ABOS Part I & OITE Orthopedic Review: AC Joint & Sarcoma MCQs | Part 22152

Key Takeaway
This module offers a comprehensive review for ABOS Part I and AAOS OITE exams. It features 20 advanced MCQs on high-yield orthopedic topics, including acromioclavicular joint separations (Rockwood classification, surgical management) and dedifferentiated liposarcoma (diagnosis, staging, treatment, surgical margins). This content is designed to enhance knowledge for orthopedic board exam preparation.
ABOS Part I & OITE Orthopedic Review: AC Joint & Sarcoma MCQs | Part 22152
A 25-year-old male presents to the emergency department after a direct fall onto the superior aspect of his right shoulder during a rugby match. He reports immediate severe pain and inability to lift his arm. On examination, there is marked superior displacement of the distal clavicle, significant tenting of the skin, and a palpable gap between the clavicle and acromion. The deltoid and trapezius muscles appear extensively stripped from the distal clavicle. A clinical image is shown below.
Based on the clinical presentation and the provided image, which Rockwood classification best describes this injury?

Correct Answer: E
The patient's presentation, including a direct fall, marked superior displacement of the distal clavicle, significant skin tenting, and extensive stripping of the deltoid and trapezius muscles, is characteristic of a Rockwood Type V AC joint separation. The clinical image further supports the severe superior displacement and soft tissue disruption.
- Type I: Involves a sprain of the AC ligaments without significant disruption or instability.
- Type II: Characterized by a complete tear of the AC ligaments, but intact coracoclavicular (CC) ligaments, leading to partial superior subluxation (typically less than 25% of clavicular height).
- Type III: Involves complete tears of both AC and CC ligaments, with the clavicle displaced superiorly by 25% to 100% of its height, but generally remaining within the sagittal contour of the acromion. Deltoid and trapezius attachments may be intact or minimally disrupted.
- Type IV: Distinguished by complete tears of AC and CC ligaments with posterior displacement of the clavicle into or through the trapezius muscle.
- Type V: Represents a severe injury with complete tears of AC and CC ligaments, marked superior displacement of the clavicle (typically >100% of its height), and extensive stripping of the deltoid and trapezius from the distal clavicle. This matches the clinical vignette and image.
A 30-year-old construction worker sustains a Rockwood Type III AC joint separation. Understanding the biomechanics of the AC joint is crucial for treatment planning. Which of the following statements accurately describes the primary role of the coracoclavicular (CC) ligaments in AC joint stability?
Correct Answer: B
The coracoclavicular (CC) ligaments (conoid and trapezoid) are the primary vertical stabilizers of the AC joint. They provide approximately 70-80% of the vertical stability, resisting superior translation of the clavicle relative to the acromion. Their disruption, as seen in Type III and higher injuries, leads to significant vertical instability.
- Option A: The AC ligaments (superior, inferior, anterior, posterior) primarily resist anterior and posterior shear forces and contribute to horizontal stability.
- Option C: The AC ligaments contribute the majority of horizontal stability, while the CC ligaments primarily provide vertical stability.
- Option D: The conoid ligament primarily resists superior translation and posterior rotation, while the trapezoid ligament primarily resists superior translation and posterior displacement, and limits horizontal movement. Their roles are more complex than simply anterior/posterior displacement resistance.
- Option E: The coracoacromial ligament forms part of the coracoacromial arch, which prevents superior humeral head migration, but the CC ligaments are distinct and primarily stabilize the AC joint itself.
A 40-year-old male presents with a painful right shoulder after falling directly onto his acromion. Radiographs reveal complete tears of both the acromioclavicular (AC) and coracoclavicular (CC) ligaments. The distal clavicle is superiorly displaced by approximately 75% of its height relative to the acromion, but an axillary lateral view confirms it remains within the sagittal contour of the acromion. The deltoid and trapezius muscle attachments appear largely intact. Which Rockwood classification best describes this injury?
Correct Answer: B
The description of complete tears of both AC and CC ligaments, with the clavicle superiorly displaced by 25% to 100% of its height and remaining within the sagittal contour of the acromion, is the classic definition of a Rockwood Type III AC joint separation. The largely intact deltoid and trapezius attachments further support this classification.
