Ulnar Dimelia (Mirror Hand): Pathoanatomy, Biomechanics, and Surgical Reconstruction

Key Takeaway
Ulnar dimelia, or "mirror hand," is an exceedingly rare congenital anomaly characterized by a duplication of the ulnar half of the upper extremity. Patients typically present with an absent radius, duplicated ulna, and a symmetrical hand featuring six to eight digits with an absent thumb. Surgical reconstruction focuses on excising supernumerary preaxial digits, performing pollicization to restore pinch and grasp, and addressing associated elbow and wrist contractures.
INTRODUCTION TO ULNAR DIMELIA
Ulnar dimelia, classically referred to as "mirror hand," is an exceedingly rare and complex congenital anomaly of the upper extremity. It is characterized by the duplication of the ulnar half of the forearm, wrist, and hand, accompanied by a complete absence of the radial components. Because there is a complete substitution of the radial structures with duplicated ulnar structures, this anomaly defies simple classification as a pure duplication and is instead considered a profound embryological patterning error.
The condition presents with radial and ulnar clusters of fingers in the same hand that are near-mirror images of each other. The largest historical series reported in the literature is that of Harrison, Pearson, and Roaf, who meticulously described the deformity and its functional implications in three patients.
Embryology and Pathogenesis
The exact etiology of ulnar dimelia remains largely unknown, and its occurrence is almost exclusively sporadic. However, advances in molecular embryology have elucidated the underlying mechanisms. The deformity is believed to result from a severe aberration in the control process of the limb bud, specifically involving the Zone of Polarizing Activity (ZPA) and the Apical Ectodermal Ridge (AER).
Clinical Pearl: Molecular Basis of Mirror Hand
The ZPA, located at the posterior margin of the developing limb bud, secretes the Sonic Hedgehog (SHH) morphogen, which dictates the radioulnar (anterior-posterior) axis. An ectopic expression of SHH at the anterior margin of the limb bud creates a second ZPA, leading to a duplication of the posterior (ulnar) structures and a failure of anterior (radial) structure formation.
While typically sporadic, when ulnar dimelia is associated with fibular dimelia (duplication of the fibula with an absent tibia), it may be explained as a single gene mutation transmitted as an autosomal dominant trait (e.g., Laurin-Sandrow syndrome). Furthermore, ulnar dimelia is frequently associated with some degree of hypoplasia of the proximal humerus, arm musculature, and scapula.
CLINICAL PRESENTATION AND PATHOANATOMY
The clinical appearance of ulnar dimelia is usually unilateral and visually striking. The hand typically features six to eight well-formed fingers that dangle from a broadened, normal-appearing palm.
Hand and Wrist Manifestations
- Digit Configuration: The digits may all lie in nearly the same plane, or there may be slight opposition between the two halves of the hand.
- Preaxial vs. Postaxial Digits: The postaxial (true ulnar) digits generally appear slightly more normal in structure and function than the preaxial (duplicated ulnar/ectopic) digits.
- Absent Thumb: A true thumb is universally absent, severely compromising pinch and grasp biomechanics.
- Syndactyly: Complex or simple syndactyly is frequently present between the duplicated digits.
- Flexion Contractures: The digits are often held in a flexed posture due to deficient or absent extrinsic extensor tendons.
- Wrist Deformity: The hand is usually severely radially deviated at the wrist, and active extension of the wrist may be impossible due to the absence of the radial wrist extensors (ECRL, ECRB).
Forearm and Elbow Manifestations
- Thickened Joints: Both the wrist and elbow appear abnormally thick and broad.
- Elbow Stiffness: Elbow motion is profoundly decreased. This is due to the presence of two olecranons articulating with the distal humerus, often in a restricted or fused manner.
- Forearm Rotation: Pronation and supination are entirely absent because the two ulnas are tethered together, and the normal radioulnar joints do not exist.
RADIOGRAPHIC EVALUATION
Standard orthogonal radiographs of the entire upper extremity are mandatory. Imaging will reveal the absence of the radius and the presence of two ulnas. The carpus is widened, often with duplicated triquetrum, hamate, and pisiform bones, while the scaphoid and trapezium are absent.
Surgical Warning: Vascular Anatomy
Never proceed to surgical reconstruction of a mirror hand without advanced vascular imaging (MR Angiography or conventional angiography). The vascular tree is highly anomalous, typically featuring a duplicated ulnar artery and an absent radial artery. The palmar arches are often incomplete, and indiscriminate excision of preaxial digits can inadvertently devascularize the remaining hand.
SURGICAL PRINCIPLES AND DECISION MAKING
The primary goal of surgical intervention is to transform a non-functional, multi-digited appendage into a functional hand with a functional thumb, while simultaneously improving the alignment and motion of the wrist and elbow.
