Decoding Acetabulum Fractures & Dislocations: Key Insights
Key Takeaway
Learn more about Decoding Acetabulum Fractures & Dislocations: Key Insights and how to manage it. Acetabulum fractures and dislocations are high-energy trauma injuries, frequently resulting from motor vehicle accidents or falls, with an incidence of 3 per 100,000 annually. These injuries often involve the acetabulum's two-columned structure (anterior and posterior) and can cause sciatic nerve damage in up to 30% of cases. Fracture patterns vary based on impact force and hip position at the time of injury.
Introduction and Epidemiology
Acetabular fractures represent a complex and highly demanding subset of orthopedic traumatology, requiring a profound understanding of pelvic osteology, precise radiographic interpretation, and advanced surgical techniques. The incidence of acetabular fractures is approximately 3 per 100,000 population per year. Historically, these injuries have followed a distinct bimodal distribution. In the younger demographic, they are predominantly the result of high-energy trauma secondary to motor vehicle collisions, motorcycle accidents, or falls from significant heights. Conversely, an increasingly prominent second peak is observed in the geriatric population, where low-energy mechanisms, such as a ground-level fall, impact osteoporotic bone, often resulting in complex fracture patterns involving the anterior column and quadrilateral plate.
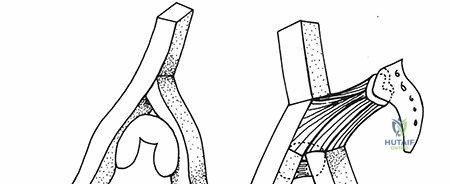
The mechanism of injury dictates the resultant fracture pattern, which is fundamentally dependent on the position of the femoral head at the exact moment of impact, the magnitude of the applied vector force, and the intrinsic bone quality of the patient. Direct impact to the greater trochanter with the hip in a neutral position classically produces a transverse type of acetabular fracture. Variations in hip abduction alter this trajectory; an abducted hip causes a low transverse fracture, whereas an adducted hip causes a high transverse fracture. An externally rotated and abducted hip transmits force anteriorly, causing an anterior column injury. An internally rotated hip directs the force posteriorly, resulting in a posterior column or posterior wall injury. With indirect trauma, such as a classic "dashboard" injury to the flexed knee, the degree of hip flexion is the critical variable. As the degree of hip flexion increases, the posterior wall is fractured in an increasingly inferior position. Similarly, as the degree of hip flexion decreases, the superior portion of the posterior wall is more likely to be involved.
Given the high-energy nature of these injuries in younger cohorts, initial clinical evaluation must rigorously adhere to Advanced Trauma Life Support protocols. Trauma evaluation is usually necessary, with strict attention to airway, breathing, circulation, disability, and exposure. Associated injuries are exceedingly common, including closed head injuries, blunt thoracic or abdominal trauma, and concomitant musculoskeletal injuries such as pelvic ring disruptions or long bone fractures.
Neurologic injuries occur in up to 30% of cases at the time of presentation. These are usually partial injuries to the sciatic nerve, with the peroneal division more commonly injured than the tibial division due to its lateral and relatively tethered anatomical course at the fibular neck and sciatic notch. Careful assessment of neurovascular status is mandatory upon initial presentation and following any closed reduction maneuvers. Patient factors such as chronological and physiological age, degree of systemic trauma, presence of associated injuries, and general medical condition are paramount, as they directly dictate damage-control orthopedics versus early total care, ultimately affecting treatment decisions and long-term prognosis.
