Operative Management of Bennett Fractures and Thumb CMC Joint Trauma

Key Takeaway
The thumb carpometacarpal joint is critical for hand function. Bennett fractures, characterized by intraarticular displacement of the first metacarpal base, compromise this stability. Deforming forces from the abductor pollicis longus necessitate precise reduction. While closed reduction and percutaneous pinning remain the gold standard for reducible fractures, open reduction is mandated for persistent articular incongruity exceeding 2 millimeters to prevent post-traumatic arthrosis and preserve pinch strength.
Anatomy and Biomechanics of the Thumb Carpometacarpal Joint
The integrity of the thumb carpometacarpal (CMC) or trapeziometacarpal joint is arguably more critical to the overall function of the hand than any other single articulation. Functioning as a highly mobile biconcave-biconvex saddle joint, it facilitates a complex range of motion, including flexion, extension, abduction, adduction, and the composite motion of opposition.
Stability of the thumb CMC joint relies heavily on its capsuloligamentous complex, most notably the anterior oblique ligament (AOL)—often referred to as the volar oblique ligament—and the dorsoradial ligament (DRL). The AOL originates from the palmar tubercle of the trapezium and inserts onto the volar-ulnar beak of the first metacarpal base, acting as the primary restraint against dorsal subluxation during pinch and grip activities.
Offset intraarticular fractures, persistent subluxation, or frank dislocation of this joint inevitably lead to a cascade of functional deficits. These include severe limitation of motion, chronic pain, and a profound weakness in both pinch and grip strength.
Clinical Pearl: Secondary metacarpophalangeal (MCP) hyperextension deformities frequently follow dorsal displacement of the thumb basal joint. This "zigzag" collapse occurs because the proximal migration of the metacarpal alters the resting tension of the extrinsic tendons, severely weakening pinch and grip strength. Reestablishing absolute stability and articular congruency to the trapeziometacarpal joint is paramount to restoring normal hand kinematics.
The Bennett Fracture: Pathoanatomy and Deforming Forces
In 1882, Edward Hallaran Bennett, an eminent Irish surgeon, first described the classic intraarticular fracture through the base of the first metacarpal. The Bennett fracture is fundamentally a two-part fracture-dislocation characterized by a highly predictable pattern of displacement driven by unopposed muscular forces.
The Deforming Muscular Forces
The pathoanatomy of a Bennett fracture is dictated by the following biomechanical forces:
* The Volar-Ulnar Fragment: The medial projection (volar beak) of the thumb metacarpal base remains anatomically reduced. It is held securely in place against the trapezium by the intact volar oblique ligament.
* The Metacarpal Shaft: The main shaft of the first metacarpal is displaced laterally, proximally, and dorsally by the robust, unopposed pull of the abductor pollicis longus (APL), which inserts at the dorsal-radial base of the metacarpal.
* Adductor Pollicis (AP): The adductor pollicis further exacerbates the deformity by pulling the distal metacarpal shaft into adduction and supination, pivoting the shaft around the intact volar fragment.
Understanding these deforming forces is critical, as any successful reduction maneuver must directly counteract the proximal, dorsal, and radial pull of the APL, as well as the adduction force of the AP.
Historical and Non-Operative Management Challenges
Historically, closed management of Bennett fractures was attempted using various traction and casting techniques. While reduction by longitudinal traction is relatively easy to achieve, it is notoriously difficult to maintain due to the persistent, dynamic pull of the extrinsic and intrinsic musculature.
- Traction Systems: The historical use of rubber band traction applied through a transverse pin placed in the proximal phalanx has proven to be undependable. It fails to adequately control the rotational and angular deforming forces acting on the metacarpal base.
- Casting Limitations: Immobilization via casting is frequently incomplete. Verification of precise articular alignment through an overlying plaster or fiberglass cast is radiographically challenging. Furthermore, attempting to maintain reduction by applying localized pressure over the base of the metacarpal is fraught with complications.
Surgical Warning: Utilizing a cast that relies on direct, localized pressure over the dorsal base of the first metacarpal to maintain reduction is highly unsatisfactory. Excessive pressure rapidly leads to skin necrosis over the bony prominence, while insufficient pressure inevitably allows for loss of reduction and subsequent malunion.
