Valgus Osteotomy for Developmental Coxa Vara: An Intraoperative Masterclass

Key Takeaway
This masterclass details valgus osteotomy for developmental coxa vara, a proximal femoral deformity. We cover critical preoperative planning, precise patient positioning, and a step-by-step intraoperative guide for K-wire, Wagner, and blade plate fixation techniques. Comprehensive surgical anatomy, neurovascular considerations, and extensive pearls and pitfalls are discussed to ensure optimal outcomes and manage potential complications effectively.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are tackling a fascinating and often profoundly challenging pediatric deformity: developmental coxa vara. This is not merely a routine surgical procedure; it is a rigorous exercise in meticulous three-dimensional planning, precise osseous execution, and a deep, nuanced understanding of pediatric hip biomechanics. Our primary objective is to correct a progressive varus deformity of the proximal femur, aiming to definitively restore a more physiological neck-shaft angle, neutralize pathological shear forces across the physis, and prevent devastating long-term complications such as premature degenerative osteoarthritis and permanent abductor dysfunction.
Before we make our initial incision, it is imperative that we briefly review the underlying pathology and epidemiology of this condition. Developmental coxa vara, historically referred to as cervical or infantile coxa vara, is a progressive, insidious deformity of the proximal femur characterized strictly by a neck–shaft angle (NSA) of less than 110 degrees. Crucially, it is not present at birth. Instead, it typically manifests clinically between the initiation of independent ambulation and six years of age. This delayed presentation is the key clinical differentiator from congenital forms of coxa vara, which are present at birth and are frequently linked to broader embryonic limb bud abnormalities, such as proximal femoral focal deficiency (PFFD). Furthermore, it must be distinguished from acquired forms of coxa vara that arise secondary to identifiable metabolic disorders (like rickets), traumatic physeal arrests, or oncologic etiologies.
The exact patho-etiology of developmental coxa vara remains a subject of academic debate, yet the most widely accepted paradigm is Pylkkänen's theory. This theory posits a primary, localized ossification defect occurring within the medial aspect of the femoral neck. This intrinsic defect leads to a progressively more vertical orientation of the proximal femoral physis. Consequently, dystrophic bone formation occurs on the medial, inferior aspect of the femoral neck. When this dysplastic bone is subjected to the physiological, repetitive weight-bearing stresses of early childhood ambulation, it fatigues. The mechanical failure of this medial bone column leads to a progressive varus collapse of the femoral head and neck relative to the shaft.
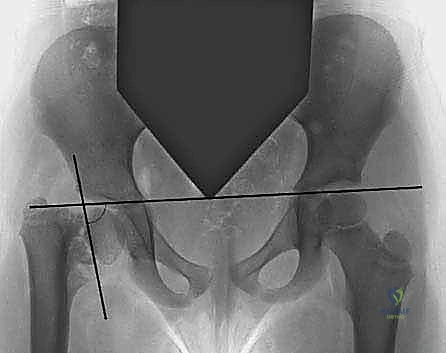
The natural history of developmental coxa vara dictates that, without intervention, this deformity frequently, if not invariably, progresses. The most reliable, validated prognostic indicator in our armamentarium is the Hilgenreiner–epiphyseal angle (HEA). This is measured on an anteroposterior pelvic radiograph between Hilgenreiner's line (a horizontal line drawn through the triradiate cartilages) and a line drawn parallel to the proximal femoral physis. Extensive natural history studies have demonstrated that patients with an HEA greater than 60 degrees will invariably progress, cementing their status as prime candidates for surgical intervention. Conversely, those with an HEA between 45 and 60 degrees occupy a clinical gray zone, requiring vigilant, serial radiographic monitoring for progression or the onset of increasing clinical symptoms.
Detailed Surgical Anatomy and Biomechanics
To execute a valgus producing osteotomy safely and effectively, we must first orient ourselves with the critical, highly specialized anatomy of the pediatric proximal femur. The proximal femoral physis is the primary growth center responsible for the longitudinal growth of the femoral neck. In the setting of developmental coxa vara, this physis is characteristically abnormal; it is wider, structurally disorganized, and significantly more vertical than in a physiological hip. It frequently presents radiographically with a pathognomonic "inverted Y-pattern," which is caused by the presence of a triangular metaphyseal bone fragment—often termed Fairbank's triangle—located in the inferior aspect of the femoral neck. Any iatrogenic vascular or mechanical injury to this already precarious physis during our surgical approach can catastrophically exacerbate the varus deformity.
