Mastering Wrist Ligament Injuries and Carpal Instability: A Comprehensive Surgical Guide

Key Takeaway
The management of wrist ligament injuries and carpal instability requires a profound understanding of carpal kinematics. Treatment ranges from arthroscopic pinning for acute Geissler Grade II tears to salvage procedures like proximal row carpectomy for chronic, fixed deformities. This guide details the biomechanics, diagnostic maneuvers, and step-by-step surgical approaches—including dorsal capsulodesis and combined exposures—essential for restoring radiocarpal stability and preventing progressive arthrosis in the complex wrist joint.
INTRODUCTION TO WRIST LIGAMENT INJURIES AND INSTABILITY
The human carpus is a highly complex, intercalated biomechanical linkage system that relies entirely on its intricate ligamentous architecture for stability. Unlike the hip or shoulder, the carpal bones possess no inherent osseous stability; their kinematic harmony is dictated by the intrinsic (interosseous) and extrinsic (capsular) ligaments. Disruption of these restraints—whether through acute high-energy trauma or chronic repetitive microtrauma—leads to carpal instability, altered contact mechanics, and inevitably, progressive degenerative arthrosis such as Scapholunate Advanced Collapse (SLAC) or Volar Intercalated Segment Instability (VISI).
The management of wrist ligament injuries demands a meticulous diagnostic approach and a tailored surgical strategy. Treatment algorithms are dictated by the chronicity of the injury, the specific ligaments involved, the presence of fixed carpal malalignment, and the status of the articular cartilage.
Clinical Pearl: The golden window for treating carpal instability is in the acute phase (within 3 to 4 weeks). Missed diagnoses during this period exponentially increase the complexity of surgical reconstruction and decrease the likelihood of restoring normal wrist kinematics.
BIOMECHANICS AND PATHOANATOMY
Understanding the pathoanatomy of wrist instability requires dividing the ligamentous supports into two primary categories:
1. Intrinsic Ligaments: These originate and insert entirely within the carpus (e.g., scapholunate interosseous ligament [SLIL], lunotriquetral interosseous ligament [LTIL]). They are the primary stabilizers of the proximal carpal row.
2. Extrinsic Ligaments: These connect the radius or ulna to the carpus (e.g., radiocarpal ligaments, ulnocarpal ligaments). They act as secondary stabilizers and proprioceptive relays.
When the wrist is subjected to extreme axial loading, hyperextension, and rotational forces (pronation or supination), the ligaments fail in a predictable, sequential manner, famously described by Mayfield's stages of perilunate instability.
DIAGNOSTIC CLASSIFICATION: THE GEISSLER GRADING SYSTEM
While static and dynamic radiographs are foundational, wrist arthroscopy remains the gold standard for diagnosing and classifying interosseous ligament tears. The Geissler Classification correlates arthroscopic findings with the degree of instability, directly guiding the treatment protocol.
Geissler Classification of Carpal Instability
- Grade I:
- Description: Attenuation or hemorrhage of the interosseous ligament as viewed from the radiocarpal space. There is no incongruency of carpal alignment in the midcarpal space.
- Treatment: Conservative management with rigid immobilization in a cast for 4 to 6 weeks.
- Grade II:
- Description: Attenuation or hemorrhage of the interosseous ligament seen from the radiocarpal space. Incongruency or a step-off is visible in the midcarpal space. A slight gap (less than the width of the arthroscopic probe) may be present between the carpal bones.
- Treatment: Arthroscopic debridement and percutaneous pinning to stabilize the interval while healing occurs.
- Grade III:
- Description: Distinct incongruency or step-off of carpal alignment seen from both the radiocarpal and midcarpal spaces. The arthroscopic probe can be passed freely through the gap between the carpal bones.
- Treatment: Arthroscopic pinning or formal open repair, depending on tissue quality and surgeon experience.