Surgical reconstruction is typically staged and initiated when the child is between 12 and 18 months of age. The core objectives include:
1. Restoration of Pinch and Grasp: Achieved via pollicization of the most functional preaxial digit.
2. Reduction of Digit Count: Excision of supernumerary, non-functional preaxial digits to narrow the hand and improve aesthetics.
3. Correction of Wrist Deviation: Realignment of the carpus over the dominant ulna.
4. Improvement of Elbow Motion: Excision of the preaxial olecranon to unlock the elbow joint.
OPERATIVE TECHNIQUE: ULNAR DIMELIA RECONSTRUCTION
Stage 1: Pollicization and Digit Excision
The most critical step in hand reconstruction is selecting the appropriate preaxial digit for pollicization. The chosen digit must have the best active mobility, adequate length, and a reliable neurovascular pedicle. Usually, the second or third digit from the preaxial border is selected.
- Incision and Exposure: A racquet-shaped incision is designed around the base of the digit chosen for pollicization. Elliptical incisions are planned for the excision of the remaining supernumerary preaxial digits.
- Neurovascular Dissection: The common digital nerves and arteries are meticulously dissected proximally into the palm. The anomalous vascular arch must be identified. The vessels to the digits slated for amputation are ligated, preserving the dominant pedicle to the pollicized digit.
- Digit Amputation: The supernumerary digits are amputated at the carpometacarpal level. The metacarpals of these digits are excised to narrow the palm, but their intrinsic muscles are carefully preserved for later transfer.
- Skeletal Shortening and Rotation (Buck-Gramcko Principle): The metacarpal of the pollicized digit is shortened. The metacarpal head is preserved to act as the new trapezium, and the metacarpophalangeal (MCP) joint becomes the new carpometacarpal (CMC) joint of the thumb. The digit is rotated 160 degrees into pronation and palmar abducted to oppose the remaining fingers.
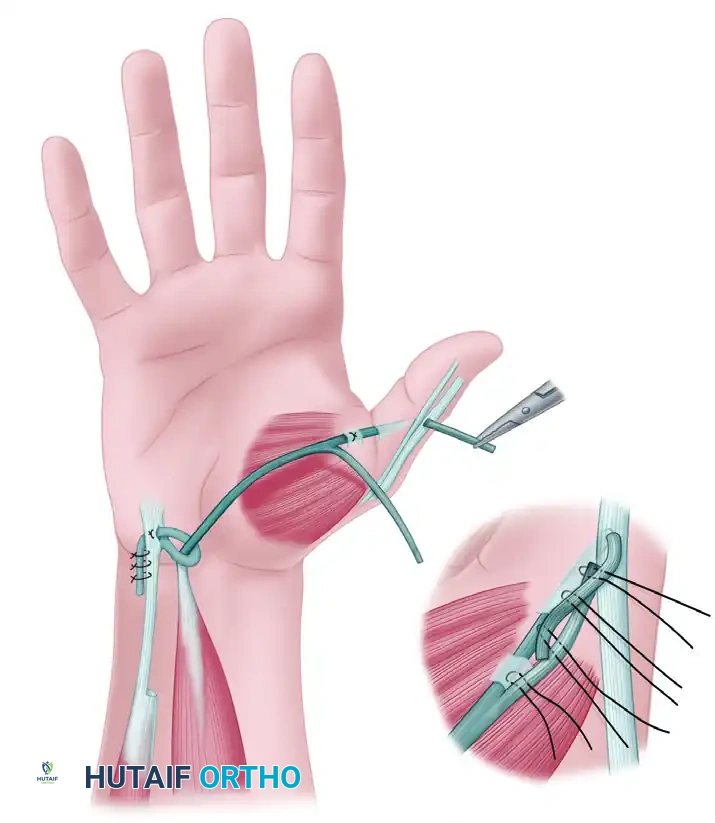
- Tendon Transfers:
- The preserved intrinsic muscles from the amputated digits are transferred to the new thumb to provide thenar function (abduction and opposition).
- The extensor digitorum communis of the pollicized digit is shortened and reattached to function as the extensor pollicis longus.
- Closure: The skin flaps are transposed to create a wide, deep first web space.
Stage 2: Elbow and Wrist Reconstruction
Elbow stiffness is a major functional limiting factor. The presence of a duplicated, preaxial ulna creates a mechanical block to flexion and extension.
- Preaxial Olecranon Excision: Through a lateral approach to the elbow, the proximal portion of the preaxial (ectopic) ulna, including its olecranon, is excised. Care must be taken to preserve the triceps insertion on the dominant, postaxial ulna.
- Capsular Release: An anterior capsulotomy of the elbow may be required to achieve functional flexion.
- Wrist Centralization: If severe radial deviation persists despite the narrowing of the hand, a centralization procedure (similar to that used in radial clubhand) may be performed, seating the carpus squarely on the distal articular surface of the dominant ulna.
