Navigating the Anatomy of the Ilioinguinal in Acetabular Surgery

Key Takeaway
Your ultimate guide to Navigating the Anatomy of the Ilioinguinal in Acetabular Surgery starts here. The anatomy of the ilioinguinal approach involves two main areas: lateral and posterior to the anterior superior iliac spine, requiring subperiosteal dissection of muscles from the iliac crest; and medial and anterior to the ASIS, focusing on the inguinal canal and its related structures. Key landmarks include the ASIS, iliac crest, and pubic tubercle, guiding surgeons through potentially hazardous abdominal wall anatomy to access the acetabulum.
Introduction and Epidemiology
Acetabular fractures represent complex injuries, frequently resulting from high-energy trauma such as motor vehicle collisions, falls from height, or severe crushing injuries. With an increasing global burden of trauma and an aging population, the incidence of acetabular fractures is on the rise, presenting orthopaedic surgeons with challenging reconstructive problems. These fractures often involve critical articular surfaces, necessitating precise anatomical reduction and stable internal fixation to restore joint congruity and minimize the risk of post-traumatic osteoarthritis.
The ilioinguinal approach, meticulously described by Emile Letournel, is a foundational anterior surgical corridor for addressing fractures involving the anterior column, anterior wall, and specific associated patterns of the acetabulum. Its development revolutionized the management of these complex injuries, providing unparalleled access to the inner table of the ilium, the quadrilateral surface, the superior pubic ramus, and the symphysis. This approach, while highly effective, traverses the intricate anatomy of the inguinal region, an area often less familiar to orthopaedic surgeons compared to general surgeons. A thorough understanding of the regional anatomy, including the neurovascular structures and the contents of the inguinal canal, is paramount to optimize surgical outcomes and mitigate potential complications. This discourse aims to provide an exhaustive review of the ilioinguinal approach, emphasizing its applied surgical anatomy, technical nuances, and management considerations for orthopaedic surgeons, residents, and medical students.
Surgical Anatomy and Biomechanics
The applied anatomy of the ilioinguinal approach is conveniently divided into two parts, dictated by the critical landmark of the anterior superior iliac spine (ASIS). Understanding these divisions is fundamental to navigating the surgical field effectively and safely.
Lateral and Posterior Dissection Considerations
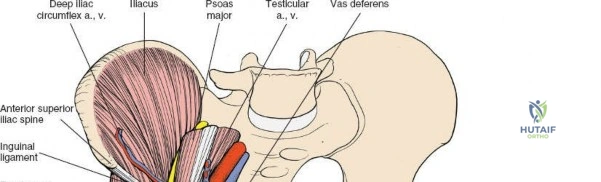
Lateral and posterior to the anterior superior iliac spine, the primary objective is the subperiosteal dissection of muscles arising from or inserting into the iliac crest and the inner wall of the ilium. This phase exposes the iliac fossa and the inner aspect of the pelvic brim. Key structures encountered in this region include the origins of the tensor fasciae latae, external oblique, and internal oblique muscles from the iliac crest.
The anterior superior iliac spine is the site of attachment to two important structures: the sartorius muscle takes its origin from it, and the inguinal ligament uses it as a lateral attachment.
The anterior third of the iliac crest serves as the origin of the following three muscles:
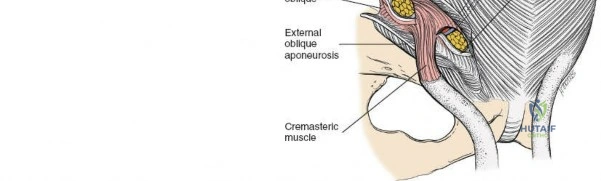
1. The external oblique forms the outer layer of the muscles of the anterior abdominal wall. It inserts into the outer strip of the anterior half of the iliac crest.
2. The internal oblique forms the middle layer of the muscles of the anterior abdominal wall. It originates from the center strip of the anterior half of the iliac crest.
3. The tensor fasciae latae arises from the outer lip of the anterior half of the iliac crest.
Subperiosteal elevation of these muscles from the iliac crest exposes the underlying bone. The iliacus muscle originates from the iliac fossa and is likewise elevated subperiosteally to expose the anterior aspect of the inner table of the ilium and the anterior column of the acetabulum. The lateral femoral cutaneous nerve (LFCN) typically courses over the iliacus muscle, approximately 2-3 cm medial to the ASIS, and requires careful identification and protection to prevent iatrogenic injury.