- Type II: Involves a complete tear of the AC ligaments but intact CC ligaments, with partial superior subluxation (less than 25% displacement).
- Type IV: Characterized by complete tears of AC and CC ligaments, but with posterior displacement of the clavicle into or through the trapezius muscle, which is not described here.
- Type V: Involves complete tears of AC and CC ligaments with marked superior displacement (>100% of clavicular height) and extensive stripping of the deltoid and trapezius muscles, which is more severe than described.
- Type VI: A rare injury involving inferior dislocation of the clavicle beneath the coracoid process or acromion.
A 32-year-old professional overhead baseball pitcher sustains a Rockwood Type III AC joint separation in his dominant throwing arm. He is highly motivated to return to elite-level competition as quickly and safely as possible. Given the controversy surrounding Type III management, what is the most appropriate initial treatment recommendation for this patient, according to the provided case material?
Correct Answer: B
The case material explicitly states that for Rockwood Type III injuries, operative indications include 'Acute injuries in young, high-demand individuals (e.g., overhead athletes, manual laborers) where functional demands are high and an earlier return to full activity is desired.' A professional overhead baseball pitcher with a dominant arm injury perfectly fits this description, making immediate surgical reconstruction the most appropriate initial recommendation.
- Option A: While non-operative management is an option for Type III injuries, it is generally reserved for sedentary individuals, those with low functional demands, or elderly patients with comorbidities. It is less suitable for a high-demand athlete aiming for a quick return to sport.
- Option C: A trial of non-operative management is a valid approach for some Type III patients, but for a professional athlete, delaying surgical intervention could prolong recovery and potentially compromise their career. The case suggests immediate surgery for this specific profile.
- Option D: Distal clavicle excision (Mumford procedure) is typically performed for symptomatic AC joint arthrosis, often a long-term complication, or sometimes concurrently with reconstruction in chronic cases, not as an initial treatment for an acute Type III separation.
- Option E: While a hook plate is a surgical option, modern literature (as summarized in the case) favors suture-button systems due to lower hardware-related complications and the need for a second surgery for removal of hook plates. More importantly, the question asks for the most appropriate *initial treatment recommendation*, which is surgery, not a specific hardware choice.
During an open reduction and internal fixation of a Rockwood Type V AC joint separation, the surgeon is carefully dissecting to expose the coracoid process for coracoclavicular ligament reconstruction. The anatomical illustration below highlights the relevant structures.
Which critical neurovascular structure is at the highest risk of iatrogenic injury if dissection is not meticulously performed, particularly when drilling tunnels through the base of the coracoid?

Correct Answer: C
The case explicitly states that 'The brachial plexus and subclavian vessels lie inferior and medial to the coracoid process. Extreme caution is required during surgical dissection and drilling around the coracoid to avoid iatrogenic injury.' These structures are immediately adjacent to the coracoid base, making them highly vulnerable during tunnel drilling or aggressive dissection.
- Option A: The axillary nerve is typically located more inferiorly and posteriorly, wrapping around the surgical neck of the humerus, and is less directly at risk during coracoid exposure for AC joint reconstruction.
- Option B: The suprascapular nerve passes through the suprascapular notch and is at risk during procedures involving the scapular neck or glenoid, but not typically during coracoid exposure.
- Option D: The cephalic vein is located more laterally in the deltopectoral groove and, while needing protection, is generally less critical than the major neurovascular bundle medial to the coracoid.
- Option E: The long thoracic nerve runs along the medial border of the scapula and is at risk during procedures involving the chest wall or scapular dissection, not typically during coracoid exposure.
A surgeon is performing an AC joint reconstruction using a suture-button system for coracoclavicular ligament reconstruction, as shown in the intraoperative image below. After achieving anatomical reduction of the clavicle, the sutures are tensioned and secured. What is the primary biomechanical principle by which this suture-button construct provides vertical stability to the AC joint?

