Anterior Tarsal Tunnel Syndrome: Operative Guide
Key Takeaway
Anterior tarsal tunnel syndrome involves the entrapment of the deep peroneal nerve beneath the inferior extensor retinaculum. Common in athletes, it presents with dysesthesias in the first web space and potential motor deficits in the extensor digitorum brevis. This guide covers the biomechanics, clinical evaluation, and step-by-step surgical decompression techniques required to relieve nerve compression and restore optimal foot and ankle function.
INTRODUCTION TO ANTERIOR TARSAL TUNNEL SYNDROME
Anterior tarsal tunnel syndrome is a highly specific, often underdiagnosed compressive neuropathy denoting the entrapment of the deep peroneal nerve (DPN) as it courses beneath the inferior extensor retinaculum of the foot and ankle. While posterior tarsal tunnel syndrome involving the tibial nerve is more widely recognized, anterior tarsal tunnel syndrome presents a unique set of biomechanical and diagnostic challenges for the orthopedic surgeon.
The condition is characterized by a constellation of symptoms, most notably dysesthesias in the first web space, radiating pain into the anterior compartment of the leg, and potential motor deficits affecting the extensor digitorum brevis (EDB) muscle. Successful management requires a profound understanding of the local pathoanatomy, precise clinical and electrodiagnostic evaluation, and meticulous surgical technique when conservative measures fail.
ANATOMY AND BIOMECHANICS
To fully grasp the pathophysiology of anterior tarsal tunnel syndrome, a rigorous understanding of the deep peroneal nerve's anatomical course is mandatory.
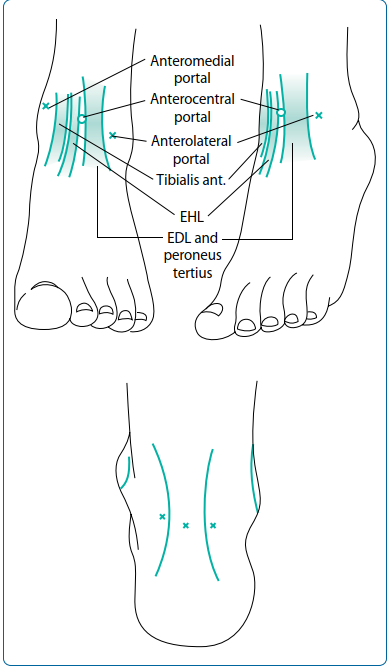
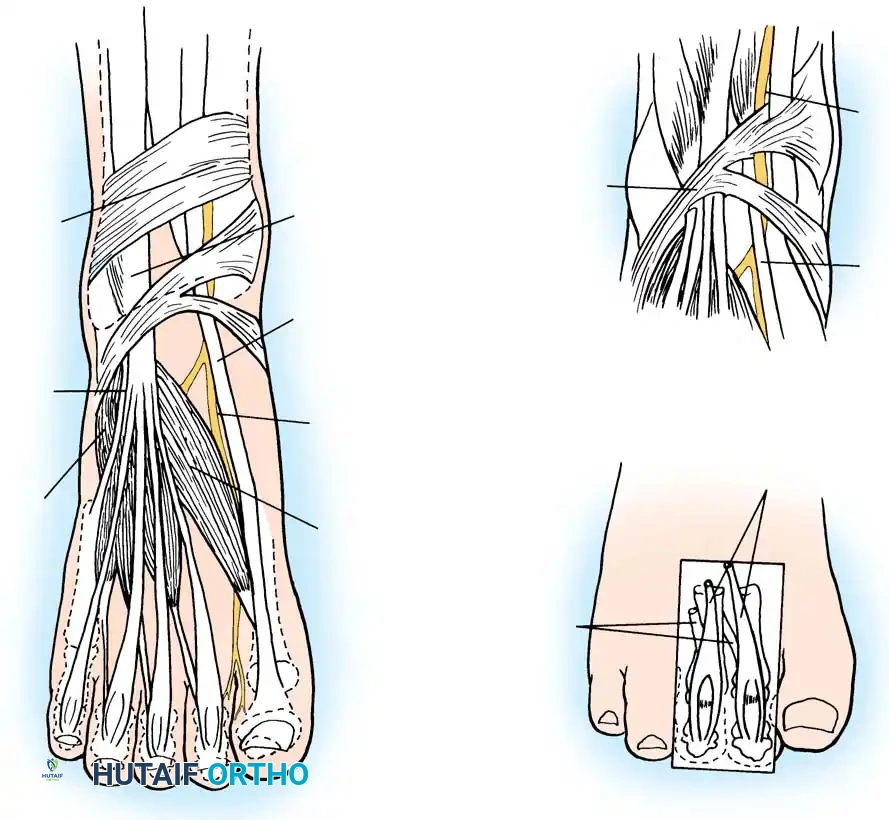
The deep peroneal nerve originates as a bifurcation of the common peroneal nerve at the level of the fibular neck. It descends through the anterior compartment of the leg, supplying the tibialis anterior, extensor digitorum longus (EDL), extensor hallucis longus (EHL), and peroneus tertius. As it approaches the ankle joint, the nerve travels between the EHL and EDL tendons, accompanied by the anterior tibial artery.