The greater trochanteric apophysis plays a central role in the clinical presentation and biomechanical failure seen in this condition. This apophysis is responsible for the growth of the greater trochanter. Because the longitudinal growth of the femoral neck is stunted by the diseased proximal physis, the greater trochanter experiences relative overgrowth. This leads to severe trochanteric prominence and a negative articulotrochanteric distance (ATD). Biomechanically, this proximal migration of the greater trochanter drastically shortens the lever arm of the hip abductor musculature (gluteus medius and minimus). This mechanical disadvantage is the direct anatomical cause of the classic painless, waddling Trendelenburg gait that these children exhibit.
Furthermore, we must deeply understand the concept of the neck-shaft angle (NSA) and femoral version in this patient population. Normally, the NSA progresses from approximately 150 degrees at birth to around 120 to 130 degrees at full skeletal maturity. In developmental coxa vara, this angle is significantly decreased, frequently presenting at less than 90 degrees in severe, neglected cases. Additionally, while the pediatric femur is typically anteverted, developmental coxa vara is uniquely associated with decreased femoral anteversion or, in severe cases, frank retroversion. This retrotorsion can contribute to anterior femoroacetabular impingement, limit internal rotation, and must be explicitly addressed with a derotational component during our osteotomy.
Finally, navigating the neurovascular and muscular intervals is paramount. Our approach today utilizes the standard lateral approach to the proximal femur. This involves splitting the fascia lata longitudinally and elevating the vastus lateralis. Deep subperiosteal dissection around the femur requires extreme vigilance to minimize bleeding from the perforating arteries—branches of the profunda femoris that pierce the adductor magnus and vastus lateralis. More importantly, the blood supply to the femoral head, primarily derived from the medial circumflex femoral artery (MCFA), must be protected. The deep branch of the MCFA courses posteriorly along the femoral neck; thus, straying outside the subperiosteal plane during our capsular or neck dissection risks catastrophic iatrogenic avascular necrosis (AVN).
Exhaustive Indications and Contraindications
The decision to proceed with a valgus osteotomy is predicated on a synthesis of clinical symptomatology and strict radiographic parameters. Clinically, these patients typically present to the orthopedic clinic with a progressive, painless limp. Pain is notably uncommon in the early stages of the disease, and its presence should prompt an investigation into alternative diagnoses such as slipped capital femoral epiphysis (SCFE) or infection. Unilateral involvement invariably leads to profound abductor weakness, manifesting as a positive Trendelenburg sign, and a measurable limb-length discrepancy (LLD), usually less than 2.5 cm. Bilateral involvement presents as a pronounced waddling gait accompanied by a compensatory increase in lumbar lordosis to maintain sagittal balance.
Radiographic indications are the ultimate arbiter for surgical intervention. As previously discussed, an HEA exceeding 60 degrees is an absolute indication for surgery, as progression is a biomechanical certainty. Furthermore, a documented neck-shaft angle (NSA) of less than 110 degrees that demonstrates progression on serial radiographs warrants intervention. The primary biomechanical goal of the surgery is to convert the pathological shearing forces acting across the vertical physis into physiological compressive forces. By valgus-producing the proximal femur, we horizontalize the physis, which not only halts the progression of the deformity but frequently induces spontaneous healing and ossification of the defective medial metaphyseal bone.
Contraindications to this procedure are relatively few but absolutely critical to respect. Active, untreated local or systemic infection is an absolute contraindication to any elective orthopedic osteotomy and hardware implantation. Additionally, patients with severe, uncorrectable metabolic bone diseases (such as refractory hypophosphatemic rickets) may experience rapid recurrence of the deformity if the underlying metabolic milieu is not medically optimized prior to surgery. Relative contraindications include extreme patient youth (where observation may still be warranted if the HEA is borderline) or profound neurological compromise where the patient lacks the muscular control to benefit from the improved biomechanics of the hip joint.