Correct Answer: D
The suture-button system for coracoclavicular (CC) ligament reconstruction works by passing strong suture tapes through tunnels drilled in the clavicle and coracoid. When tensioned, these sutures pull the clavicle inferiorly towards the coracoid process, thereby approximating the two structures and functionally replacing the torn CC ligaments. This restores vertical stability to the AC joint.
- Option A: While AC joint capsular repair may be performed concurrently, the suture-button construct itself is primarily for CC ligament reconstruction and vertical stability, not direct AC ligament repair.
- Option B: Suture-button systems provide dynamic stability, allowing for some micromotion, rather than rigid bony fixation between the clavicle and acromion. Rigid fixation between the clavicle and acromion alone has largely been abandoned due to high failure rates.
- Option C: The goal is to restore the normal anatomical relationship and stability, not to compress the articular surfaces for fusion. Fusion is not a desired outcome for acute AC joint reconstruction.
- Option E: While some historical techniques (e.g., Weaver-Dunn) involved coracoacromial ligament transfer, the suture-button system is a distinct method for CC ligament reconstruction and does not primarily act as a scaffold for other ligament transfers.
A 35-year-old male underwent surgical repair for a Rockwood Type V AC joint separation. A post-operative radiograph is provided below.
Based on the radiograph, which of the following statements best describes the primary fixation method used and its main purpose?
Correct Answer: C
The post-operative radiograph clearly shows a suture-button construct, characterized by small cortical buttons on the superior aspect of the clavicle and inferior aspect of the coracoid, connected by suture material (not directly visible but implied by the buttons). As detailed in the case, suture-button systems are increasingly popular for coracoclavicular (CC) ligament reconstruction, providing dynamic vertical stability by approximating the clavicle to the coracoid.
- Option A: A clavicle hook plate would appear as a plate with a hook extending under the acromion, which is not seen here. While it provides some stability, it's associated with higher irritation rates.
- Option B: K-wires would appear as thin metallic pins crossing the joint, which are absent in this image. K-wires are generally associated with high rates of migration and infection.
- Option D: An AC joint plate would be positioned directly over the AC joint, typically with screws into both the clavicle and acromion, which is not the primary construct shown.
- Option E: Tension band wiring is typically used for fractures, not primary ligamentous reconstruction of the AC joint in this manner.
A 48-year-old male undergoes surgical reconstruction for a Rockwood Type IV AC joint separation using a suture-button system. Six months post-operatively, he presents with persistent pain, instability, and a noticeable superior prominence of the distal clavicle. Radiographs confirm a loss of reduction with significant superior displacement of the clavicle. Which of the following is the most appropriate initial salvage strategy?
Correct Answer: C
The patient presents with a clear loss of reduction and persistent instability after initial surgery. The case material explicitly lists 'Loss of Reduction / Re-dislocation' as a common complication (5-20%) and states the salvage strategy is 'Revision surgery with stronger fixation (e.g., additional suture-buttons, allograft augmentation, AC plate). Address technical errors (e.g., inadequate tensioning, improper tunnel placement, premature mobilization). For chronic cases, more robust reconstruction with graft.'
- Option A: While rehabilitation is crucial, it cannot correct a structural loss of reduction. Aggressive therapy without addressing the underlying instability would likely be ineffective and potentially harmful.
- Option B: Observation and NSAIDs are insufficient for a symptomatic loss of reduction, which indicates mechanical failure of the initial repair.
- Option D: Distal clavicle excision (Mumford procedure) is typically reserved for symptomatic AC joint arthrosis or osteolysis, not for acute or subacute loss of reduction of a Type IV injury, which requires restoration of stability.
- Option E: A corticosteroid injection might temporarily mask pain but does not address the mechanical instability caused by the loss of reduction.
A 29-year-old patient is 4 weeks post-operative from an AC joint reconstruction with a suture-button system. They are currently in Phase I (Protection & Early Motion) of their rehabilitation protocol. Which of the following activities is strictly contraindicated at this stage to protect the healing repair?