Medial and Anterior Dissection Considerations
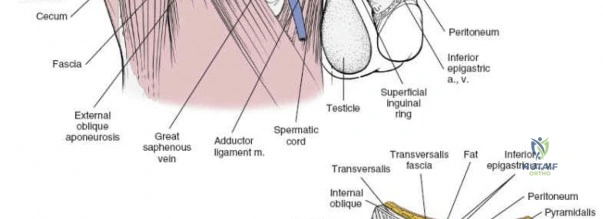
Medial and anterior to the anterior superior iliac spine, the applied anatomy of the approach is that of the inguinal canal and its related structures. Because pathology in this area nearly always relates to herniae, both inguinal and femoral, it is usually an unfamiliar ground for orthopedic surgeons and, thus, is potentially hazardous.
This region encompasses the complex arrangement of the abdominal wall musculature, the inguinal ligament, and the neurovascular bundle of the femoral triangle. A detailed understanding of these structures is critical for safe surgical execution.
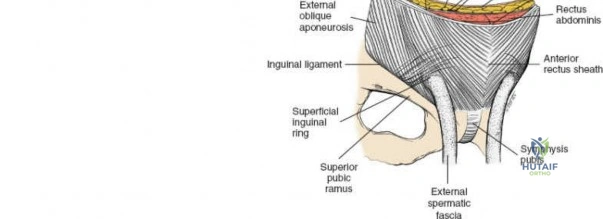
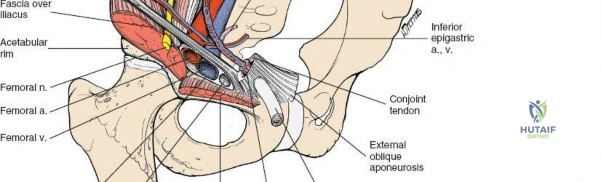
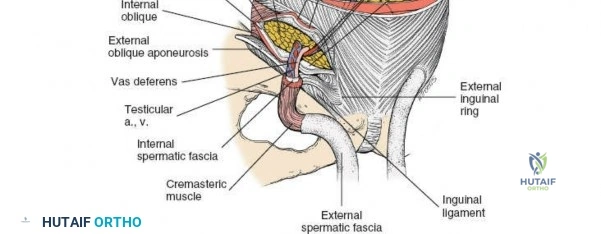
The inguinal ligament extends from the ASIS to the pubic tubercle, forming the floor of the inguinal canal. Superior to the ligament, the aponeuroses of the external oblique, internal oblique, and transversus abdominis muscles form the anterior and posterior walls of the inguinal canal.
The pubic tubercle is not easily palpated because it is covered by the spermatic cord in the male and the round ligament in the female.
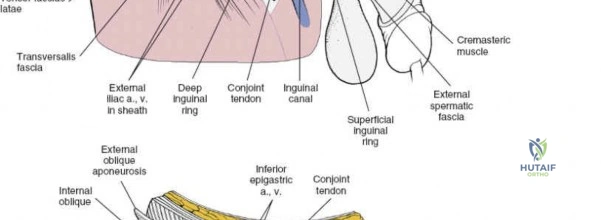
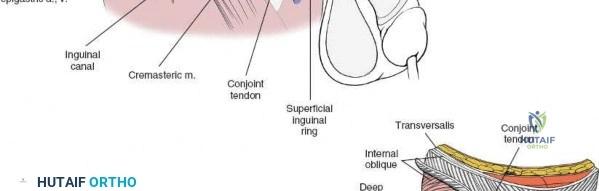
The contents of the inguinal canal differ between sexes. In males, it contains the spermatic cord (vas deferens, testicular artery, pampiniform plexus, nerves, lymphatics) and the ilioinguinal nerve. In females, it contains the round ligament of the uterus and the ilioinguinal nerve. These structures must be identified, mobilized, and protected.
Neurovascular Structures of the Inguinal Region
Several vital neurovascular structures are in close proximity to the surgical field and demand meticulous identification and protection:
- Femoral Nerve: Originating from the lumbar plexus (L2-L4), it courses beneath the inguinal ligament, lateral to the femoral artery. It supplies the quadriceps femoris and provides sensory innervation to the anterior thigh and medial leg. Injury can result in quadriceps weakness and sensory deficits.
- Femoral Artery and Vein: These major vessels pass beneath the inguinal ligament, medial to the femoral nerve. The femoral artery typically lies lateral to the femoral vein (medial to the artery). They are encased within the femoral sheath and are crucial to identify and protect to avoid catastrophic hemorrhage.
- Lateral Femoral Cutaneous Nerve (LFCN): Typically exits the pelvis medial to the ASIS and passes superficial to the sartorius muscle, supplying sensory innervation to the lateral thigh. It is highly susceptible to traction or direct injury during dissection, leading to meralgia paresthetica.
- Ilioinguinal Nerve: Arises from the lumbar plexus (L1) and typically courses within the inguinal canal, often exiting through the superficial inguinal ring. It provides sensory innervation to the skin of the pubic region, anterior scrotum/labium majus, and medial thigh. It is at risk during incision and dissection of the inguinal canal.
- Genitofemoral Nerve: Also from the lumbar plexus (L1, L2), it divides into a genital branch (traverses the inguinal canal with the spermatic cord/round ligament) and a femoral branch (travels with the femoral artery). Both branches provide sensory and motor innervation (cremasteric reflex via genital branch).
- Corona Mortis: This anatomical variant refers to an aberrant obturator artery or vein that crosses the superior pubic ramus, often in close proximity to the pubic symphysis. It connects the external iliac or inferior epigastric vessels to the obturator vessels and can be a significant source of hemorrhage if transected inadvertently. Its presence should be evaluated preoperatively with advanced imaging.
Surgical Windows of the Ilioinguinal Approach
Letournel conceptualized the ilioinguinal approach as providing access through three distinct windows, offering comprehensive exposure to the anterior column and medial wall of the acetabulum:
-
Lateral Window (Iliac Fossa Window): This window provides access to the inner table of the ilium from the ASIS to the sacroiliac joint. It is created by subperiosteal elevation of the iliacus muscle from the iliac fossa.