Below is a comprehensive table summarizing the indications and contraindications for valgus osteotomy in developmental coxa vara:
| Category | Specific Criteria / Condition | Clinical Rationale |
|---|---|---|
| Absolute Indications | Hilgenreiner-Epiphyseal Angle (HEA) > 60° | Invariable progression of varus deformity due to unmitigated shear forces. |
| Absolute Indications | Documented progressive decrease in NSA | Indicates active mechanical failure of the medial femoral neck. |
| Relative Indications | HEA between 45° and 60° with clinical decline | "Gray zone" requiring intervention if limp or LLD worsens significantly. |
| Relative Indications | Significant abductor weakness / Trendelenburg | Warrants correction to restore the abductor lever arm and prevent joint degeneration. |
| Absolute Contraindications | Active local or systemic infection | High risk of deep hardware infection and catastrophic osteomyelitis. |
| Relative Contraindications | Unoptimized metabolic bone disease | High risk of hardware failure, nonunion, or rapid recurrence of the varus deformity. |
Pre-Operative Planning, Templating, and Patient Positioning
Fellows, the success of this operation hinges entirely on meticulous, obsessive preoperative planning. The operating room is not the place to make geometric decisions; we need a flawless roadmap before the patient even enters the suite. Our planning begins with a comprehensive clinical assessment, verifying the precise degree of limb-length discrepancy and rotational profile of the lower extremity. This physical data must correlate perfectly with our imaging findings to ensure we address all components of the deformity—varus, shortening, and retroversion.
Our imaging review must be exhaustive. The cornerstone of our planning is a high-quality, standing anteroposterior (AP) pelvic radiograph. On this view, we will meticulously measure the current NSA, the Hilgenreiner–epiphyseal angle (HEA), and assess for the classic inverted-Y pattern, coxa breva, and any secondary acetabular dysplasia.
We must also obtain a true frog-leg lateral radiograph. This specific view is indispensable for assessing the degree of femoral retrotilt or frank retroversion, which is a common concomitant deformity in developmental coxa vara that must be corrected to restore normal hip kinematics.

In the modern era, advanced imaging modalities such as CT or MRI are frequently utilized to provide infinitely more detailed information. A 3D CT reconstruction, in particular, offers an invaluable, rotatable perspective on the complex 3D morphology of the proximal physis and the exact degree of version. This allows us to plan our osteotomy cuts with sub-millimeter precision.



Templating is the phase where we mathematically determine our desired alignment. We will draw out the planned osteotomy on digital or physical templates to determine the precise amount of valgus correction needed. Our goal is to achieve a postoperative NSA of 140 to 160 degrees and reduce the HEA to less than 35 degrees. We must also calculate the exact size of the laterally based closing wedge (if performing a wedge osteotomy) or the angle of our blade plate. Implant selection is dictated by the patient's age and bone caliber: multiple Kirschner wires are ideal for very young children (under 4 years) with small bones, while a custom-made high-angle pediatric blade plate or a locking proximal femoral plate is preferred for older children requiring robust, rigid fixation.
Patient positioning sets the stage for intraoperative success. The patient is placed supine on a fully radiolucent operating table. We place a folded blanket or a specialized bump beneath the ipsilateral pelvis. This slight elevation stabilizes the hemipelvis and provides the necessary clearance for the C-arm fluoroscopy unit to obtain unhindered, true AP and lateral views of the proximal femur. The entire lower extremity must be prepped and draped free. This free draping is an absolute requirement, as it allows the surgeon to manipulate the leg through a full range of motion to assess the adequacy of the reduction, the restoration of version, and the stability of the osteotomy prior to final closure.
Step-by-Step Surgical Approach and Fixation Technique
Alright, fellows, scalpels ready. Let's begin the execution phase. We are utilizing the standard lateral approach to the proximal femur. I am making a longitudinal incision, typically 8 to 12 cm in length, centered precisely over the palpable greater trochanter and extending distally along the lateral midline of the thigh. We must be continuously mindful of the lateral femoral cutaneous nerve superficially; careful blunt dissection through the subcutaneous fat will help protect it. We then identify the fascia lata and split it longitudinally in line with its fibers using electrocautery, extending the split proximally to the tip of the trochanter.
