head—a catastrophic complication. The safe zone for cam resection is generally confined to the anterolateral and anterior quadrants, strictly avoiding the posterior superior retinacular vessels.

Arthroscopic access relies on precise portal placement through safe muscular intervals. The standard Anterolateral (AL) portal is established 1-2 cm proximal and 1-2 cm anterior to the tip of the greater trochanter, passing through the gluteus medius. The Anterior (A) portal or Mid-Anterior Portal (MAP) is typically placed distal and slightly lateral to the anterior superior iliac spine (ASIS), utilizing the interval between the tensor fasciae latae (TFL) laterally and the sartorius/rectus femoris medially.

When establishing anterior portals, the lateral femoral cutaneous nerve (LFCN) is at significant risk. The LFCN typically branches extensively as it courses distally over the anterior thigh. To minimize injury, anterior portals should be made with superficial skin incisions only, followed by blunt dissection with a hemostat down to the capsule.

Exhaustive Indications and Contraindications
Patient selection is the absolute determinant of success in hip arthroscopy. The ideal candidate is a young, active patient presenting with insidious onset, activity-related groin pain that is exacerbated by deep flexion and internal rotation. The classic "C-sign," where the patient cups their hand over the greater trochanter with the thumb posterior and fingers deep in the anterior groin, is a hallmark presentation. Mechanical symptoms such as clicking, catching, or giving way strongly suggest labral tearing or loose bodies.
Physical examination must be rigorous. The Anterior Impingement Test (FADIR: Flexion, Adduction, Internal Rotation) is highly sensitive for anterolateral rim pathology. The FABER test (Flexion, Abduction, External Rotation) often elicits posterior pain or demonstrates restricted mobility compared to the contralateral side. Diagnostic intra-articular injections of local anesthetic (often performed concurrently with MR arthrography) are paramount; near-complete temporary relief of provocative pain confirms the hip joint as the primary pain generator, effectively ruling out extra-articular mimics like athletic pubalgia, core muscle injuries, or lumbar radiculopathy.
Arthroscopic intervention is indicated when patients have radiographically confirmed FAI morphology, concordant clinical exams, and have failed a comprehensive trial of conservative management (activity modification, physical therapy focusing on core and pelvic stabilization, NSAIDs). Crucially, the joint must exhibit minimal to no degenerative changes. Arthroscopy is a joint-preserving procedure; it is explicitly not a salvage operation for advanced osteoarthritis.
| Parameter | Indications for Arthroscopic FAI Surgery | Absolute/Relative Contraindications |
|---|---|---|
| Clinical | Symptomatic FAI failing >3 months non-op care; Positive FADIR/FABER; Positive diagnostic injection. | Medically unfit for surgery; Active joint infection; Severe psychiatric overlay. |
| Radiographic | Alpha angle > 55°; LCEA > 40° (Pincer) or normal; Crossover sign present. | Tönnis Grade 2 or 3 OA; Joint space < 2mm on AP/False Profile views. |
| Morphologic | Cam, Pincer, or Mixed morphology; Labral tears; Focal chondral defects. | Severe Acetabular Dysplasia (LCEA < 20°); Global protrusio acetabuli. |
| Biomechanical | Preserved capsular integrity; Correctable version abnormalities. | Severe femoral retroversion (< 5°) requiring derotational osteotomy. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning separates the master surgeon from the technician. It requires a comprehensive synthesis of plain radiography, advanced cross-sectional imaging, and three-dimensional conceptualization.
Plain radiographs remain the cornerstone of evaluation. A well-centered AP pelvis (coccyx pointing to the symphysis with a 1-2 cm gap) is mandatory to assess acetabular version. We evaluate the Lateral Center Edge Angle (LCEA) to distinguish between dysplasia (<25°), normal coverage (25-40°), and pincer overcoverage (>40°).
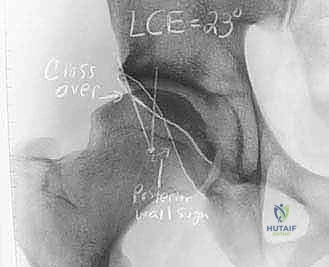
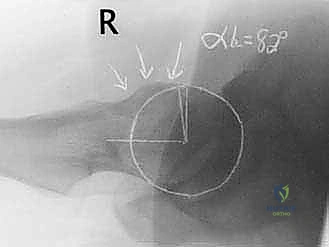
The presence of a crossover sign (anterior wall crossing lateral to the posterior wall) or a prominent ischial spine sign indicates acetabular retroversion. For the proximal femur, a Dunn 45° view or a cross-table lateral view is essential to calculate the alpha angle. An alpha angle exceeding 50-55 degrees suggests a pathological cam lesion.
Magnetic Resonance Arthrography (MRA) with gadolinium is the gold standard for evaluating the intra-articular soft tissues. MRA provides exquisite detail of the acetabular labrum, allowing us to classify tears (e.g., radial flap, longitudinal peripheral, intrasubstance) and accurately map chondral delamination.
Furthermore, MR imaging frequently reveals synovial herniation pits (Pitt's pits) at the anterior femoral head-neck junction, which are strongly correlated with chronic cam impingement. In complex or revision cases, a 3D CT scan with surface rendering is invaluable for precise topographic mapping of the cam lesion and volumetric assessment of acetabular version.