Correct Answer: D
Phase I of rehabilitation (4-6 weeks post-op) is focused on protecting the healing repair and maintaining passive range of motion. The guidelines explicitly state to 'avoid cross-body adduction or AC joint compression' and 'No lifting, pushing, pulling, or active shoulder movements against resistance.' Active cross-body adduction directly stresses the AC joint and could jeopardize the repair.
- Option A: Gentle pendulum exercises are initiated around 1-2 weeks post-op and are appropriate for Phase I.
- Option B: Active range of motion exercises for the elbow, wrist, and hand should begin immediately post-op to prevent stiffness.
- Option C: Gentle passive shoulder flexion (0-90 degrees) may be initiated around 2-3 weeks under therapist guidance, making it an appropriate activity for Phase I.
- Option E: Gentle scapular retraction and protraction exercises (non-weight bearing) are encouraged to maintain scapulothoracic mobility.
A 55-year-old sedentary patient, 3 years after non-operative management of a Rockwood Type III AC joint separation, presents with chronic, localized pain and crepitus over the AC joint, particularly with overhead activities and reaching across the body. Physical examination reveals tenderness and pain with cross-body adduction. Radiographs demonstrate significant degenerative changes and osteophytes at the AC joint. What is the most appropriate surgical intervention for this patient's current symptoms?
Correct Answer: C
The patient's presentation of chronic, localized pain, crepitus, and radiographic evidence of degenerative changes (arthrosis/osteophytes) at the AC joint, 3 years after injury, is characteristic of symptomatic AC joint arthrosis. The case material states that 'Distal clavicle excision (Mumford procedure) may also be performed concurrently if significant AC joint arthritis is present' and 'Distal Clavicle Osteolysis... If refractory symptoms, consider Mumford procedure (distal clavicle excision).' For symptomatic AC joint arthrosis, the Mumford procedure is the definitive surgical treatment.
- Option A: Revision CC ligament reconstruction is indicated for chronic instability or loss of reduction, but the primary issue here is symptomatic arthrosis, not necessarily instability requiring reconstruction.
- Option B: Open reduction and internal fixation with a hook plate is for acute AC joint separations or chronic instability, not for degenerative arthritis of the joint itself.
- Option D: Arthroscopic subacromial decompression addresses impingement in the subacromial space, which is distinct from AC joint arthrosis, although they can coexist. The primary pathology described is AC joint degeneration.
- Option E: While physical therapy is always part of conservative management, for chronic, symptomatic degenerative changes refractory to non-operative care, surgical intervention is often required.
A 62-year-old male presents with a slowly enlarging, painless mass in his right posterior thigh, first noticed 18 months prior, with rapid growth in the last 6 months. Physical examination reveals a deep-seated, firm-to-rubbery, 10x8 cm mass with severely limited mobility. Distal neurovascular status is intact. Given these initial findings, which of the following characteristics is the *most* concerning for a soft tissue sarcoma?
Correct Answer: D
The most concerning characteristic for a soft tissue sarcoma in this presentation is the deep subfascial location and recent rapid growth. The case explicitly states, 'The presentation of a deep, painless, enlarging soft tissue mass greater than 5 centimeters in an adult must be considered a soft tissue sarcoma until proven otherwise. The historical details, specifically the deep subfascial location and the recent acceleration in growth, raise immediate suspicion for a malignant process.' Deep location, size greater than 5 cm, and rapid growth are classic 'red flags' for malignancy.
Option A (The patient's age of 62 years): While soft tissue sarcomas are more common in older adults, age alone is not the most concerning feature compared to tumor characteristics. Sarcomas can occur at any age.
Option B (The mass being painless): Painless masses are often dismissed, but many sarcomas are indeed painless, especially in their early stages. Pain is a late symptom, often indicating nerve involvement or rapid expansion, but its absence does not rule out malignancy.
Option C (The insidious onset 18 months prior): The insidious onset is common for many soft tissue masses, both benign and malignant. The *change* in growth pattern (rapid acceleration) is more concerning than the initial slow growth.
Option E (Intact distal neurovascular status): Intact neurovascular status is a reassuring sign regarding limb function but does not diminish the suspicion of malignancy. Sarcomas can grow to a large size by displacing neurovascular structures before causing deficits.