Surgical Anatomy and Biomechanics
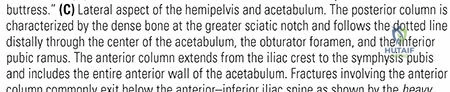
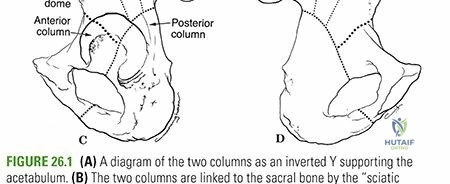
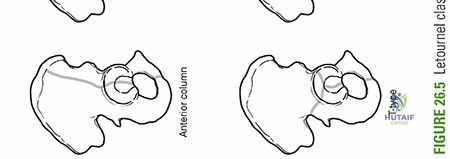
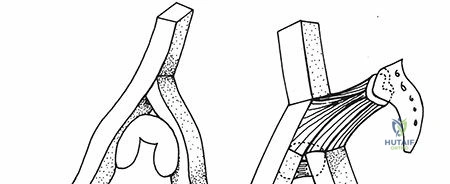
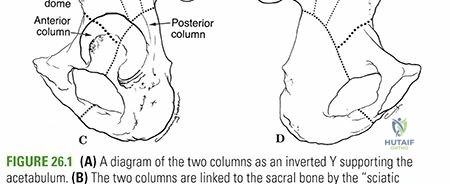
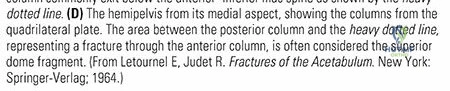
A mastery of acetabular anatomy is the foundation of successful surgical intervention. From the lateral aspect of the pelvis, the innominate osseous structural support of the acetabulum may be conceptualized as a two-columned construct, originally described by Judet and Letournel, forming an inverted Y. This architectural model divides the hemipelvis into an anterior and posterior column, meeting at the thickest portion of the ilium, the sciatic buttress, to form the weight-bearing dome.
Anterior Column Iliopubic Component
The anterior column extends from the anterior iliac crest down to the symphysis pubis. It encompasses the anterior half of the iliac wing, the pelvic brim, the anterior wall of the acetabulum, and the superior pubic ramus. Mechanically, it supports the anterior aspect of the femoral head and is frequently involved in fractures seen in the elderly population.
Posterior Column Ilioischial Component
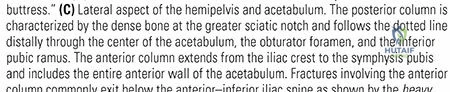
The posterior column is a massive, dense strut of bone that extends from the superior gluteal notch to the ischial tuberosity. It includes the dense bone of the greater and lesser sciatic notches, the posterior wall of the acetabulum, and the ischial tuberosity. The posterior column provides the primary buttress against posterior subluxation of the femoral head, making its anatomical restoration critical for hip stability.
Acetabular Dome and Quadrilateral Plate
The acetabular dome is the superior, critically important weight-bearing portion of the acetabulum at the junction of the anterior and posterior columns, including osseous contributions from each. Medial to the acetabulum lies the quadrilateral plate, a thin, flat surface of bone forming the medial wall of the acetabulum. Medial displacement of the quadrilateral plate allows for central subluxation of the femoral head, a common and challenging deformity to correct.
Critical Neurovascular Structures
Surgical approaches to the acetabulum place several vital structures at risk, necessitating meticulous dissection and anatomical familiarity.
The Corona Mortis represents a critical vascular communication between the external iliac or deep inferior epigastric vessels and the obturator vessels. It may be visualized within the Stoppa approach or the second window of the ilioinguinal approach. It is present in up to 10% to 15% of patients and typically extends over the superior pubic ramus. The average distance from the symphysis pubis to the corona mortis is approximately 6 cm. Iatrogenic injury to this anastomosis can result in massive, life-threatening hemorrhage that retracts into the true pelvis.
The ascending branch of the medial femoral circumflex artery is the main blood supply to the femoral head. It courses deep to the quadratus femoris muscle. During posterior approaches, the quadratus femoris must be preserved, or only partially released at its most proximal aspect, to avoid devascularizing the femoral head and inducing iatrogenic avascular necrosis.