Structures exposed: Inner table of the ilium, sacroiliac joint, anterior aspect of the quadrilateral surface, anterior inferior iliac spine (AIIS). The iliacus muscle, covered by its fascia, is carefully elevated.The LFCN is typically located superficial to the iliacus muscle and must be protected.
This window is ideal for reducing and fixing fractures involving the iliac wing, high anterior column, and for placement of a plate along the pelvic brim.
-
Middle Window (Vascular Window): Located between the lateral border of the femoral nerve laterally and the femoral artery/vein medially.

This narrow, delicate corridor provides access to the psoas muscle, pectineus muscle, and the superior pubic ramus.
Structures exposed: Superior pubic ramus, superior part of the quadrilateral surface, obturator externus.

Careful retraction of the femoral nerve (laterally) and femoral vessels (medially) is essential. A plate can be passed through this window to stabilize the superior pubic ramus or the anterior column. -
Medial Window (Pubic Window): Located medial to the femoral artery and vein, extending to the pubic symphysis.
This window exposes the anterior surface of the pubic bone, the pubic symphysis, and the obturator canal.
Structures exposed: Anterior surface of the pubic body, pubic symphysis, superior pubic ramus, and the obturator foramen. The space of Retzius (preperitoneal space) is entered, allowing access to the bladder and structures around the pubic symphysis.The spermatic cord/round ligament and ilioinguinal nerve are retracted laterally. The obturator vessels and nerve within the obturator canal are visualized posteriorly. This window is critical for addressing fractures extending to the pubic symphysis or involving the anterior column and obturator ring.
Biomechanical Relevance
The anterior column and anterior wall are critical load-bearing structures of the acetabulum, contributing significantly to its overall stability. Fractures in this region can lead to joint incongruity, instability, and long-term disability. The ilioinguinal approach provides direct visualization and access for anatomical reduction of these fragments, facilitating stable fixation with precontoured plates and screws. The ability to place fixation along the pelvic brim, the quadrilateral surface, and the superior pubic ramus through these windows allows for robust construct biomechanics essential for early mobilization and favorable patient outcomes.
Indications and Contraindications
The ilioinguinal approach is a powerful tool for acetabular fracture management, but its application must be judiciously determined based on fracture morphology, patient factors, and surgeon expertise.
Indications for Ilioinguinal Approach
The primary indications for the ilioinguinal approach are fracture patterns involving the anterior column and/or anterior wall of the acetabulum where anatomical reduction and stable fixation are required. Specific fracture types amenable to this approach include:
- Anterior Column Fractures: These fractures involve the iliopectineal line, extending from the iliac crest or gluteal notch through the ASIS, AIIS, and superior pubic ramus.
- Anterior Wall Fractures: Isolated fractures of the anterior wall, often associated with hip dislocation.
- Associated Anterior Column and Posterior Hemi-transverse Fractures: This pattern often necessitates an anterior approach for the anterior column component, with potential for reduction of the posterior hemi-transverse component via the same approach or a combined approach.
- Transverse Fractures: Especially those with significant anterior displacement or involvement of the anterior articular surface, where primary reduction is achieved anteriorly.
- T-Type Fractures: When the primary displacement is anterior, or the anterior column component is irreducible via other approaches.
- Both Column Fractures: In selected cases, particularly when the main displacement is anterior and the posterior column can be addressed simultaneously or with a staged posterior approach.
- Irreducible Fractures: Fractures that cannot be adequately reduced via closed means or other open approaches due due to interposition of soft tissues or complex fragment interactions.
- Congruent but Displaced Fractures: Fractures where the articular surface is maintained but the entire fragment is displaced, requiring surgical reduction and fixation.
Contraindications for Ilioinguinal Approach
Contraindications can be absolute or relative, guiding the surgeon's decision-making process to ensure patient safety and optimal outcomes.
-
Absolute Contraindications:
- Unstable Patient Hemodynamics: In a polytrauma setting, immediate life-saving interventions take precedence over definitive fracture fixation.
- Active Local Infection: Presence of cellulitis, open wounds, or abscess in the operative field.
- Severe Comorbidities: Patients with high anesthetic risk or comorbidities precluding major surgery.
- Extensive Posterior Wall or Posterior Column Involvement: Where the primary instability or displacement is posterior and cannot be adequately addressed via the anterior approach.
- Insufficient Surgeon Experience: Complex acetabular surgery requires specialized training and experience.
-
Relative Contraindications:
- Obesity: May increase technical difficulty, prolong operative time, and heighten complication rates.
- Extensive Scarring: Previous abdominal surgery or trauma in the inguinal region may complicate dissection.
- Delay in Presentation: Chronic fractures (typically >3 weeks) with established callus formation are significantly more challenging to reduce.
- Significant Bone Loss or Comminution: May limit the ability to achieve stable fixation.
- Pre-existing Hernia: May complicate the approach and potentially lead to new or recurrent hernia formation.
Operative versus Non-Operative Indications
The decision to proceed with operative or non-operative management for acetabular fractures is multifaceted and depends on several factors, including fracture stability, articular congruity, patient age, functional demands, and associated injuries.
| Indication Type | Criteria for Operative Management | Criteria for Non-Operative Management |
|---|---|---|