At the level of the ankle, the nerve passes beneath the superior extensor retinaculum and then enters the true "anterior tarsal tunnel" beneath the inferior extensor retinaculum.
Just distal to the ankle joint, the deep peroneal nerve bifurcates into two terminal branches:
1. The Lateral Terminal Branch (Motor): Courses laterally beneath the EDB muscle, providing its primary motor innervation. Entrapment of this specific branch leads to isolated EDB atrophy and weakness.
2. The Medial Terminal Branch (Sensory): Continues distally alongside the dorsalis pedis artery to provide pure sensory innervation to the first web space and the apposing sides of the first and second toes.
Clinical Pearl: The deep peroneal nerve is highly susceptible to compression due to its superficial location over the bony prominences of the midfoot and its rigid confinement beneath the cruciform fibers of the inferior extensor retinaculum.
ETIOLOGY AND PATHOGENESIS
Mann and Baxter extensively described the etiology of this syndrome, noting that it most commonly occurs in athletes (particularly runners) or in patients with degenerative structural changes in the foot. The entrapment is typically mechanical, resulting from either extrinsic compression or intrinsic space-occupying lesions.
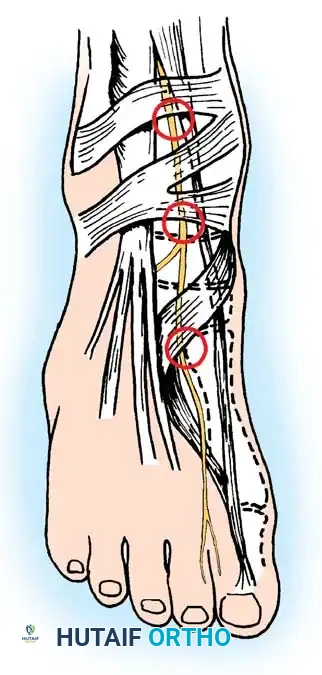
Common Zones of Impingement
The most common areas of nerve entrapment, as noted by Mann and Baxter, occur at distinct anatomical bottlenecks:
1. Beneath the inferior extensor retinaculum.
2. Over the talonavicular joint, particularly in the presence of dorsal osteophytes.
3. At the metatarsocuneiform articulation.
Causative Factors
- Dorsal Osteophytes: Degenerative joint disease at the ankle, midtarsal, or metatarsocuneiform joints can produce dorsal osteophytes that act as a hard anvil against which the nerve is compressed by the overlying retinaculum or footwear.
- Extrinsic Compression: Tight-fitting shoes, rigid ski boots, or even a key tied into the lacing of a running shoe can precipitate acute or chronic compression.
- Repetitive Microtrauma: Hooking the feet under a bar or bench when performing sit-ups places direct, repetitive pressure over the anterior tarsal tunnel.
- Space-Occupying Lesions: Ganglion cysts (with or without the presence of traumatic osteophytes), lipomas, or peripheral nerve sheath tumors (schwannomas) can drastically reduce the volume of the tunnel, leading to severe entrapment.
CLINICAL EVALUATION AND DIAGNOSIS
Patient History and Physical Examination
Patients typically present with an insidious onset of aching pain over the dorsum of the midfoot, accompanied by sharp, burning dysesthesias radiating into the first web space.
Key physical findings include:
* Sensory Deficits: Decreased light touch and pinprick sensation strictly localized to the first web space and the apposing sides of the adjacent toes.
* Tinel's Sign: A positive percussion test (Tinel sign) over the deep peroneal nerve beneath the inferior extensor retinaculum or over a palpable dorsal osteophyte.
* Motor Deficits: Possible atrophy and weakness of the extensor digitorum brevis muscle. This is often visible as a concavity on the lateral dorsum of the foot compared to the contralateral side.
* Proximal Radiation: Patients may experience proximally radiating dysesthesias into the anterior compartment of the leg (Valleix phenomenon).
Diagnostic Imaging
- Weight-Bearing Radiographs: Essential for identifying dorsal osteophytes at the talonavicular or tarsometatarsal joints, which are frequent culprits of mechanical tethering.
- Magnetic Resonance Imaging (MRI): Highly recommended if a space-occupying lesion (such as a ganglion cyst or nerve sheath tumor) is suspected. MRI will clearly delineate the size, extent, and origin of the mass relative to the neurovascular bundle.