The superior gluteal neurovascular bundle emerges from the greater sciatic notch, superior to the piriformis muscle. It supplies the gluteus medius, gluteus minimus, and tensor fasciae latae. Excessive retraction during posterior approaches or dissection extending too far into the sciatic notch can cause profound abductor weakness and a subsequent Trendelenburg gait.
Indications and Contraindications
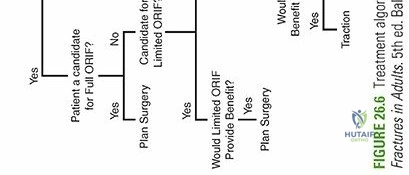
The decision to proceed with operative versus non-operative management of an acetabular fracture requires a synthesis of radiographic parameters, patient physiology, and functional demands. The primary goal of surgery is to achieve an anatomical reduction of the articular surface and stable internal fixation to allow for early mobilization and prevent post-traumatic osteoarthritis.
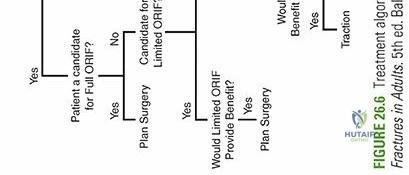
Operative and Non Operative Decision Making
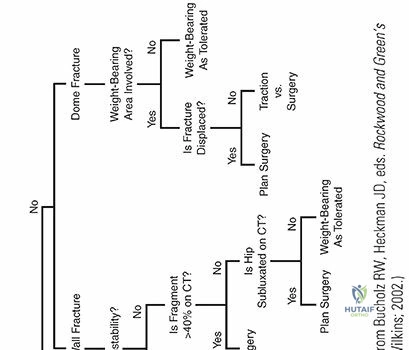
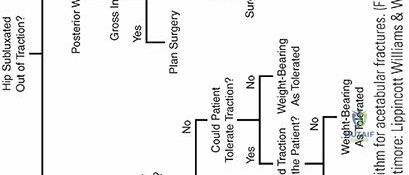
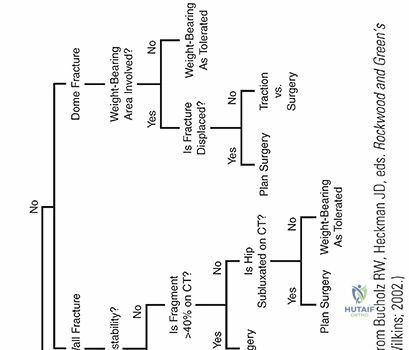
Non-operative management is generally reserved for fractures that do not disrupt the weight-bearing dome and maintain hip joint stability and congruency. Displacement of less than 2 mm within the articular surface is often tolerated. Additionally, the concept of secondary congruence, often seen in both-column fractures where the articular fragments displace uniformly around an intact femoral head, may permit non-operative treatment, provided the femoral head remains perfectly spherical and centered beneath the acetabular roof. Roof arc angles, measured on AP and Judet views, help quantify the involvement of the weight-bearing dome; angles greater than 45 degrees in all three planes historically suggested non-operative potential, though modern CT analysis has largely superseded this metric.
Operative indications are definitive for fractures exhibiting greater than 2 mm of displacement in the weight-bearing dome, posterior wall fractures involving greater than 20% to 25% of the articular surface (or those demonstrating clinical or radiographic instability), intra-articular incarcerated loose bodies, irreducible fracture-dislocations, and progressive sciatic nerve deficits following closed reduction.
| Parameter | Operative Management | Non Operative Management |
|---|---|---|
| Articular Displacement | > 2 mm in the weight-bearing dome | < 2 mm or extra-articular |
| Hip Stability | Unstable (e.g., large posterior wall) | Stable examination under fluoroscopy |
| Joint Congruence | Incongruent or subluxated | Congruent or secondary congruence |
| Intra articular Debris | Present (bone or cartilage fragments) | Absent |
| Neurologic Status | Progressive sciatic nerve deficit | Intact or stable deficit |
| Patient Physiology | Medically optimized for major surgery | Severe comorbidities or non-ambulatory |
| Soft Tissue Envelope | Intact, amenable to surgical incision | Severe local infection or Morel-Lavallée |

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the most critical phase of acetabular fracture management. The surgeon must construct a three-dimensional mental model of the fracture to select the appropriate surgical approach, anticipate reduction vectors, and plan implant placement.