| Fracture Pattern | Displaced anterior column, anterior wall, associated anterior column posterior hemi-transverse, transverse, T-type fractures where anatomical reduction is critical for joint congruity. Articular incongruity >2mm, joint instability. | Minimally displaced or undisplaced fractures (articular step-off <2mm). Stable acetabular roof arc measurements (anterior and posterior roof arcs >45 degrees). Non-weight bearing area fractures. |
| Patient Factors | Young, active patients with high functional demands. Absence of severe comorbidities. | Elderly, low-demand patients with significant comorbidities (e.g., severe osteoporosis, multiple medical issues) where surgical risks outweigh potential benefits. Non-ambulatory patients. |
| Associated Injury | Displaced intra-articular fragments, incarcerated osteochondral fragments, nerve impingement. | No significant associated injuries requiring immediate surgical intervention. |
| Reducibility | Irreducible fractures via closed means or with significant soft tissue interposition. | Easily reducible via closed means with stable maintenance of reduction. |
| Prognosis | Goal to preserve native hip joint and achieve long-term functional outcomes. | Consideration for potential post-traumatic arthritis with conservative management, but deemed acceptable given patient's overall health and functional expectations. |
| Special Cases | Open fractures (after debridement and stabilization), fracture-dislocations that remain unstable after reduction, floating hip. | Both-column fractures in elderly patients treated with primary total hip arthroplasty (THA) in selected cases, though this is a surgical approach, it's not internal fixation of the fracture. Certain stable acetabular dome fractures where the posterior column is intact and weight-bearing axis is preserved. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful acetabular fracture surgery via the ilioinguinal approach. This meticulous preparation minimizes intraoperative surprises and optimizes surgical execution.
Preoperative Imaging and Fracture Analysis
High-quality imaging is essential for accurate fracture classification and planning:
* Plain Radiographs: Anteroposterior (AP) view of the pelvis, Judet oblique views (obturator oblique and iliac oblique) are the standard initial workup. These views help identify specific fracture lines and their extent, allowing for preliminary classification according to Letournel and Judet.
* Computed Tomography (CT) Scan: The gold standard for detailed fracture assessment. Thin-cut axial images with multiplanar reconstructions (coronal and sagittal) provide invaluable information regarding fragment displacement, articular step-off, comminution, and intra-articular fragments. 3D reconstructions are particularly useful for visualizing the overall fracture pattern, assessing reduction maneuvers, and planning plate placement. A CT angiogram may be considered if there is suspicion of vascular injury or to identify an aberrant obturator artery (corona mortis).
Based on the imaging, the fracture pattern is precisely classified, and the involvement of the anterior column, anterior wall, quadrilateral surface, and pubic ramus is assessed. The likely displacement vectors are determined, guiding the choice of reduction tools and fixation strategies.
Preoperative Templating and Implant Selection
- Templating: Preoperative templating with radiographic overlays or digital software helps in selecting appropriate plate length and contours. The pelvic brim (iliopubic) plate is a common choice for anterior column fixation. Specific plates (e.g., reconstruction plates, anatomical precontoured plates) are chosen based on the fracture morphology and the surgeon's preference.
- Screw Selection: Various screw types (cortical, cancellous, lag screws) and lengths are pre-selected. Consideration is given to screw trajectories to achieve bicortical purchase and avoid intra-articular penetration or neurovascular injury.
- Reduction Instruments: A range of reduction clamps (e.g., Farabeuf, Matta, pointed reduction clamps), large fragment forceps, Hohmann retractors, and bone hooks should be readily available.
Patient Preparation
- Medical Optimization: Patients are thoroughly assessed for medical comorbidities. Preoperative optimization of cardiac, pulmonary, and nutritional status is crucial.
- Antibiotic Prophylaxis: Intravenous broad-spectrum antibiotics are administered within one hour of incision.
- Deep Vein Thrombosis (DVT) Prophylaxis: Mechanical (compression stockings, pneumatic compression devices) and chemical prophylaxis (low-molecular-weight heparin) are initiated based on institutional protocols and patient risk factors.
- Bowel Preparation: Some surgeons advocate for a mild bowel preparation to decompress the small bowel and facilitate exposure, although this is not universally practiced.
- Blood Management: Type and cross-match for several units of packed red blood cells should be performed, as significant blood loss can occur. Cell saver technology is frequently employed.
Patient Positioning
The patient is positioned supine on a radiolucent operating table.
* Lower Extremity Access: The entire affected lower extremity should be prepped and draped free to allow for traction, rotation, and flexion/extension maneuvers during reduction. A bump under the ipsilateral hip may facilitate internal rotation of the leg and optimize exposure of the iliac wing.
* Fluoroscopy Access: The table must allow for easy C-arm access for intraoperative fluoroscopic imaging in AP and Judet views to confirm reduction and implant placement.
* Instrumentation and Draping: The abdomen and entire affected hemipelvis are prepped and draped in a sterile fashion. The ipsilateral hip is left exposed for manipulation. The contralateral leg is often slightly abducted and flexed to allow for C-arm positioning.
* Foley Catheter: A urinary catheter is inserted to decompress the bladder, which is critical for reducing its profile in the medial window and protecting it from injury.
* Preoperative Marking: Key anatomical landmarks (ASIS, pubic tubercle, iliac crest, inguinal ligament) are marked on the skin.
Detailed Surgical Approach and Technique
The ilioinguinal approach is a technically demanding procedure requiring a systematic, layer-by-layer dissection and a precise understanding of the pelvic anatomy.
Incision
The incision roughly follows the lines of cleavage, typically a long oblique incision beginning 2-3 cm posterior to the ASIS, extending along the inguinal crease towards the pubic symphysis. The original description by Letournel involves a curved incision.