The Articular Incongruity Controversy
Considerable controversy surrounds the acceptable limits of articular displacement in Bennett fractures. While anatomical reduction is the universal goal, biomechanical and long-term clinical studies suggest that articular incongruity of 1 to 3 mm seems to be well tolerated, provided that solid bony union and absolute joint stability are achieved. However, persistent subluxation or step-offs greater than 2-3 mm significantly increase focal contact pressures, accelerating the onset of post-traumatic osteoarthritis.
Surgical Management: Closed Reduction and Percutaneous Pinning (CRPP)
For the majority of acute Bennett fractures, the technique of closed reduction and percutaneous pinning (CRPP), as popularized by Wagner, is the preferred and most widely utilized treatment modality.
The Reduction Maneuver
The reduction must systematically reverse the deforming forces:
1. Longitudinal Traction: Apply strong axial traction to the thumb to overcome the proximal pull of the APL.
2. Palmar Abduction: Bring the thumb into palmar abduction to correct the adduction deformity caused by the adductor pollicis.
3. Pronation: Pronate the metacarpal shaft to correct the supination deformity.
4. Direct Pressure: While maintaining the above positions, apply firm, direct pressure over the dorsal-radial aspect of the first metacarpal base, pushing it volarly and ulnarly to reduce the shaft to the captive volar-ulnar fragment.
Percutaneous Pinning Technique
Once reduction is confirmed via multi-planar fluoroscopy (including a true AP or Robert's view, and a true lateral of the CMC joint), fixation is achieved using smooth Kirschner wires (typically 0.045-inch or 0.062-inch).
- Trans-trapezial Fixation: The primary K-wire is driven from the dorsal-radial aspect of the first metacarpal base, across the CMC joint, and into the trapezium.
- Intermetacarpal Fixation: A second K-wire is often placed from the first metacarpal shaft into the second metacarpal to neutralize the adduction forces and provide rotational stability.
Surgical Management: Open Reduction and Internal Fixation (ORIF)
Should closed reduction prove unsatisfactory—leaving an articular step-off greater than 2 mm or persistent joint subluxation—open reduction is strictly indicated.
The Wagner Surgical Approach
- Incision: A curved or L-shaped incision is made along the glabrous border of the thenar eminence, curving dorsally over the CMC joint.
- Superficial Dissection: Meticulous care must be taken to identify and protect the sensory branches of the superficial radial nerve and the lateral antebrachial cutaneous nerve.
- Deep Dissection: The thenar musculature (abductor pollicis brevis and opponens pollicis) is elevated subperiosteally from the first metacarpal shaft and reflected volarly.
- Capsulotomy: A longitudinal or T-shaped capsulotomy of the CMC joint is performed to expose the articular surface and the fracture hematoma.
- Reduction and Fixation: The fracture site is debrided of hematoma and interposed tissue. The shaft is anatomically reduced to the volar-ulnar fragment using a pointed reduction forceps. Fixation is typically achieved using multiple parallel K-wires or, if the volar fragment is sufficiently large, a 1.5 mm or 2.0 mm mini-fragment lag screw.
Management of Complex Combined Hand Trauma
In high-energy crush injuries, a Bennett fracture may present as part of a broader spectrum of severe hand trauma, including multiple metacarpal fractures, severe soft tissue degloving, and muscle devitalization. In such catastrophic injuries, the principles of damage control orthopedics and meticulous soft tissue management take precedence.
Surgical debridement must be aggressive and thorough to prevent deep space infections and subsequent osteomyelitis.
Initial exposure of a complex dorsal hand injury requires wide extension of the surgical incisions to fully assess the zone of injury. Retractors are placed to evaluate the integrity of the extensor apparatus and the underlying intrinsic musculature.