Radiographic Evaluation
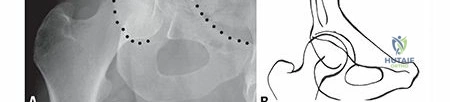
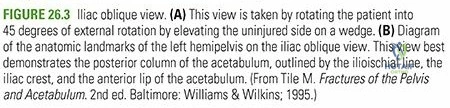
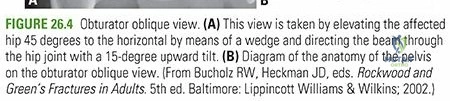
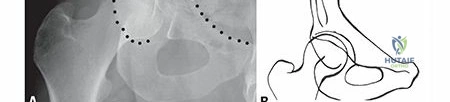
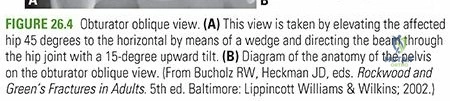
The standard radiographic series includes an Anteroposterior pelvis and the two Judet oblique views (Obturator Oblique and Iliac Oblique), taken at 45-degree angles.
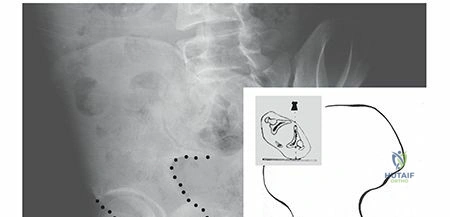
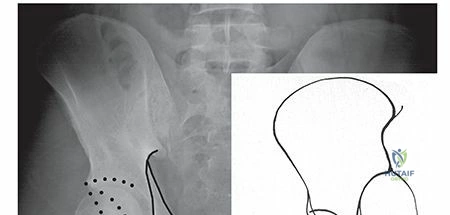
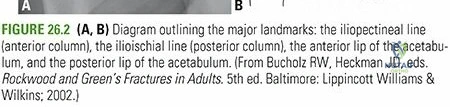
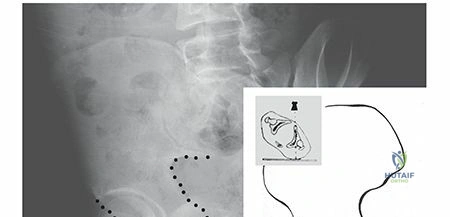
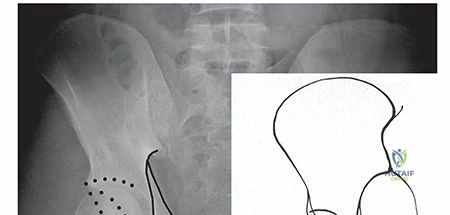
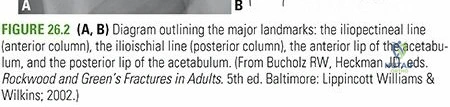
- The AP view allows evaluation of the six fundamental radiographic lines of Letournel: the iliopectineal line (anterior column), the ilioischial line (posterior column), the radiographic teardrop (inferior medial wall), the acetabular roof, the anterior wall, and the posterior wall.
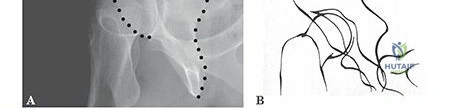
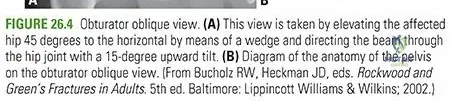
- The Obturator Oblique view highlights the anterior column and the posterior wall.