This incision ensures adequate exposure of the entire anterior column, from the iliac wing to the pubic symphysis. The length of the incision is tailored to the extent of the fracture and the patient's body habitus, typically ranging from 15-25 cm.
Initial Dissection and Exposure
- Skin and Subcutaneous Tissue: The incision is carried down through the skin and subcutaneous fat. The superficial epigastric and superficial circumflex iliac vessels are encountered and should be ligated or cauterized.

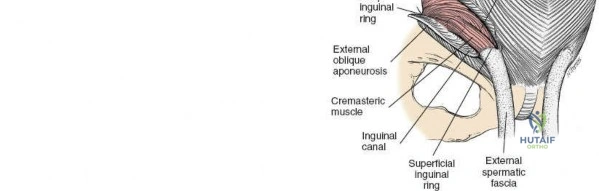
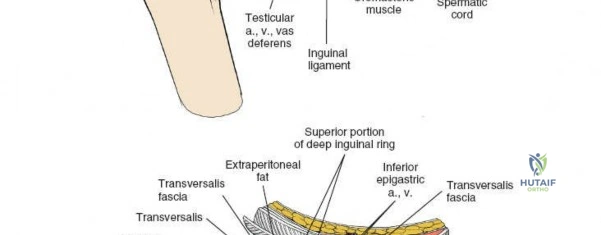
- External Oblique Aponeurosis: The external oblique aponeurosis is identified. The superficial inguinal ring is often visualized as a defect in this aponeurosis just superior to the pubic tubercle.

The ilioinguinal nerve is typically found coursing within the inguinal canal, superficial to the spermatic cord (male) or round ligament (female), and deep to the external oblique aponeurosis. It should be carefully identified and protected.
The external oblique aponeurosis is incised longitudinally, approximately 1-2 cm superior to and parallel to the inguinal ligament, from the ASIS to the pubic tubercle. This incision opens the inguinal canal.
Management of the Inguinal Canal Contents
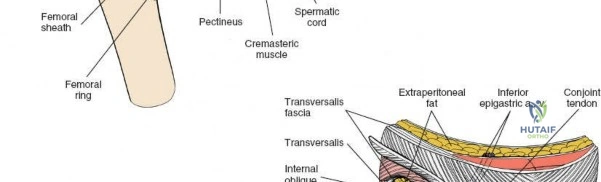
- Spermatic Cord/Round Ligament: In males, the spermatic cord, containing the vas deferens, testicular artery, and pampiniform plexus, is carefully identified. In females, the round ligament is identified. These structures are gently dissected free from their attachments and encircled with a Penrose drain or vessel loop. They are then retracted inferiorly and medially towards the pubic tubercle.


This maneuver allows access to the posterior wall of the inguinal canal (transversalis fascia) and the underlying preperitoneal space. - Ilioinguinal Nerve: The ilioinguinal nerve typically accompanies the spermatic cord/round ligament. It should be isolated and protected, usually retracted with the cord.
Development of the Three Surgical Windows
The key to the ilioinguinal approach is the development of the three anatomical windows by dividing the transversalis fascia and mobilizing the neurovascular structures.
-
Accessing the Lateral Window (Iliac Fossa):
- The transversalis fascia is incised longitudinally from the ASIS towards the lateral aspect of the deep inguinal ring.
- The peritoneum and its contents are carefully swept medially and superiorly, exposing the iliacus muscle.
- The lateral femoral cutaneous nerve (LFCN) is identified as it crosses the iliacus muscle, typically 2-3 cm medial to the ASIS. It is usually found lying on the iliacus fascia and should be protected. If it is tethered, neurolysis may be performed to minimize traction injury.
- The iliacus muscle is then elevated subperiosteally from the inner table of the ilium using an electrocautery and periosteal elevators. This exposes the entire iliac fossa, from the ASIS posteriorly towards the sacroiliac joint, and inferiorly to the anterior column.
A curved Hohmann retractor can be placed around the iliac wing to retract the iliacus and the LFCN, providing wide access to the iliac crest and inner wall of the ilium. This window is primarily for the reduction and fixation of the iliac wing component of anterior column fractures.
-
Accessing the Middle Window (Vascular Window):
- The femoral nerve and vessels are identified exiting beneath the inguinal ligament. The femoral nerve is the most lateral of the three main structures, followed by the artery, and then the vein (NAVY: Nerve, Artery, Vein, Y-fronts for lateral to medial).
- The femoral nerve is carefully dissected free and retracted laterally using a small Hohmann retractor or vessel loop.
- The femoral artery and vein, encased in the femoral sheath, are dissected free and retracted medially. This creates a narrow space, the middle window.

Through this window, the psoas muscle and pectineus muscle can be identified. Subperiosteal dissection of the pectineus from the superior pubic ramus exposes the bone. The quadrangular surface and the superior aspect of the obturator foramen can be visualized. This window is critical for manipulating fragments of the superior pubic ramus and for placing fixation along the iliopectineal line.
-
Accessing the Medial Window (Pubic Window):
- The femoral artery and vein are further retracted laterally. The spermatic cord/round ligament and ilioinguinal nerve are retracted superiorly and laterally.
- The transversalis fascia is further incised towards the pubic symphysis, entering the preperitoneal space (space of Retzius).
- The bladder, usually identified by the presence of the Foley catheter, is gently swept medially.