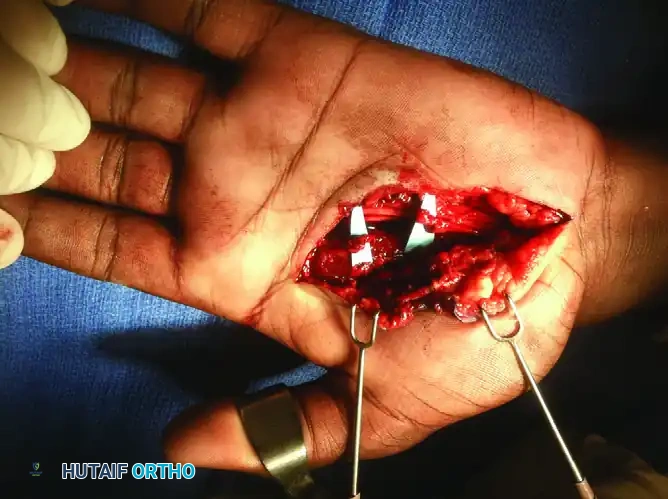
During the exploration of high-energy crush injuries, devitalized muscle tissue must be meticulously excised. The image above demonstrates the surgical débridement of devitalized second and third dorsal interossei. Failure to adequately debride necrotic intrinsic muscle bellies will lead to severe ischemic contractures (intrinsic plus hand) or catastrophic deep infections.
Once the soft tissue bed has been adequately debrided and stabilized, rigid skeletal fixation is applied. In complex, comminuted fractures where screw fixation is impossible, large Kirschner wires provide excellent, versatile stabilization.


The radiographs above demonstrate the final fixation of complex metacarpal trauma utilizing a large Kirschner wire. This intramedullary or trans-articular pinning technique maintains longitudinal alignment and prevents the collapse of the metacarpal arch while the severe soft tissue injury heals.
Postoperative Protocol and Rehabilitation
The postoperative management of Bennett fractures requires a delicate balance between protecting the articular reduction and preventing debilitating stiffness.
Immobilization Phase (Weeks 0-4)
- Immediately postoperatively, the patient is placed in a well-padded, rigid thumb spica splint.
- At 10 to 14 days, sutures are removed, and the patient is transitioned to a short-arm thumb spica cast. The interphalangeal (IP) joint of the thumb may be left free to prevent extensor tendon adhesions, provided the fracture pattern allows.
- Strict elevation and active range of motion of the uninvolved digits are encouraged to mitigate edema and complex regional pain syndrome (CRPS).
Pin Removal and Mobilization (Weeks 4-6)
- Radiographs are obtained at 4 to 6 weeks to assess for clinical and radiographic union.
- Once bridging callus is visualized and the fracture is non-tender, the percutaneous K-wires are removed in the clinic.
- A custom thermoplastic thumb spica splint is fabricated for use between exercise sessions and during sleep.
- Active range of motion (AROM) of the thumb CMC and MCP joints is initiated under the guidance of a certified hand therapist.
Strengthening Phase (Weeks 6-12)
- Passive range of motion (PROM) and gentle dynamic splinting are introduced if stiffness persists.
- Progressive strengthening, focusing on pinch and grip mechanics, begins at 8 weeks postoperatively.
- Return to heavy manual labor or contact sports is typically restricted until 10 to 12 weeks, ensuring complete consolidation of the fracture and maturation of the capsuloligamentous repair.
Complications and Pitfalls
Despite meticulous surgical technique, complications can arise in the management of Bennett fractures:
- Loss of Reduction: Most commonly occurs due to inadequate initial fixation (e.g., using pins that are too small) or failure to recognize the severity of the deforming forces. Frequent radiographic follow-up during the first 3 weeks is mandatory.
- Post-Traumatic Osteoarthritis: The most frequent long-term complication. While minor incongruities (1-3 mm) may be tolerated, significant step-offs lead to rapid cartilage wear. Symptomatic arthritis may eventually require salvage procedures such as trapeziometacarpal arthrodesis or ligament reconstruction and tendon interposition (LRTI).
- Pin Tract Infections: Superficial infections are common with percutaneous wires. They are generally managed successfully with oral antibiotics and local pin care. Deep infections requiring premature pin removal are rare but devastating.
- Sensory Nerve Injury: The superficial radial nerve is highly susceptible to injury during both percutaneous pinning and open approaches. Neuromas in this region are profoundly debilitating. Blunt dissection to the bone and the use of soft tissue protectors during drilling are essential preventative measures.
You Might Also Like