Electrodiagnostic Studies (EMG/NCS)
Electrical studies are the gold standard for confirming the diagnosis and ruling out proximal lesions (e.g., L5 radiculopathy or common peroneal nerve entrapment at the fibular head).
Pathognomonic findings include:
* Electromyography (EMG): Fibrillations, positive sharp waves, and reduced motor action potentials in the extensor digitorum brevis.
* Nerve Conduction Studies (NCS): Increased distal motor and sensory latencies across the ankle, in the presence of a normal nerve conduction velocity in the deep peroneal nerve from the fibular neck to the ankle.
Surgical Warning: Entrapment can occasionally occur distal to the motor branch to the EDB. In these cases, the patient will present with pure sensory symptoms in the first web space, and EMG of the EDB will be entirely normal. Do not let a normal EDB EMG rule out a distal sensory branch entrapment.
NONOPERATIVE MANAGEMENT
Conservative treatment should be exhausted before considering surgical intervention, particularly in cases driven by extrinsic compression or transient inflammation.
* Footwear Modification: Eliminating tight-fitting shoes, avoiding rigid boots, and utilizing alternative lacing techniques to bypass the dorsal midfoot.
* Immobilization: A short period of immobilization in a walking boot can reduce acute perineural inflammation.
* Corticosteroid Injections: A carefully targeted, ultrasound-guided steroid injection beneath the inferior extensor retinaculum can be both diagnostic and therapeutic. Care must be taken to avoid intratendinous or intraneural injection.
SURGICAL MANAGEMENT: OPERATIVE TECHNIQUE
Operative decompression and neurolysis of the deep peroneal nerve distal to the ankle joint are highly successful when conservative measures (steroid injection, immobilization, or both) fail, or when a clear space-occupying lesion is identified.
Preoperative Preparation and Positioning
- The patient is placed in the supine position on the operating table.
- A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the delicate branches of the deep peroneal nerve and the adjacent dorsalis pedis artery.
- Intravenous antibiotics are administered prior to tourniquet inflation.
Incision and Superficial Dissection
- A longitudinal incision is made over the dorsum of the foot, centered over the area of maximal tenderness or the palpable Tinel's sign. The incision typically runs parallel and just lateral to the extensor hallucis longus (EHL) tendon.
- Careful superficial dissection is performed to avoid injury to the crossing branches of the superficial peroneal nerve, which lie in the subcutaneous tissue.
(Note: Preoperative planning and incision marking are critical. The fullness or mass, if present, should be outlined by dots to guide the surgical approach, ensuring adequate exposure for both nerve release and mass excision.)
Deep Dissection and Retinaculum Release
- The inferior extensor retinaculum is identified. It is a distinct, cruciform fascial structure binding the extensor tendons.
- The retinaculum is carefully incised longitudinally over the neurovascular bundle.
- The deep peroneal nerve is identified lying between the EHL tendon medially and the EDL tendons laterally. It is intimately associated with the dorsalis pedis artery.
- Trace the Nerve: Trace each nerve branch well distal to the inferior edge of the retinaculum until it is absolutely certain that no tethering exists.
Management of Space-Occupying Lesions and Osteophytes
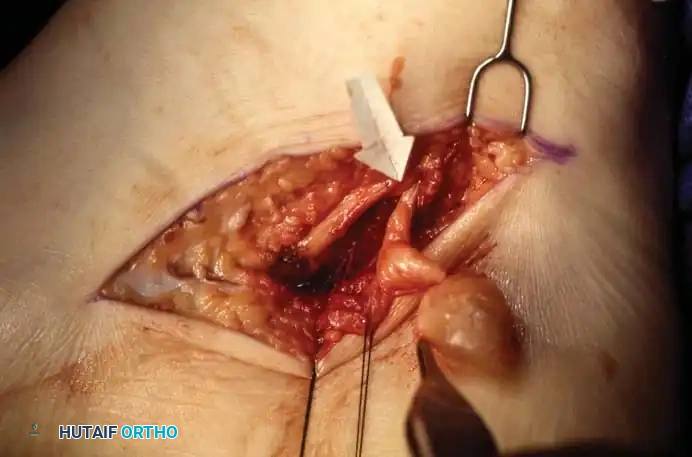
If the entrapment is secondary to a ganglion cyst or a peripheral nerve sheath tumor, meticulous microsurgical technique is required.

(Intraoperative view demonstrating a space-occupying lesion compressing the adjacent nerve structures. Careful isolation of the nerve from the mass is paramount.)