- Grade IV:
- Description: Severe incongruency or step-off of carpal alignment. Gross instability is evident with manipulation. A standard 2.7-mm arthroscope can be passed directly through the gap between the carpal bones (the "drive-through" sign).
- Treatment: Formal open repair, often augmented with capsulodesis or ligament reconstruction.
SPECIFIC INJURY PATTERNS AND CLINICAL PRESENTATION
Triquetrolunate and Midcarpal Instabilities
Axial loading of a hyperextended, pronated wrist is the classic mechanism contributing to the injury of the ligamentous supports of the triquetrolunate (LT) and midcarpal joints. Disruption of the lunotriquetral interosseous ligament, the dorsal intercarpal (DIC) ligament, and the radiotriquetral ligaments leads to profound laxity on the ulnar side of the wrist.
Patients with triquetrolunate instability typically present with:
* Focal pain on the ulnar aspect of the wrist.
* A mechanical "click" or "clunk" during active radial and ulnar deviation.
* A history of a specific traumatic event, though chronic attritional tears can occur.
Physical Examination:
The hallmark of LT instability is localized tenderness over the LT interval. The Lunotriquetral Ballottement Test (Kleinman's Shear Test) is highly sensitive.
* Technique: The examiner stabilizes the lunate with the thumb and index finger of one hand. With the opposite hand, the examiner grasps the triquetrum and pisiform, attempting to displace them dorsally and palmarward relative to the lunate.
* Positive Finding: Excessive laxity, reproduction of the patient's pain, and palpable crepitance constitute a positive test.
Radiographic Evaluation:
If the triquetrolunate injury is merely a sprain or partial tear, standard static radiographs will appear normal. However, in cases of complete triquetrolunate dissociation, the triquetrum may displace proximally on the anteroposterior (AP) view. This displacement is often exaggerated during dynamic ulnar deviation views, creating a distinct overlapping shadow of the lunate and triquetrum. A disruption of the smooth Gilula's arcs is a critical radiographic red flag.
Dorsal Transscaphoid Perilunar Dislocations
Dorsal transscaphoid perilunar dislocations represent a severe disruption of the carpal architecture, combining a "greater arc" injury (scaphoid fracture) with a "lesser arc" injury (perilunate ligamentous disruption).
Surgical Warning: Similar to isolated scaphoid fractures, the diagnosis of a transscaphoid perilunar dislocation is frequently overlooked in the emergency setting, especially in polytrauma patients with distracting upper extremity injuries. A missed perilunate dislocation rapidly progresses to irreversible cartilage necrosis and severe carpal collapse.
- Acute Management: Early reduction by closed manipulation under conscious sedation or regional block is paramount to relieve tension on the median nerve and restore carpal perfusion. If accurate, anatomic reduction of the scaphoid fracture and carpal alignment is not obtained (which is common), prompt open reduction and internal fixation (ORIF) is mandatory. Bone grafting may be necessary if there is comminution at the scaphoid fracture site.
- Delayed Presentation: Closed reduction may occasionally be possible up to 3 weeks post-injury. However, these injuries almost universally require ORIF with Kirschner wires (K-wires) or headless compression screws for definitive stability.
- Chronic Presentation: While successful open reductions have been reported up to 6 weeks post-injury, attempting an open reduction after 2 months is fraught with complications due to severe soft tissue contracture and early chondral damage. In these late cases, salvage procedures such as Proximal Row Carpectomy (PRC) or partial/total wrist arthrodesis are indicated.
Palmar Transscaphoid Perilunar Dislocations
Palmar transscaphoid perilunar dislocations are exceedingly rare. They typically result from a high-energy fall on the dorsum of a hyper-flexed wrist. This mechanism is the exact biomechanical opposite of the hyperextension force that produces the much more common dorsal perilunar dislocation. Treatment principles mirror those of dorsal dislocations, though the surgical approach must be tailored to address the palmar displacement of the carpus.
SURGICAL TREATMENT ALGORITHMS
The surgical management of wrist instability is dictated by the chronicity of the injury and the presence of degenerative changes.