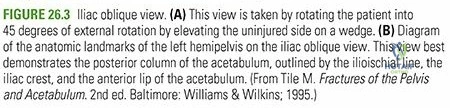
- The Iliac Oblique view profiles the posterior column and the anterior wall.
High-resolution computed tomography with 2D multiplanar reformats and 3D surface rendering is the gold standard. It delineates marginal impaction, intra-articular loose bodies, quadrilateral plate comminution, and precise fracture line trajectories that plain radiographs often obscure.
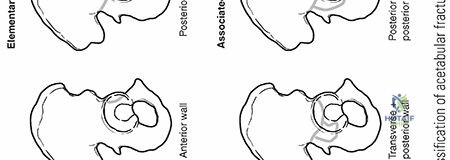
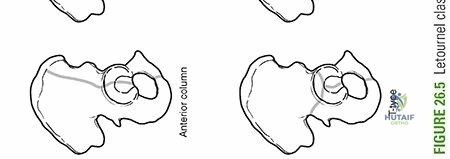
Letournel Classification System
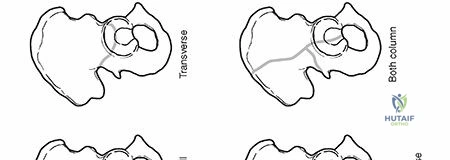
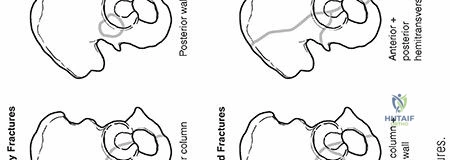
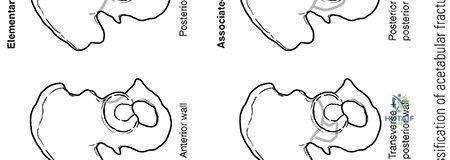
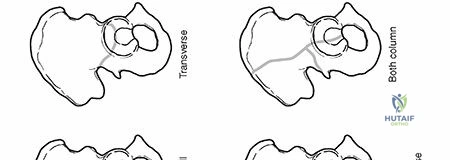
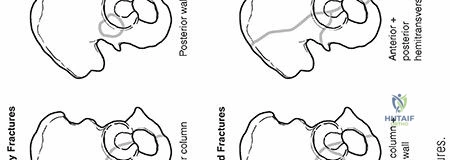
Using the imaging data, the fracture is categorized according to the Judet and Letournel classification into five elementary patterns (Anterior Wall, Anterior Column, Posterior Wall, Posterior Column, Transverse) and five associated patterns (Posterior Column and Posterior Wall, Transverse and Posterior Wall, T-type, Anterior Column/Anterior Hemidecalogue and Posterior Hemitransverse, Both-Column). This classification directly dictates the surgical approach.
Patient Positioning Considerations
Positioning is dictated by the chosen surgical approach.
- Prone Positioning: Utilized for the Kocher-Langenbeck approach. The knee must be flexed to at least 90 degrees to relax the sciatic nerve, and the hip is extended. A radiolucent table is mandatory.
- Supine Positioning: Utilized for the Ilioinguinal or modified Stoppa approaches. A bump is placed under the ipsilateral sacrum, and the entire hemipelvis must be accessible to fluoroscopy.
- Floppy Lateral Positioning: Allows access to both anterior and posterior approaches sequentially without re-draping, highly useful for complex T-type or both-column fractures requiring a combined approach.
Skeletal traction via a distal femoral pin is frequently employed intraoperatively to distract the femoral head, facilitating disimpaction of articular fragments and clearance of the joint space.
Detailed Surgical Approach and Technique
The execution of acetabular surgery requires meticulous soft tissue handling, strategic exploitation of internervous and intermuscular planes, and mastery of specialized reduction tooling.