Following initial evaluation, an MRI of the right thigh was performed. The image below shows an axial T1-weighted view of the mass. Based on the provided image and the detailed MRI description in the case, which of the following is the most accurate interpretation of the findings?
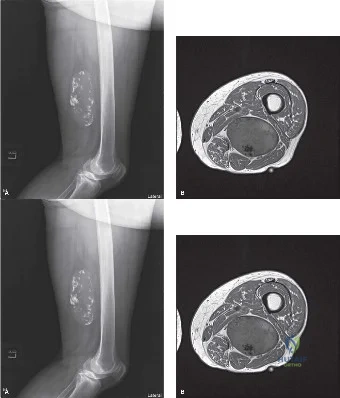
Correct Answer: C
The case explicitly describes the MRI findings: 'The majority of the tumor exhibited high signal intensity on T1-weighted images that suppressed on STIR sequences, confirming the presence of macroscopic adipose tissue. However, unlike a simple benign lipoma, the mass demonstrated significant heterogeneity. There were thickened, irregular internal septations (>2 mm) and distinct nodular areas of non-fatty tissue that were isointense to muscle on T1, hyperintense on T2, and demonstrated avid, heterogeneous enhancement following gadolinium administration.' This biphasic appearance, with both fatty and solid enhancing components, is the classic radiological hallmark of an atypical lipomatous tumor or a dedifferentiated liposarcoma.
Option A (A homogeneous mass with low signal intensity on T1, consistent with a myxoid liposarcoma): Myxoid liposarcomas typically lack macroscopic fat on T1 and show very high signal on T2 due to the myxoid matrix, often appearing cyst-like. This does not match the description of high T1 signal from fat.
Option B (A predominantly fatty mass with thin septations (<2mm) and no enhancing non-fatty components, typical of a simple lipoma): While the mass is predominantly fatty, the description of 'thickened, irregular internal septations (>2 mm) and distinct nodular areas of non-fatty tissue that... demonstrated avid, heterogeneous enhancement' rules out a simple lipoma, which would have thin septations and no significant enhancing non-fatty components.
Option D (A highly heterogeneous mass with significant necrosis and hemorrhage, lacking macroscopic fat, characteristic of a pleomorphic liposarcoma): Pleomorphic liposarcomas are typically high-grade, highly heterogeneous, and often lack visible macroscopic fat on MRI. While the mass is heterogeneous, the presence of significant macroscopic fat on T1 makes pleomorphic liposarcoma less likely as the primary radiological diagnosis.
Option E (A mass with serpiginous vascular channels and phleboliths, suggestive of an intramuscular hemangioma): The MRI description does not mention serpiginous vascular channels or phleboliths (signal voids), which are characteristic of hemangiomas. Plain films also did not identify phleboliths.
Given the high suspicion for a malignant soft tissue sarcoma based on the MRI findings, an image-guided core needle biopsy was planned. Which of the following is the *most* critical aspect of the biopsy strategy for this patient?
Correct Answer: C
The most critical aspect of the biopsy strategy is targeting the solid, enhancing, non-fatty nodular components identified on MRI. The case states: 'Multiple cores were obtained using a 14-gauge coaxial system, specifically targeting the solid, enhancing, non-fatty nodular components identified on the MRI, as these areas harbor the highest grade of malignancy and dictate the overall prognosis and treatment strategy. Biopsying only the fatty components could lead to a false-negative diagnosis of a simple lipoma or under-grading the lesion as merely an atypical lipomatous tumor.'
Option A (Obtaining only fatty tissue samples to confirm the lipomatous nature of the lesion): This is incorrect and dangerous. As explained in the case, biopsying only fatty components risks missing the high-grade dedifferentiated component, leading to under-diagnosis and inappropriate treatment.
Option B (Performing an open incisional biopsy to ensure adequate tissue volume): While incisional biopsies provide more tissue, a well-planned core needle biopsy is generally preferred for extremity sarcomas due to lower morbidity and less risk of tumor seeding, provided it is performed by an experienced musculoskeletal radiologist. The case specifically mentions a percutaneous, ultrasound-guided core needle biopsy.