1. Acute Injuries (0 to 4 Weeks)
For acute wrist ligament injuries, the primary goal is anatomic restoration of the carpal relationships to allow primary ligamentous healing.
* Closed/Arthroscopic Methods: Arthroscopically controlled manipulation and percutaneous pinning (using 0.045-inch or 0.062-inch K-wires) are ideal for Geissler Grade II and some Grade III injuries.
* Open Methods: If closed or arthroscopic methods fail to achieve anatomic reduction, or in the presence of a Geissler Grade IV tear, formal open repair of the ligaments using suture anchors or transosseous sutures is required.
2. Chronic Instability Without Arthrosis (>4 Weeks)
When instability is diagnosed late but the articular cartilage remains pristine, primary repair is often impossible due to ligament retraction and scarring.
* Ligament Reconstruction: Utilizing tendon grafts (e.g., flexor carpi radialis or palmaris longus) to recreate the SLIL or LTIL.
* Capsular Imbrication and Capsulodesis: Procedures such as the dorsal capsulodesis (Blatt procedure) can be added to tether the distal pole of the scaphoid, limiting its abnormal palmar flexion.
* Limited Intercarpal Arthrodesis: Fusion of specific carpal joints (e.g., scaphotrapeziotrapezoid [STT] fusion or scaphocapitate fusion) to stabilize the kinematic chain while preserving some wrist motion.
3. Chronic Instability With Arthrosis or Fixed Deformity
If there is a fixed, irreducible carpal deformity, established arthrosis, intractable pain, or severe functional impairment, reconstructive ligament procedures will fail. Salvage operations are required to preserve functional motion and relieve pain:
* Excisional Arthroplasty: Proximal Row Carpectomy (PRC) involves excising the scaphoid, lunate, and triquetrum, allowing the capitate to articulate with the lunate fossa of the radius.
* Limited Intercarpal Arthrodesis: Four-corner fusion (capitate, hamate, lunate, triquetrum) with scaphoid excision is the standard for SLAC wrist.
* Total Wrist Fusion: The ultimate salvage procedure for pan-carpal arthritis, providing a stable, pain-free wrist at the expense of all radiocarpal and midcarpal motion.
SURGICAL APPROACHES TO THE WRIST
Achieving adequate exposure while preserving the vascular supply to the carpus is the cornerstone of wrist surgery. Depending on the injury pattern, a dorsal, palmar, or combined approach may be utilized.
The Dorsal Approach and Capsulotomy
The dorsal approach provides excellent visualization of the proximal carpal row, the midcarpal joint, and the intrinsic ligaments.
Positioning and Incision:
The patient is positioned supine with the arm on a hand table. A pneumatic tourniquet is applied. A longitudinal incision is made over the dorsal wrist, centered over Lister's tubercle. The extensor retinaculum is exposed and incised, typically through the third extensor compartment. The extensor pollicis longus (EPL) is transposed radially, and the tendons of the fourth compartment are retracted ulnarly.
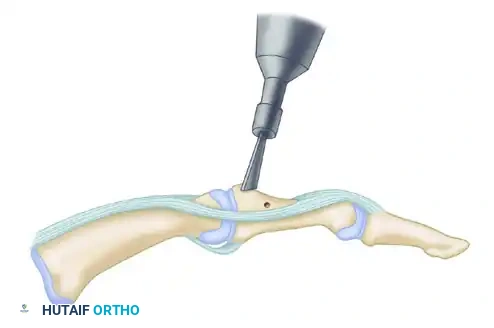
The Capsular Flap:
Preserving the dorsal capsular ligaments is critical to prevent iatrogenic instability. A highly effective technique is the creation of a radially based capsular flap.
Above: The intact dorsal ligamentous architecture of the wrist prior to capsulotomy, highlighting the complex interplay of the extrinsic stabilizers.