The Kocher Langenbeck Approach
The Kocher-Langenbeck approach is the workhorse for posterior pathology, including posterior wall, posterior column, and certain transverse and T-type fractures.
The incision begins near the posterior superior iliac spine, extends to the greater trochanter, and continues distally along the femoral shaft. The superficial dissection splits the gluteus maximus bluntly in line with its fibers. The fascial incision distally splits the iliotibial band.
Deep dissection requires immediate identification and protection of the sciatic nerve. The nerve is often found deep to the piriformis and superficial to the obturator internus and gemelli. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) are tagged and tenotomized near their femoral insertion and reflected medially over the sciatic nerve to act as a protective cushion. Crucially, the quadratus femoris must be preserved to protect the ascending branch of the medial femoral circumflex artery.
Following capsulotomy, the hip joint is distracted. Marginal impaction of the articular surface is elevated, and the subchondral defect is grafted with cancellous autograft or allograft. The posterior wall is then reduced and provisionally held with Kirschner wires. Definitive fixation is achieved using a pre-contoured 3.5 mm reconstruction plate spanning from the ischium to the intact ilium, supplemented by spring plates for comminuted marginal fragments and lag screws directed outside the joint capsule.
The Ilioinguinal Approach
Developed by Letournel, the ilioinguinal approach provides extensive access to the anterior column, anterior wall, and the internal aspect of the innominate bone from the SI joint to the pubic symphysis.
The incision spans from the posterior aspect of the anterior two-thirds of the iliac crest, curving anteriorly to the pubic symphysis. The approach is defined by three distinct surgical windows created by mobilizing the neurovascular structures:
1. First Window (Lateral): Lateral to the iliopsoas muscle and femoral nerve. It provides access to the internal iliac fossa and the sacroiliac joint.
2. Second Window (Middle): Between the iliopsoas/femoral nerve laterally and the external iliac vessels medially. This exposes the pelvic brim, quadrilateral plate, and superior pubic ramus.
3. Third Window (Medial): Medial to the external iliac vessels and lateral to the spermatic cord or round ligament. It provides access to the superior pubic ramus and the pubic symphysis.
Reduction of the anterior column often involves the use of specialized pelvic reduction forceps, such as the Jungbluth or Weber clamps, applied to strategically placed cortical screws. Fixation typically involves a long reconstruction plate placed along the pelvic brim.
The Modified Stoppa Approach
The modified Stoppa approach is an intrapelvic, sub-rectus approach that has gained immense popularity for treating fractures with significant medial displacement of the quadrilateral plate.
A Pfannenstiel incision is typically utilized. The rectus abdominis is split along the linea alba, and dissection proceeds bluntly into the retropubic space of Retzius. The surgeon works along the deep aspect of the true pelvis. The corona mortis must be identified and ligated early in the dissection. This approach allows for direct buttressing of the quadrilateral plate using infrapectineal plating techniques, effectively resisting the medial subluxation forces of the femoral head.
Complications and Management
Acetabular fractures are fraught with potential complications, stemming both from the initial traumatic insult and the complex surgical interventions required for reconstruction.
Post Traumatic Osteoarthritis
Post-traumatic osteoarthritis is the most common long-term complication, occurring in up to 20% to 30% of patients despite anatomical reduction. The incidence is heavily correlated with the initial energy of the injury, the presence of marginal impaction, damage to the femoral head cartilage, and the quality of the surgical reduction. A reduction with a residual step-off greater than 1 mm significantly increases the risk of rapid joint degeneration.
Avascular Necrosis
Avascular necrosis of the femoral head occurs in approximately 2% to 10% of cases. It is most frequently associated with posterior fracture-dislocations where the hip remains dislocated for a prolonged period, leading to mechanical kinking or tearing of the medial femoral circumflex artery. Iatrogenic AVN can occur if the quadratus femoris or the piriformis fossa vascular anastomoses are aggressively disrupted during posterior surgical approaches.