Option D (Ensuring the biopsy tract is placed perpendicular to the long axis of the limb): The biopsy tract should be placed longitudinally, in line with the planned surgical incision, to ensure it can be completely excised en bloc with the tumor. A perpendicular tract would be difficult to excise completely.
Option E (Avoiding any muscle penetration to minimize post-biopsy hematoma): While minimizing hematoma is important, avoiding *any* muscle penetration is often impossible for deep intramuscular lesions. The key is to ensure the biopsy tract traverses only the muscle immediately adjacent to the tumor and falls entirely within the planned future surgical excision ellipse, even if it means traversing muscle.
Based on the clinical presentation, physical examination, and the MRI findings (including the image provided), which of the following diagnoses is most consistent with Mr. J.A.'s tumor?
Correct Answer: C
The clinical and radiological findings are most consistent with a Dedifferentiated Liposarcoma. The case explicitly states: 'The presence of a predominantly fatty tumor with thick septations and nodular, enhancing, non-lipomatous components is the classic radiological hallmark of an atypical lipomatous tumor or a dedifferentiated liposarcoma.' The table in the case further reinforces this, describing DDLPS as having a 'Biphasic appearance. Fatty regions adjacent to prominent, solid, non-fatty, avidly enhancing nodular components.'
Option A (Simple Lipoma): A simple lipoma would be homogeneously fatty with thin septations (<2mm) and no nodular enhancement. This contradicts the MRI findings of thickened septations and enhancing non-fatty nodules.
Option B (Myxoid Liposarcoma): Myxoid liposarcomas typically lack macroscopic fat on T1 and show very high T2 signal due to the myxoid matrix. The MRI here clearly shows macroscopic fat (high T1 signal).
Option D (Intramuscular Hemangioma): Hemangiomas can be heterogeneous but are characterized by serpiginous vascular channels and often phleboliths (signal voids), which were not described in this case's MRI or plain films.
Option E (Pleomorphic Liposarcoma): Pleomorphic liposarcomas are high-grade and typically lack visible macroscopic fat on MRI, presenting as highly heterogeneous, necrotic, and hemorrhagic masses. While this tumor has high-grade features, the prominent macroscopic fat on T1 makes pleomorphic liposarcoma less likely than dedifferentiated liposarcoma, which specifically arises from a fatty precursor.
The core needle biopsy revealed a biphasic tumor with areas consistent with Well-Differentiated Liposarcoma and an abrupt transition to a high-grade, pleomorphic spindle cell proliferation. To definitively confirm the diagnosis and distinguish it from other high-grade sarcomas, which molecular finding is the diagnostic hallmark for this tumor?
Correct Answer: C
The diagnostic hallmark for the ALT/WDLPS and Dedifferentiated Liposarcoma spectrum is MDM2 and CDK4 gene amplification. The case explicitly states: 'To definitively confirm the diagnosis, molecular profiling utilizing Fluorescence In Situ Hybridization was performed. The tumor cells demonstrated high-level amplification of the MDM2 (Murine Double Minute 2) and CDK4 (Cyclin-Dependent Kinase 4) genes located on chromosome 12q13-15. This molecular signature is the diagnostic hallmark of the ALT/WDLPS and Dedifferentiated Liposarcoma spectrum, distinguishing it definitively from pleomorphic liposarcoma or undifferentiated pleomorphic sarcoma.'
Option A (FUS-DDIT3 translocation (t(12;16))): This translocation is characteristic of Myxoid Liposarcoma.
Option B (EWSR1 rearrangement): This is the defining molecular alteration in Ewing Sarcoma and some other round cell sarcomas.
Option D (INI1 (SMARCB1) deletion): This is characteristic of epithelioid sarcoma and malignant rhabdoid tumors.
Option E (SS18-SSX fusion gene): This fusion gene is the diagnostic hallmark of Synovial Sarcoma.