To expose the carpus while preserving capsular integrity for later repair, an alternative capsular incision is utilized. This flap is radially based, utilizing the interval between the dorsal intercarpal (DIC) ligament and the dorsal radiocarpal (DRC) ligament (also referred to anatomically as the dorsal radiotriquetral ligament).
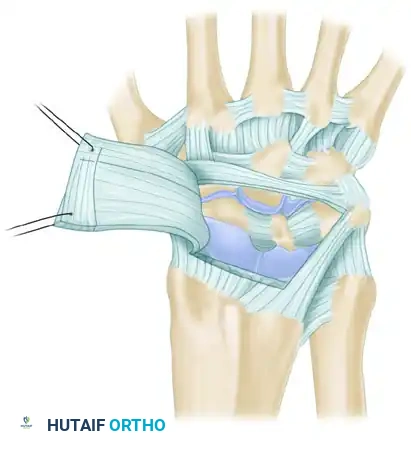
FIGURE 69-86: Alternative capsular incision, radially based between the dorsal intercarpal (DIC) ligament and the dorsal radiocarpal (DRC) ligament. C, capitate; DIC, dorsal intercarpal ligament; DRC, dorsal radiocarpal ligament; H, hamate; L, lunate; LT, Lister tubercle; S, scaphoid; T, triquetrum.
This ligament-sparing capsulotomy allows broad exposure of the scaphoid, lunate, and triquetrum. Geissler et al. emphasized the utility of this dorsal approach to meticulously clean out the space required to receive the lunate during the reduction of perilunate dislocations.
The Palmar Approach
A palmar approach is frequently recommended in conjunction with the dorsal approach, particularly in the setting of perilunate dislocations.
* Indications: The primary indication for the palmar approach is to decompress the median nerve (carpal tunnel release), which is often acutely compressed by the volarly dislocated lunate.
* Technique: An extended carpal tunnel incision is utilized. This approach also allows for the repair of the palmar extrinsic ligaments (e.g., the radioscaphocapitate ligament), which are critical for preventing palmar subluxation of the carpus.
Surgical Pitfall: Attempting to reduce a chronic or severely displaced perilunate dislocation from a dorsal approach alone can lead to excessive force and iatrogenic cartilage damage. A combined dorsal and palmar approach is often required to safely mobilize the carpus, decompress the median nerve, and achieve a tension-free anatomic reduction.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of wrist ligament repairs is as critical as the surgical execution.
- Immobilization Phase (0 to 8 Weeks):
- Following open repair or pinning, the wrist is immobilized in a bulky compressive dressing and a short-arm volar splint.
- At 10 to 14 days, sutures are removed, and the patient is transitioned to a rigid short-arm cast or a custom thermoplastic splint.
- K-wires used for intercarpal stabilization are typically left in place for 8 to 10 weeks to allow sufficient biological healing of the ligamentous tissues.
- Early Mobilization Phase (8 to 12 Weeks):
- Once pins are removed, active and active-assisted range of motion (ROM) exercises are initiated under the guidance of a certified hand therapist.
- Proprioceptive re-education (e.g., using a gyroscope or powerball) is critical to retrain the dynamic neuromuscular stabilizers of the wrist.
- Strengthening Phase (12+ Weeks):
- Progressive resistance exercises are introduced.
- Patients are cautioned that maximum medical improvement may take up to 12 months, and a mild permanent loss of terminal flexion and extension is a common and expected outcome following major carpal reconstruction.
CONCLUSION
The successful treatment of wrist ligament injuries and carpal instability relies on a high index of suspicion, precise diagnostic imaging, and a thorough understanding of carpal biomechanics. From the acute arthroscopic management of Geissler Grade II tears to the complex, combined open approaches required for perilunate dislocations, the orthopedic surgeon must employ a meticulous, tissue-respecting technique. By adhering to these evidence-based principles, surgeons can restore carpal stability, mitigate the progression of degenerative arthrosis, and optimize functional outcomes for their patients.
You Might Also Like