This provides access to the anterior aspect of the pubic body, the pubic symphysis, and the inferior pubic ramus. The obturator nerve and vessels exit through the obturator foramen posteriorly and must be protected. The "corona mortis," if present, requires meticulous identification and ligation if necessary.
This window is essential for reducing and fixing fractures involving the pubic symphysis and the lower part of the anterior column.
Fracture Reduction and Fixation
- Debridement: Hematoma, loose bone fragments, and soft tissue debris are removed from the fracture site.
-
Reduction Maneuvers:
- Traction: Longitudinal traction on the limb, often combined with internal or external rotation, can help disimpact fragments.
- Direct Manipulation: Large fracture fragments are manipulated using pointed reduction clamps, bone hooks, or reduction forceps. These instruments can be applied to the iliac wing, pubic ramus, or the quadrilateral surface.
- Joy-sticking: Schanz pins or Kirschner wires can be inserted into large fragments to serve as joy-sticks for manipulation.
- Indirect Reduction: Techniques such as external rotation of the limb can help reduce certain anterior column fragments by leveraging muscle attachments.
- Visualization: Fluoroscopy is used intermittently to assess reduction in AP and Judet views. Direct visualization through the windows confirms anatomical reduction of the articular surface and fracture lines.

Reduction is often performed sequentially, starting with the most displaced or largest fragment, and then addressing smaller fragments. For anterior column fractures, the iliac wing component is often reduced first, followed by the pubic ramus component, aiming to restore the iliopectineal line.
-
Internal Fixation:
- Plate Placement: Precontoured plates (e.g., pelvic brim plates, reconstruction plates) are typically used. A plate is usually contoured to lie along the pelvic brim (iliopectineal line), spanning from the anterior iliac crest across the anterior column to the pubic symphysis or pubic tubercle.

The plate is secured with screws, ensuring bicortical purchase where possible and avoiding penetration into the joint or critical neurovascular structures. Screw length and trajectory are critical. Fluoroscopic guidance is essential for confirming screw placement.

Additional fixation, such as independent lag screws or small fragment plates, may be used for specific fragments, particularly those involving the quadrilateral surface or the pubic symphysis.

The plate must be carefully positioned to avoid tension on the femoral nerve or vessels. The middle window is particularly important for passing the plate from the lateral to the medial window while protecting the neurovascular bundle.

The plate is typically secured first to the intact bone fragments at either end and then progressively compressed across the fracture lines.

Careful attention to the quadrilateral surface is needed as screws placed too long can perforate into the hip joint.