Deep to the fascia, we identify the vastus lateralis. We incise its fascia longitudinally, approximately 5 to 10 mm anterior to the dense lateral intermuscular septum. Using a Cobb elevator, we carefully and atraumatically elevate the vastus lateralis from the lateral aspect of the femur. To gain adequate exposure for our osteotomy and hardware placement, we must release the vastus lateralis proximally. I make a transverse incision through the muscle belly just distal to the level of the greater trochanteric apophysis. We then incise the periosteum and perform a meticulous, circumferential subperiosteal dissection around the proximal femur, staying intimately on the bone to avoid avulsing the posterior perforating vessels.
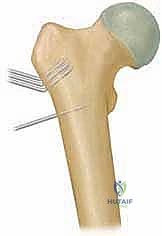
Now, let's proceed with the K-wire technique, typically reserved for our youngest pediatric patients where a blade plate would be too bulky. My assistant, please hand me the first threaded Kirschner wire. Under live AP fluoroscopic guidance, I am advancing this first heavy, threaded K-wire through the lateral cortex of the proximal femur, aiming up into the center of the femoral neck and head. The trajectory of this wire is critical; it must represent the planned valgus angle relative to the femoral shaft. We typically place two to three parallel threaded wires into the proximal fragment to ensure absolute rotational control.
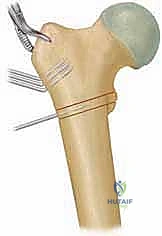
Once the proximal wires are securely seated short of the articular surface, we mark our osteotomy site just proximal to the lesser trochanter. If derotation is required for retroversion, we score the anterior cortex longitudinally with the Bovie to serve as a rotational reference. Using an oscillating saw under continuous saline irrigation to prevent thermal necrosis, we perform a transverse or slightly oblique osteotomy. The distal fragment is then abducted (valgus-producing maneuver) and, if necessary, internally rotated.
For older children, we transition to the blade plate technique. Prior to the osteotomy, the seating chisel is driven into the femoral neck at the predetermined angle (e.g., 130 degrees relative to the shaft if aiming for a 140-degree NSA with a 10-degree wedge). The osteotomy is then performed, and a laterally based wedge of bone is removed. The seating chisel is extracted, and the definitive blade plate is inserted into the prepared track.

The distal fragment is brought to the plate, effectively closing the wedge and creating the valgus correction. The plate is then secured to the femoral shaft with cortical screws. We utilize a dynamic compression principle to ensure the osteotomy site is rigidly compressed, which is vital for primary bone healing. Fluoroscopy confirms the final NSA, the horizontalization of the physis, and the correct placement of all hardware.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and flawless execution, complications in the surgical management of developmental coxa vara can and do occur. As academic surgeons, we must be intimately familiar with these pitfalls, their incidence rates, and the appropriate salvage strategies. The most common complication is undercorrection or recurrence of the varus deformity. This typically occurs if the surgeon fails to achieve an HEA of less than 35 degrees or an NSA of at least 140 degrees. Recurrence rates can approach 15-20% in cases of inadequate initial correction. Salvage requires a revision valgus osteotomy, often utilizing more rigid internal fixation and potentially incorporating a larger closing wedge.
Premature physeal closure is another significant risk, occurring in up to 10% of cases. This can be caused by the natural progression of the diseased physis, but it is frequently iatrogenic, resulting from hardware crossing the physis or thermal necrosis during the osteotomy. If the physis closes prematurely, it exacerbates the limb-length discrepancy and trochanteric overgrowth. Management may require a contralateral distal femoral epiphysiodesis to manage the LLD, or a distal and lateral transfer of the greater trochanter to restore the abductor lever arm.
Avascular necrosis (AVN) of the femoral head is the most devastating complication, though fortunately rare (incidence < 2%) in purely extracapsular valgus osteotomies. It is usually the result of straying from the subperiosteal plane posteriorly and injuring the medial circumflex femoral artery, or from placing hardware that violates the superior-posterior retinacular vessels. If AVN occurs, management is complex and depends on the extent of head involvement, ranging from prolonged non-weight-bearing and bracing to, in severe late-stage collapse, complex pelvic support osteotomies or eventual total hip arthroplasty.