Based on the final histopathological diagnosis of Dedifferentiated Liposarcoma (FNCLCC Grade 2) and the following staging parameters: Tumor (T): >10 cm, deep to superficial fascia (T3); Node (N): No regional lymph node involvement (N0); Metastasis (M): No distant metastasis (M0). What is the correct AJCC stage for this patient's soft tissue sarcoma?
Correct Answer: E
The patient's AJCC stage is Stage IIIB. According to the AJCC staging system for Soft Tissue Sarcoma of the Trunk and Extremities (which is detailed in the case):
- T3: Tumor greater than 10 cm and deep to the superficial fascia.
- N0: No regional lymph node involvement.
- M0: No distant metastasis.
- G2: FNCLCC Grade 2 (Intermediate-to-High Grade).
Combining these factors:
- T3 (large, deep)
- N0 (no nodal spread)
- M0 (no distant mets)
- G2 (intermediate/high grade)
A T3, N0, M0, Grade 2 tumor corresponds to Stage IIIB. Stage IIIB indicates a large, deep, intermediate-to-high-grade tumor with a significant risk of both local recurrence and distant hematogenous metastasis.
The other options represent lower stages that do not match the combination of a large (T3) and intermediate-to-high grade (G2) tumor.
The multidisciplinary tumor board recommended neoadjuvant external beam radiation therapy followed by wide surgical resection. Which of the following is a primary oncologic advantage of neoadjuvant (preoperative) radiation therapy for this patient's large, deep, high-grade dedifferentiated liposarcoma?
Correct Answer: C
A primary oncologic advantage of neoadjuvant radiation therapy is that it treats a smaller target volume and potentially sterilizes the reactive pseudocapsule, making surgical resection easier. The case states: 'Neoadjuvant radiation therapy (typically 50 Gy in 25 fractions) offers several distinct oncologic advantages: it treats a smaller target volume, potentially sterilizes the reactive pseudocapsule, thickens the tumor pseudocapsule making surgical resection easier, and requires a lower total dose, thereby reducing long-term tissue fibrosis and joint stiffness.'
Option A (Significantly lower risk of acute postoperative wound complications compared to adjuvant radiation): This is incorrect. The case explicitly mentions: 'However, as demonstrated by the landmark O'Sullivan trial, neoadjuvant radiation carries a significantly higher risk of major acute postoperative wound complications (up to 35%) compared to adjuvant radiation.'
Option B (Requires a higher total radiation dose, leading to better tumor kill): This is incorrect. Neoadjuvant radiation typically uses a *lower* total dose (e.g., 50 Gy) compared to adjuvant radiation (e.g., 60-66 Gy) because the tumor is still in situ, allowing for a smaller, more focused field. The goal is to downstage and sterilize, not necessarily to deliver a higher total dose.
Option D (Allows for immediate surgical resection without delay): This is incorrect. Neoadjuvant radiation *delays* surgery by several weeks (typically 5-6 weeks for treatment plus a recovery period), which is a known drawback.
Option E (It is the only effective method to preserve the sciatic nerve in such cases): While neoadjuvant radiation can help with local control and potentially facilitate nerve-sparing surgery, it is not the *only* effective method. Surgical technique (epimesial dissection) is also crucial, and nerve preservation depends on the extent of tumor invasion, not solely on radiation.
During the surgical resection, the tumor pseudocapsule was found to be densely adherent to the epineurium of the sciatic nerve. The orthopedic oncologist performed an epimesial dissection, sharply peeling the epineurium away from the intact sciatic nerve fascicles, leaving the epineurium attached to the tumor specimen. What type of surgical margin does this technique represent at the interface with the sciatic nerve?
Correct Answer: B
An epimesial dissection, where the outermost layer of the nerve sheath (epineurium) is left attached to the tumor specimen, constitutes a Marginal (R1) margin at that specific anatomical location. The case states: 'This constitutes a planned marginal (R1) resection at this specific anatomical location. The rationale is that the combination of this marginal resection and the neoadjuvant radiation therapy provides excellent local control rates while preserving limb function, avoiding the devastating morbidity of a complete sciatic nerve resection.'