- Plate Placement: Precontoured plates (e.g., pelvic brim plates, reconstruction plates) are typically used. A plate is usually contoured to lie along the pelvic brim (iliopectineal line), spanning from the anterior iliac crest across the anterior column to the pubic symphysis or pubic tubercle.
Closure
- Hemostasis: Meticulous hemostasis is achieved.
- Peritoneal Closure: The incised transversalis fascia and peritoneum are carefully reapproximated to prevent future hernia formation.
- Spermatic Cord/Round Ligament Repositioning: The spermatic cord or round ligament is returned to its anatomical position.
- External Oblique Aponeurosis Closure: The external oblique aponeurosis is closed over the inguinal canal, reconstructing the anterior wall of the inguinal canal.
- Muscle and Fascia Closure: The origins of the external oblique, internal oblique, and tensor fasciae latae are reattached to the iliac crest if elevated.
- Subcutaneous Tissue and Skin: The subcutaneous tissue is closed in layers, followed by skin closure with staples or sutures. A suction drain may be placed in the deep space to manage potential hematoma, particularly if extensive dissection was performed or significant bleeding was encountered.
Complications and Management
The ilioinguinal approach, while effective, is associated with a range of potential complications given the complex anatomy of the inguinal region. Meticulous surgical technique, thorough anatomical knowledge, and careful postoperative management are crucial for minimizing these risks.
| Complication | Incidence (Approximate) | Salvage/Management Strategies |
| Nerve Injuries | LFCN: 5-15% (neuropraxia, paresthesia); Femoral Nerve: <1% (motor weakness, sensory deficit); Ilioinguinal/Genitofemoral: <5% (sensory deficit). | Prevention: Meticulous dissection, careful retraction (avoid prolonged, direct pressure on nerves), early identification. LFCN: Often resolves spontaneously. Gabapentin/pregabalin for persistent pain. Local anesthetic injections. Rarely, surgical neurolysis or neurectomy for intractable cases. Femoral Nerve: Urgent consultation with neurology and vascular surgery. Neurolysis if entrapped. Physiotherapy. Prognosis variable. Ilioinguinal/Genitofemoral: Conservative management for sensory changes. Gabapentin. Surgical exploration/neurectomy if severe pain persists. |
| Vascular Injuries | Femoral Artery/Vein: <1% (hematoma, pseudoaneurysm, thrombosis); External Iliac vessels: Rare but catastrophic; Corona Mortis: Up to 30% variants, ~2% significant bleeding if not identified. | Prevention: Preoperative CT angiogram for high-risk cases. Careful identification and protection of vessels. Intraoperative: Immediate direct pressure, vascular clamp, vascular repair (primary repair or graft) by vascular surgeon. Postoperative: Close monitoring for signs of hematoma or limb ischemia. Anticoagulation for thrombosis. |
| Infection | Superficial: 2-5%; Deep: <1%. | Prevention: Strict aseptic technique, prophylactic antibiotics, proper wound care. Superficial: Oral antibiotics, wound care. Deep: Surgical debridement, intravenous antibiotics, implant retention vs. removal depending on stability and pathogen. |
| Heterotopic Ossification (HO) | Varies widely, 10-50% radiographic HO, 5-15% symptomatic HO (requiring excision). | Prevention: Postoperative NSAIDs (e.g., indomethacin) for 3-6 weeks, or radiation therapy (single dose 700-800 cGy within 72 hours pre- or post-op) for high-risk patients (e.g., severe head injury, ankylosing spondylitis, previous HO). Management: Surgical excision of mature HO after bone scan confirms maturity and patient symptoms warrant intervention. |
| Nonunion/Malunion | Rare (1-5%) with anatomical reduction and stable fixation. Higher in complex patterns, comminution, or infection. | Nonunion: Revision surgery with debridement, bone grafting, and rigid fixation. Malunion: Corrective osteotomy for symptomatic malunion if function significantly impaired. Often managed conservatively if asymptomatic. |
| Post-traumatic Arthritis | 10-30%, even with good reduction. Directly related to quality of reduction, residual articular incongruity, and extent of initial chondral damage. | Prevention: Anatomical reduction, stable fixation, early mobilization. Management: Non-operative (NSAIDs, physiotherapy, injections) for mild symptoms. Total hip arthroplasty (THA) for severe, debilitating arthritis. |
| Inguinal Hernia | <1-5%. Related to inadequate closure of the transversalis fascia or external oblique aponeurosis. | Prevention: Meticulous layered closure of the posterior and anterior walls of the inguinal canal. Management: Surgical repair (herniorrhaphy) once fracture healing is stable, often with mesh. |
| Ileus/Bowel Injury | Ileus: 5-10% (transient). Bowel injury: Rare (<0.1%). | Ileus: NPO, nasogastric tube decompression, prokinetic agents. Bowel Injury: Immediate surgical repair by general surgeon, often requiring colostomy if contamination is severe. |
| Blood Loss/Transfusion | Significant blood loss is common; transfusion rates 20-50%. | Prevention: Meticulous hemostasis, cell saver. Management: Blood product transfusion, close hemodynamic monitoring, correction of coagulopathy. |
| DVT/Pulmonary Embolism (PE) | DVT: 5-15% (clinical); PE: <1-2% (clinical). | Prevention: Early mobilization, mechanical and chemical prophylaxis. Management: Anticoagulation (therapeutic dose), IVC filter in selected cases for PE. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is crucial for achieving optimal functional outcomes following acetabular fracture fixation via the ilioinguinal approach. The protocol is typically individualized based on fracture stability, quality of fixation, patient comorbidities, and surgeon preference. The general principles involve protecting the fixation, preventing complications, and progressively restoring range of motion, strength, and weight-bearing capacity.
Phase 1: Immediate Postoperative (Weeks 0-6)
Goals: Protect fixation, manage pain and swelling, prevent DVT and HO, initiate gentle range of motion.
- Weight Bearing: Strict non-weight bearing (NWB) or touch-down weight bearing (TDWB) on the operative extremity. This is paramount to prevent stress on the healing fracture and fixation construct.
- Mobility:
- Bed rest with assistive devices (e.g., abduction pillow) to maintain neutral hip alignment.
- Log-roll transfers.
- Initiate gentle ankle pumps and quadriceps/gluteal isometric exercises.
- Passive or active-assisted range of motion (ROM) of the hip, avoiding extremes of motion (e.g., no hip flexion beyond 90 degrees, no adduction past midline, no extreme internal/external rotation) which could stress the repair.
- Out-of-bed transfers to a chair with NWB status using a walker or crutches.
- Pain Management: Multimodal approach including opioids, NSAIDs (if not contraindicated for HO prophylaxis), acetaminophen, and nerve blocks.
- DVT Prophylaxis: Continue mechanical and chemical prophylaxis.
- HO Prophylaxis: Continue NSAID regimen or radiation therapy as indicated.
- Wound Care: Monitor incision for signs of infection. Drain care if present.
- Education: Educate patient on weight-bearing restrictions, transfer techniques, and signs of complications.
Phase 2: Early Recovery (Weeks 6-12)
Goals: Gradual increase in weight bearing, progressive ROM and strengthening, improved gait mechanics.