Operating Room Setup and Patient Positioning
Proper patient positioning is the foundation of safe access. While some surgeons prefer the lateral decubitus position, the supine position on a specialized hip distraction table is the most widely utilized technique globally, offering excellent anatomical orientation and simplified fluoroscopic access.

The patient is positioned supine with the perineal post placed firmly against the medial thigh of the operative leg, lateralizing the vector of traction to distract the femoral head laterally rather than purely longitudinally. This lateralization is critical to overcome the suction seal and the robust iliofemoral ligament without applying excessive, nerve-damaging force. The operative leg is placed in slight flexion (10-15 degrees) to relax the anterior capsule, neutral abduction, and 10-15 degrees of internal rotation to present the femoral neck horizontally.

A massive, oversized, well-padded perineal post is mandatory to distribute pressure and prevent devastating pudendal neurapraxia. Traction should be applied slowly and deliberately, allowing the viscoelastic capsular tissues to creep. We utilize fluoroscopy to confirm adequate joint distraction (ideally 10-12 mm of joint space) before attempting portal placement, ensuring instruments do not scuff the pristine articular cartilage.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of FAI arthroscopy is a highly choreographed sequence divided into central compartment (intra-articular) and peripheral compartment (extra-articular, intra-capsular) phases.
We begin with central compartment access. Under fluoroscopic guidance, a spinal needle is introduced into the joint via the intended Anterolateral (AL) portal. The joint is vented by injecting 20-30 cc of normal saline, breaking the suction seal and facilitating further distraction. A nitinol wire is passed, followed by a cannulated switching stick and a 5.0mm or 5.5mm arthroscope.

Once intra-articular, the Mid-Anterior Portal (MAP) is established under direct visualization to avoid iatrogenic labral or chondral injury. An interportal capsulotomy is then performed, connecting the AL and MAP portals parallel to the labrum, typically 5-8 mm away from the rim. This capsulotomy dramatically improves instrument mobility and visualization.

A comprehensive diagnostic arthroscopy is performed, probing the labrum, assessing the ligamentum teres, and meticulously grading the acetabular and femoral chondral surfaces (Outerbridge classification).

Acetabuloplasty and Labral Repair
If pincer impingement is present, an acetabuloplasty is performed. The labrum is carefully elevated from the acetabular rim (takedown), preserving its chondrolabral junction if possible. A motorized burr is introduced to resect the bony overcoverage, effectively retroverting the anterior rim to a neutral profile.

Care must be taken not to over-resect, which induces iatrogenic dysplasia. The resected rim provides a bleeding, cancellous bone bed, optimizing the biological environment for subsequent labral healing.

Labral repair is prioritized over debridement to restore the critical suction seal. Suture anchors (typically 1.5mm to 2.9mm) are placed precisely on the acetabular rim, angled away from the articular surface to prevent joint penetration.

Sutures are passed around or through the labrum using specialized curved or straight suture passing devices. Base-refixation techniques or looped stitches are utilized to securely re-approximate the labrum to the bony rim, tensioning it to recreate the fluid seal against the femoral head.

Peripheral Compartment and Femoral Osteoplasty
Following central compartment work, traction is completely released. The hip is flexed to 30-45 degrees to relax the anterior capsule, allowing the arthroscope to be advanced into the peripheral compartment.

The cam lesion is visually identified as a distinct bony prominence covered by reactive fibrocartilage. A T-capsulotomy or extension of the interportal capsulotomy distally along the femoral neck may be required for adequate exposure of large lesions.
Femoral osteoplasty is performed using a high-speed burr, systematically resecting the cam deformity to restore a spherical head and a concave, offset head-neck junction. Resection typically extends from the anteroinferior neck, across the anterior quadrant, to the anterolateral and superolateral neck. Constant fluoroscopic checks (dynamic frog-leg and AP views) are mandatory to confirm adequate resection depth and contour. The golden rule of osteoplasty is to resect no more than 30% of the femoral neck diameter to prevent catastrophic post-operative femoral neck fractures. Finally, meticulous capsular closure is performed using heavy, non-absorbable sutures to restore the iliofemoral ligament's integrity and prevent microinstability.
Complications, Incidence Rates, and Salvage Management
While arthroscopic hip preservation is highly successful, it is a technically demanding procedure with a steep learning curve. Complications, though relatively infrequent (reported overall incidence of 1.5% to 5%), can be devastating and require immediate recognition and skilled salvage management.

Neurological injuries are the most common complications, primarily related to traction. Pudendal neurapraxia (manifesting as perineal numbness or sexual dysfunction) is directly correlated with traction time and perineal post pressure. Traction must be strictly limited to less than 2 hours, and the post must be meticulously padded. The Lateral Femoral Cutaneous Nerve (LFCN) is at risk during anterior portal placement; superficial incisions and blunt dissection are preventative.
Sciatic and femoral nerve palsies are rare but can occur with excessive distraction or extravasation of arthroscopic
Clinical & Radiographic Imaging Archive