MANAGEMENT OF ASSOCIATED POLYDACTYLY
While ulnar dimelia represents a profound duplication of the entire ulnar axis, surgeons frequently encounter isolated duplication anomalies (polydactyly) in pediatric orthopedics. The management of these extra digits depends heavily on their morphological classification.
Type 1 Duplications (Pedunculated Extra Digits)
Type 1 polydactyly consists of a soft-tissue appendage devoid of skeletal articulation, attached to the hand by a narrow skin pedicle. Historically, these were managed in the neonatal nursery with suture ligation.
Surgical Warning: Suture Ligation of Pedunculated Digits
Suture ligation (tying off the digit with a silk tie to induce necrosis) is strictly not recommended. There are documented reports of fatal hemorrhage following the sloughing of the necrotic digit, as well as risks of severe infection and painful neuroma formation.
Evidence-Based Management (Katz and Linder Technique):
Katz and Linder reported a highly successful prospective series of 11 infants with pedunculated extra digits managed via sharp excision.
* Setting: Outpatient clinic or minor procedure room.
* Anesthesia: Topical anesthesia (e.g., EMLA cream) applied to the base of the pedicle.
* Technique: Digital traction is applied to the extra digit. A single, decisive swipe of a #15 scalpel is used to excise the digit flush at its base.
* Hemostasis: Direct, sustained pressure is applied to control bleeding. Electrocautery is rarely needed.
* Closure: The skin edges are approximated with a sterile adhesive strip (Steri-Strip).
* Outcomes: In the Katz and Linder series, all infants cried for only "a few seconds after the excision," no complications were encountered, and at the 1-year follow-up, the excision site was barely visible.
Type 2 Duplications (Articulating Extra Digits)
Type 2 duplications contain skeletal elements (phalanges and/or metacarpals) and articulate with the hand skeleton. These cannot be managed with simple clinic excision.
- Timing: Excision should be performed in the operating room under general anesthesia, usually when the child is approximately 1 year old.
- Technique: The extra digit is excised through a carefully planned elliptical incision at its base. The dissection must identify and protect the neurovascular bundles of the adjacent normal digit.
- Skeletal Management: The duplicated skeletal elements are excised.
- Pitfall Avoidance: A frequent complication of Type 2 excision is an unsightly, painful bump caused by a retained segment of the duplicated metacarpal head or a flaring of the shared epiphysis. To prevent this, the surgeon must perform a longitudinal osteotomy to shave down the flaring of the remaining metacarpal head, ensuring a smooth contour. The collateral ligaments must be meticulously reconstructed to prevent angular deformity of the remaining digit.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Following complex reconstruction for ulnar dimelia, meticulous postoperative care is paramount to ensure graft survival and functional outcome.
- Immobilization: The upper extremity is immobilized in a bulky, long-arm spica cast or a well-padded splint. The elbow is held at 90 degrees of flexion, the wrist in neutral, and the newly pollicized thumb is protected in palmar abduction and opposition.
- Pin Removal: If Kirschner wires were used to stabilize the CMC joint of the new thumb or the centralized wrist, they are typically removed in the clinic at 4 to 6 weeks postoperatively.
- Occupational Therapy: Intensive, specialized pediatric hand therapy begins immediately upon cast removal. Therapy focuses on:
- Scar massage and desensitization.
- Fabrication of a custom thermoplastic thumb spica splint for nighttime use.
- Play-based therapy to encourage cortical integration of the new thumb, promoting active pinch and grasp.
- Long-Term Surveillance: Patients require follow-up until skeletal maturity. Growth spurts can unmask tethering from scar tissue, recurrent wrist deviation, or progressive elbow stiffness, which may necessitate secondary soft-tissue releases or corrective osteotomies.
📚 Medical References
- Bhaskaranand K, Bhaskaranand N, Bhat AK: A variant of mirror hand: a case report, J Hand Surg 28A:678, 2003.
- Buck-Gramcko D: Operative Behandlung einer SpiegelbildDeformität der hand (mirror hand—doppelte ulna mit polydaktylie): traitement operatoire d’une difformite en miroir de l’avant-bras (deboublement du cutitus et des doigts cubitaux), Ann Chir Plast 9:180, 1964.
- Entin MA: Reconstruction of congenital abnormalities of the upper extremity, J Bone Joint Surg 41A:681, 1959.
- Entin MA: Congenital anomalies of the upper extremity, Surg Clin North Am 40:497, 1960.
- Gorriz G: Ulnar dimelia—a limb without anteroposterior differentiation, J Hand Surg 7A:466, 1982.
- Harrison RG, Pearson MA, Roaf R: Ulnar dimelia, J Bone Joint Surg 42B:549, 1960.
- Turek SL: Orthopaedic principles and their application, Philadelphia, 1967, Lippincott.
You Might Also Like