Below is a table summarizing the primary complications, their estimated incidence, and standard salvage management:
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Recurrence / Undercorrection | 10% - 20% | Failure to reduce HEA < 35°; inadequate valgus angle achieved. | Revision valgus osteotomy with rigid plate fixation. |
| Premature Physeal Closure | 5% - 10% | Iatrogenic hardware violation of physis; thermal necrosis. | Epiphysiodesis for LLD; Trochanteric advancement for abductor weakness. |
| Hardware Failure / Migration | 2% - 5% | Poor bone quality; non-compliance with weight-bearing restrictions. | Revision internal fixation; potential use of bone grafting. |
| Avascular Necrosis (AVN) | < 2% | Injury to MCFA during dissection; superior retinacular vessel injury. | Containment bracing; core decompression; late reconstructive osteotomies. |
Phased Post-Operative Rehabilitation Protocols
The surgical procedure concludes when the patient leaves the operating room, but the success of the intervention relies heavily on a strictly managed, phased postoperative rehabilitation protocol. The immediate postoperative phase (Weeks 0-6) is focused entirely on protecting the osteotomy site to allow for initial callus formation and osseous union. For younger patients treated with K-wires, a one-and-a-half spica cast is almost universally applied in the operating room to ensure absolute immobilization and prevent catastrophic hardware migration. For older children treated with rigid blade plates or locking plates, a spica cast may be avoided, but the patient is placed on strict non-weight-bearing or toe-touch weight-bearing precautions using a walker or crutches.
Phase two (Weeks 6-12) begins once radiographic evidence of bridging callus is observed at the osteotomy site. At this juncture, the spica cast is removed in the clinic. If K-wires were utilized and left protruding through the skin (or buried just beneath), they are typically removed at this stage under light sedation or in the clinic setting. The patient is then transitioned to partial weight-bearing. Physical therapy is initiated with a primary focus on restoring active and passive range of motion to the hip and knee, which often become stiff during the period of immobilization. Aquatic therapy is highly beneficial during this phase.
Phase three (Months 3-6) represents the return to full functional activity. Once complete radiographic union is confirmed, the patient is advanced to full, unrestricted weight-bearing. The physical therapy paradigm shifts aggressively toward strengthening the hip abductor complex (gluteus medius and minimus). Because the valgus osteotomy has restored the mechanical lever arm, these muscles must be rehabilitated to overcome years of preoperative mechanical disadvantage. Final hardware removal (for blade plates or locking plates) is generally considered 12 to 18 months postoperatively, assuming complete remodeling of the osteotomy site has occurred, to prevent stress shielding and facilitate future imaging or interventions.
Summary of Landmark Literature and Clinical Guidelines
To practice evidence-based orthopedic surgery, we must stand on the shoulders of the giants who elucidated the principles we employ today. The modern management of developmental coxa vara is heavily heavily influenced by the landmark natural history studies conducted by Weinstein et al. Their rigorous longitudinal follow-up of these patients firmly established the Hilgenreiner-epiphyseal angle (HEA) as the paramount prognostic indicator. They definitively proved that an HEA greater than 60 degrees is an absolute harbinger of progression, shifting the orthopedic paradigm from watchful waiting to proactive surgical intervention in these high-risk patients.
Furthermore, the work of Amstutz and Wilson in the mid-20th century provided the foundational classification systems and highlighted the biomechanical necessity of the valgus osteotomy. They elegantly described how converting shear forces to compressive forces not only halts deformity progression but stimulates the physiological ossification of the medial cervical defect. Their long-term outcome studies validated the use of laterally based closing wedge osteotomies to achieve these biomechanical goals.
Finally, the technical refinements introduced by Carroll and others regarding the use of multiple threaded Kirschner wires in the very young pediatric population revolutionized our approach to toddlers with this condition. By demonstrating that rigid fixation could be achieved without the need for massive, bone-displacing hardware, they minimized the risk of iatrogenic physeal arrest and avascular necrosis in the smallest femurs. As you move forward in your careers, fellows, I urge you to revisit these classic texts. A deep mastery of the literature is what separates a competent technician from a true master orthopedic surgeon.