- Weight Bearing: Progress from TDWB to partial weight bearing (PWB) as tolerated, typically 25-50% body weight, with assistive devices (walker/crutches). Progression is often guided by radiographic evidence of early fracture healing (callus formation) and clinical stability.
- Mobility:
- Continue active/passive ROM exercises for the hip, gradually increasing arc of motion.
- Initiate gentle hip strengthening exercises (e.g., straight leg raises in supine, gentle hip abduction/adduction against gravity, mini-squats with support).
- Core strengthening exercises.
- Scar massage once incision is well healed.
- Gait Training: Focus on proper gait mechanics with PWB, gradually reducing reliance on assistive devices.
- Pain Management: Wean off opioids as pain subsides.
- Monitoring: Regular radiographic follow-up to assess fracture healing and implant integrity.
Phase 3: Advanced Recovery (Weeks 12-24)
Goals: Full weight bearing, restore full pain-free ROM and strength, improve endurance, prepare for return to functional activities.
- Weight Bearing: Progress to full weight bearing (FWB) as tolerated, typically by 12-16 weeks, without assistive devices, once radiographic evidence of solid union is confirmed.
- Mobility:
- Aggressive hip strengthening, focusing on all muscle groups (abductors, adductors, flexors, extensors).
- Proprioceptive and balance training.
- Functional exercises (e.g., step-ups, lunges, cycling).
- Stretching to improve flexibility and address any residual stiffness.
- Cardiovascular Fitness: Encourage low-impact aerobic activities.
- Sport-Specific Training: For athletes, gradual progression to sport-specific drills and activities.
Phase 4: Return to Activity (Months 6+)
Goals: Return to pre-injury activity levels, optimize long-term function.
- Activity Progression: Gradual return to higher impact activities and sports, guided by pain, strength, and functional assessment.
- Maintenance: Continue a home exercise program for strength and flexibility.
- Long-term Monitoring: Educate patients about the risk of post-traumatic arthritis and the importance of continued follow-up.
Throughout all phases, patient compliance, pain management, and vigilant monitoring for complications (e.g., nerve irritation, implant loosening, HO, infection) are paramount. A multidisciplinary approach involving orthopaedic surgeons, physical therapists, and pain management specialists is often most effective.
Summary of Key Literature and Guidelines
The foundational understanding and widespread adoption of the ilioinguinal approach for acetabular fractures are largely attributed to the seminal work of Judet and Letournel. Their comprehensive classification system and detailed surgical approaches, particularly the description of the ilioinguinal corridor, transformed the management of these complex injuries from a largely non-operative realm to a reconstructive surgical discipline.
Classic Literature
- Judet and Letournel's Work: The publication of "Fractures of the Acetabulum" in 1993, a culmination of decades of research, remains the definitive text. It meticulously details the fracture patterns, surgical anatomy, and technical aspects of the various approaches, including the ilioinguinal. Their work established the principles of anatomical reduction, stable internal fixation, and early mobilization as cornerstones of successful treatment. They rigorously demonstrated the clinical superiority of operative management for displaced articular fractures.
Evolution of Surgical Techniques
While the fundamental principles outlined by Letournel remain, advancements in imaging, instrumentation, and implant design have refined the ilioinguinal approach:
* Advanced Imaging: The advent of routine CT scanning with 3D reconstructions has significantly improved preoperative planning, allowing surgeons to precisely delineate fracture patterns, assess articular congruity, and identify critical anatomical variations (e.g., corona mortis) with greater accuracy than plain radiographs alone.
* Precontoured Plates: The development of anatomically precontoured plates has simplified plate application and improved fixation stability, particularly along the pelvic brim and for fragments of the quadrilateral surface. These plates often reduce the need for extensive intraoperative contouring, potentially shortening operative time and reducing soft tissue irritation.
* Minimally Invasive Approaches: While the ilioinguinal remains an open approach, there is ongoing research into percutaneous or limited open techniques, often guided by fluoroscopy or navigation systems, to reduce soft tissue dissection and potentially lower complication rates, though these are typically reserved for less complex patterns or specific fracture elements.
* Navigation and Robotics: The integration of computer-assisted navigation and robotics is emerging in complex pelvic surgery, offering enhanced precision for screw placement and reduction verification, potentially reducing neurovascular risks and improving reduction accuracy, though widespread adoption for acetabular fractures via the ilioinguinal approach is still developing.
Outcomes and Evidence
Numerous studies have consistently demonstrated that anatomical reduction (defined as <1-2 mm articular step-off or gap) and stable fixation of acetabular fractures are the most critical prognostic factors for favorable long-term outcomes, particularly in preventing post-traumatic osteoarthritis.
* Reduction Quality: Studies by Matta, Tile, and others have shown a direct correlation between the quality of reduction and the incidence of post-traumatic arthritis. Excellent or good reductions are associated with significantly lower rates of arthritis and better functional scores compared to imperfect or poor reductions.
* Timing of Surgery: Early surgical intervention (typically within 5-10 days of injury) is generally advocated, as delayed surgery can increase the difficulty of reduction due to hematoma organization and early callus formation, potentially leading to poorer outcomes. However, patient stability often dictates the timing.
* Functional Outcomes: With anatomical reduction, good to excellent functional outcomes are reported in 70-85% of patients. Factors influencing poorer outcomes include advanced age, severe initial cartilage damage, associated injuries, and complications such as infection or heterotopic ossification.
Current Guidelines
Current guidelines for acetabular fracture management emphasize:
* Comprehensive Preoperative Assessment: Including meticulous imaging and medical optimization.
* Adherence to Surgical Principles: Anatomical reduction, stable internal fixation, and protection of neurovascular structures.
* Appropriate Approach Selection: Tailoring the surgical approach to the specific fracture pattern. The ilioinguinal approach remains the gold standard for most anterior column and anterior wall fractures.
* Proactive Management of Complications: Including DVT and HO prophylaxis.
* Structured Rehabilitation: A progressive, supervised rehabilitation program is essential for restoring function.
In conclusion, the ilioinguinal approach remains a cornerstone for the surgical treatment of complex anterior acetabular fractures. Its effective application relies on a profound understanding of the regional anatomy, meticulous surgical technique, and comprehensive postoperative care. Continued adherence to established principles, coupled with the integration of technological advancements, ensures the best possible outcomes for patients facing these challenging injuries.
Clinical & Radiographic Imaging