Neurologic Injury
Sciatic nerve palsy is a devastating complication. While traumatic palsies are present in up to 30% of cases preoperatively, iatrogenic palsies occur in 2% to 6% of surgically treated patients. Iatrogenic injury is usually secondary to excessive retractor pressure during the Kocher-Langenbeck approach. Continuous intraoperative somatosensory evoked potential and spontaneous electromyography monitoring, combined with maintaining the knee in flexion and the hip in extension, are critical preventative strategies.
Heterotopic Ossification
Heterotopic ossification is primarily a complication of the Kocher-Langenbeck and extensile approaches, where extensive stripping of the gluteal musculature provokes ectopic bone formation. Severe HO can lead to profound mechanical block to hip motion. Prophylaxis is highly recommended and typically consists of either a single fraction of low-dose radiation (700-800 cGy) administered within 72 hours postoperatively or a 6-week course of oral indomethacin.
Complications Summary Table
| Complication | Estimated Incidence | Etiology and Risk Factors | Prevention and Management Strategies |
|---|---|---|---|
| Post Traumatic Osteoarthritis | 20% - 30% | Cartilage necrosis, imperfect reduction, high-energy impact | Anatomical reduction (<1mm step-off), early mobilization, definitive THA if severe |
| Avascular Necrosis | 2% - 10% | Prolonged dislocation, vascular injury (MFCA) | Urgent closed reduction in ER, preserve quadratus femoris intraoperatively |
| Sciatic Nerve Palsy | Traumatic: 30% Iatrogenic: 2%-6% |
Posterior dislocation, retractor neuropraxia | Knee flexion/hip extension during surgery, careful retractor placement, intraoperative neuromonitoring |
| Heterotopic Ossification | 15% - 40% (without prophylaxis) | Extensive muscle stripping, posterior approaches | Indomethacin (75mg SR/day) or single-dose radiation therapy, meticulous hemostasis |
| Venous Thromboembolism | 4% - 10% | Pelvic venous stasis, endothelial injury, hypercoagulability | Mechanical prophylaxis, LMWH or direct oral anticoagulants for 4-6 weeks post-op |
| Infection | 1% - 5% | Prolonged operative time, Morel-Lavallée lesions | Preoperative optimization, aggressive debridement of degloving injuries, targeted antibiotics |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is a delicate balance between protecting the internal fixation and promoting early joint mobility to nourish the articular cartilage and prevent stiffness.
Immediately postoperatively, patients are placed on strict deep vein thrombosis prophylaxis, typically utilizing low-molecular-weight heparin or targeted direct oral anticoagulants, continued for a minimum of four to six weeks. Heterotopic ossification prophylaxis is initiated within the first 24 to 48 hours.
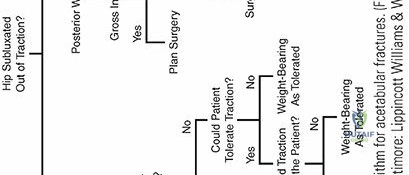
Weight-bearing is strictly limited to protect the articular reduction. Patients are generally restricted to toe-touch weight-bearing or non-weight-bearing on the operative extremity for 8 to 12 weeks, depending on the fracture pattern, bone quality, and the rigidity of the fixation achieved.
Despite weight-bearing restrictions, early range of motion is paramount. Continuous passive motion machines or active-assisted physical therapy should begin on postoperative day one. Early mobilization prevents capsular contracture, aids in the clearance of intra-articular hematoma, and provides the mechanical stimulation necessary for fibrocartilage healing of small chondral defects. Isometric strengthening of the quadriceps, hamstrings, and gluteal muscles is initiated early, progressing to dynamic resistance training only after radiographic evidence of fracture consolidation is confirmed, typically around the 12-week mark.
Summary of Key Literature and Guidelines
The
Clinical & Radiographic Imaging