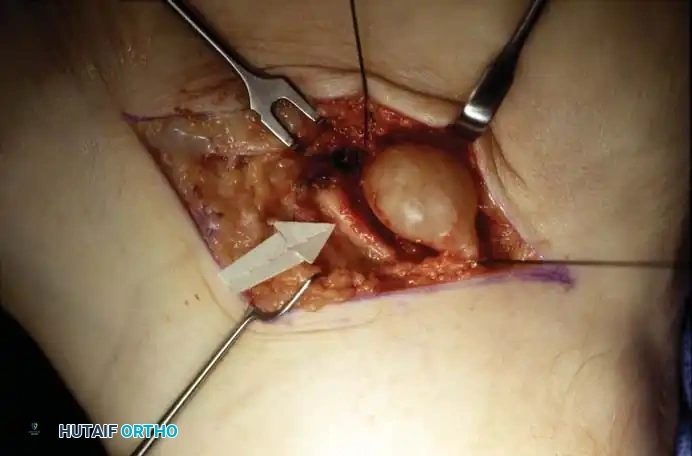
(Further dissection reveals the extent of the tumor/ganglion. The mass must be completely excised while preserving the integrity of the nerve fascicles.)
- Osteophyte Excision: If a dorsal osteophyte at the talonavicular or metatarsocuneiform joint is the source of compression, the nerve and artery must be gently retracted. The osteophyte is then resected flush with the normal cortical bone using a rongeur or a high-speed burr. Bone wax may be applied to minimize postoperative bleeding.
- Epineurotomy: Inspect the nerve carefully under loupe magnification. If the epineurium appears unequally thickened, fibrotic, or severely constricted, a longitudinal epineurotomy should be performed using a micro-blade to decompress the individual fascicles.
Surgical Principles for Variant Tarsal Entrapments
While the focus here is the anterior tarsal tunnel, the surgical principles of nerve decompression apply equally to posterior tarsal tunnel variants. For instance, space-occupying lesions (like schwannomas or ganglions) can entrap the tibial nerve branches.
If a tumor involves the medial calcaneal branch or the lateral plantar nerve deep to the abductor hallucis, the surgeon must trace the nerve well distal to the inferior edge of the flexor retinaculum. This is made easier by releasing part of the fascial origin of the abductor hallucis. The tumor is often resectable while leaving most of the nerve branch intact, utilizing the same microsurgical epineural dissection techniques described for the deep peroneal nerve.
Closure
- Remove a small section of the extensor retinaculum over the neurovascular bundle to prevent postoperative tethering and recurrence of the syndrome.
- Deflate the Tourniquet: Remove the tourniquet and secure meticulous hemostasis before closing the wound. The dorsalis pedis artery and its venae comitantes can bleed significantly, leading to a postoperative hematoma that could re-compress the nerve.
- Close the wound in layers (subcutaneous tissue and skin only). Do not repair the retinaculum over the nerve.
- Apply a sterile, bulky compression dressing.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Optimal postoperative care is designed to prevent perineural adhesions while allowing the surgical incision to heal without tension.
- Immediate Postoperative Phase (Days 0-14): The patient is placed in a bulky compression dressing and a short leg plaster splint or a removable walking boot. The foot is maintained in a neutral position to avoid excessive stretch on the healing nerve and soft tissues.
- Weight-Bearing: The patient begins weight-bearing to tolerance in the protective boot.
- Suture Removal: The sutures are removed at approximately 10 to 14 days postoperatively. Adhesive strips may be applied if necessary.
- Mobilization: Immobilization is discontinued at 2 weeks unless localized tenderness or swelling persists. Active and passive range of motion exercises for the toes and ankle are initiated to promote nerve gliding and prevent scar tissue tethering.
- Return to Activity: If the patient is an athlete, progressive training and sport-specific drills can typically resume approximately 4 to 6 weeks after surgery, provided the incision is fully healed and the patient is asymptomatic during impact activities.
COMPLICATIONS AND PITFALLS
While surgical decompression of the anterior tarsal tunnel is generally highly successful, surgeons must be vigilant regarding potential complications:
1. Incomplete Release: Failure to trace the nerve far enough distally, or failure to recognize and resect an underlying dorsal osteophyte, is the most common cause of persistent postoperative symptoms.
2. Vascular Injury: The dorsalis pedis artery is highly vulnerable during the deep dissection. Injury can result in pseudoaneurysm formation or severe hematoma.
3. Superficial Peroneal Nerve Neuroma: Careless superficial dissection can transect branches of the superficial peroneal nerve, leading to painful neuroma formation that often eclipses the original deep peroneal nerve symptoms.
4. Complex Regional Pain Syndrome (CRPS): As with any peripheral nerve surgery in the foot and ankle, there is a risk of CRPS. Early mobilization, aggressive pain management, and vitamin C supplementation may help mitigate this risk.
By adhering to strict anatomical principles, utilizing appropriate diagnostic modalities, and executing precise microsurgical techniques, the orthopedic surgeon can reliably relieve deep peroneal nerve entrapment and restore excellent function to the patient's foot and ankle.
You Might Also Like