- A. Wide (R0) margin: This implies a resection with a cuff of uninvolved healthy tissue (typically >1 cm) around the entire tumor, with no microscopic tumor at the margin. While the overall goal is R0, at the nerve interface, this was not achieved due to adherence.
- C. Intralesional (R2) margin: This means gross tumor was left behind, or the tumor was cut through. This is not the case here, as the nerve fascicles were preserved, and the epineurium was removed with the tumor.
- D. Amputation margin: This refers to the margin of an amputation, which was avoided in this limb-sparing procedure.
- E. Contaminated margin: This term is not a standard oncologic margin classification in the same way as R0, R1, R2. It might refer to a situation where tumor cells are spilled, but the epimesial dissection is a controlled, planned technique.
Following the wide surgical resection and epimesial dissection of the sciatic nerve, the patient underwent postoperative management. Given the history of neoadjuvant radiation therapy, which of the following is the *most* critical aspect of acute postoperative wound management?
Correct Answer: C
The most critical aspect of acute postoperative wound management, especially after neoadjuvant radiation, is meticulous drain management, leaving drains in until output is consistently low, to prevent seroma and wound dehiscence. The case highlights this: 'Drain management is critical. The closed-suction drains were left in place until the output decreased to less than 30 cc per 24-hour period for two consecutive days. In irradiated fields, lymphatic leakage can be prolonged, and premature drain removal frequently leads to seroma formation and subsequent wound dehiscence.'
Option A (Early aggressive range of motion exercises to prevent stiffness): While rehabilitation is important, early aggressive range of motion could jeopardize wound healing, especially in an irradiated field prone to dehiscence. Rehabilitation is phased and carefully progressed.
Option B (Immediate removal of surgical drains within 24 hours to reduce infection risk): This is incorrect. Premature drain removal in irradiated fields is a major cause of seroma and wound complications, as lymphatic leakage can be prolonged. Drains are kept in longer than usual.
Option D (High-dose systemic corticosteroids to reduce inflammation and promote wound healing): Corticosteroids can impair wound healing and increase infection risk, especially in the context of surgery and radiation. They are generally not used routinely for this purpose.
Option E (Strict bed rest for the first week to minimize stress on the wound): While activity is restricted, strict bed rest is generally avoided due to the risk of DVT and other complications. Early mobilization within safe limits is encouraged, along with DVT prophylaxis.
A 45-year-old male presents with a deep, painless thigh mass. MRI shows a predominantly fatty lesion with thin septations (<2mm) and no enhancing non-fatty components. A biopsy confirms mature adipocytes with no atypia. In contrast, Mr. J.A.'s tumor was a Dedifferentiated Liposarcoma. Which of the following features *most* reliably distinguishes Mr. J.A.'s tumor from the 45-year-old male's lesion?
Correct Answer: D
The features that most reliably distinguish Mr. J.A.'s Dedifferentiated Liposarcoma from the 45-year-old male's lesion (which sounds like a simple lipoma or possibly an atypical lipomatous tumor without dedifferentiation) are the identification of thickened, irregular septations and enhancing non-fatty nodules on MRI, along with MDM2/CDK4 amplification. The case explicitly states that these MRI findings are the 'classic radiological hallmark' of ALT/WDLPS/DDLPS, and MDM2/CDK4 amplification is the 'diagnostic hallmark' distinguishing it from other sarcomas and benign lesions.
Option A (The presence of a deep-seated mass): Both simple lipomas and liposarcomas can be deep-seated (intramuscular). This alone does not distinguish them.
Option B (The absence of pain): Both benign lipomas and many liposarcomas (including Mr. J.A.'s) can be painless. Pain is not a reliable distinguishing factor.
Option C (The presence of macroscopic fat on MRI): Both simple lipomas and well-differentiated/dedifferentiated liposarcomas contain macroscopic fat and would show high signal on T1-weighted images. This feature alone does not differentiate them.
Option E (The patient's age at presentation): While liposarcomas are more common in older adults, and the 45-year-old is younger than Mr. J.A. (62), age is not a definitive diagnostic criterion. Both benign and malignant lesions can occur across a wide age range.
None
