Masterclass in Peroneal Tendon Surgery: Synovectomy, Repair, and Stabilization
Key Takeaway
Peroneal tendon pathology, including tenosynovitis, longitudinal tears, and subluxation, frequently requires surgical intervention when conservative measures fail. This comprehensive guide details the operative techniques for peroneal tendon synovectomy, primary repair of the peroneus brevis and longus, and stabilization via fibular groove deepening. Mastery of the superior peroneal retinaculum anatomy and sural nerve preservation is critical for restoring lateral hindfoot biomechanics and ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Peroneal tendon disorders encompass a complex and highly variable spectrum of pathologies that range from acute, inflammatory tenosynovitis to chronic, degenerative tendinosis, longitudinal interstitial tearing, and frank, recurrent subluxation. Because the peroneus brevis and peroneus longus tendons share a common synovial sheath as they pass posterior to the lateral malleolus, inflammatory and mechanical conditions frequently affect both structures simultaneously. Historically underdiagnosed, peroneal tendon pathology is now recognized as a primary generator of posterolateral ankle pain, particularly in the athletic population and those with chronic lateral ankle instability. The intimate relationship of these tendons with the osseous morphology of the fibula and the restraining soft tissues dictates their susceptibility to injury.

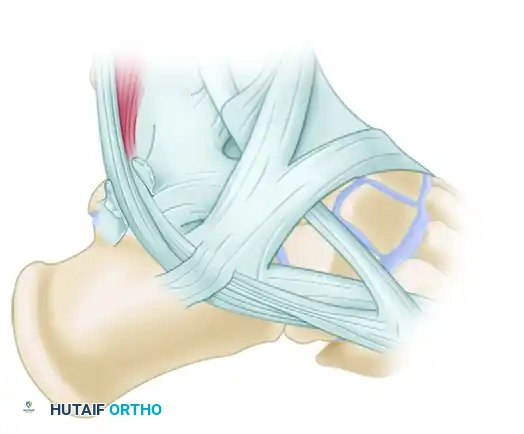
The retromalleolar groove of the distal fibula serves as a critical anatomical pulley, altering the vector of the peroneal muscle-tendon units to facilitate effective hindfoot eversion and plantarflexion of the first ray. The peroneus brevis lies anterior and medial within this groove, directly against the fibular sulcus. This anatomic positioning makes the peroneus brevis highly susceptible to mechanical attrition, particularly when the superior peroneal retinaculum (SPR) is incompetent, or when the fibular groove presents with a morphologically shallow or convex architecture. The "nutcracker effect," wherein the robust peroneus longus tendon compresses the underlying peroneus brevis against the sharp posterior ridge of the fibula during forced dorsiflexion, is a primary biomechanical driver of longitudinal split tears.
Epidemiologically, peroneal tendon pathology frequently presents concomitantly with chronic lateral ankle instability. Recurrent inversion injuries stretch and attenuate the lateral ligamentous complex, particularly the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (CFL). As the primary dynamic stabilizers of the lateral ankle, the peroneal tendons are subjected to exponentially increased eccentric loads to compensate for this static ligamentous incompetence. Over time, this compensatory overload leads to tenosynovitis, microvascular compromise, and eventual macroscopic tearing. Furthermore, acute traumatic events, such as forced dorsiflexion of an inverted foot—commonly seen in skiing, football, and gymnastics—can cause acute avulsion of the SPR, leading to immediate and debilitating subluxation.
Surgical intervention is definitively indicated when exhaustive conservative management fails to relieve symptoms. Conservative protocols typically involve a combination of rigid immobilization, targeted nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections (used with extreme caution to avoid tendon rupture), and structured physical therapy focusing on eccentric strengthening and proprioceptive recovery. However, in the presence of acute high-grade tears, significant retromalleolar crowding, or chronic structural instability, surgical reconstruction becomes mandatory. This masterclass details the comprehensive surgical management of peroneal tendon pathology, providing an exhaustive guide to tenosynovectomy, primary repair, side-to-side tenodesis, and fibular groove deepening.
Detailed Surgical Anatomy and Biomechanics
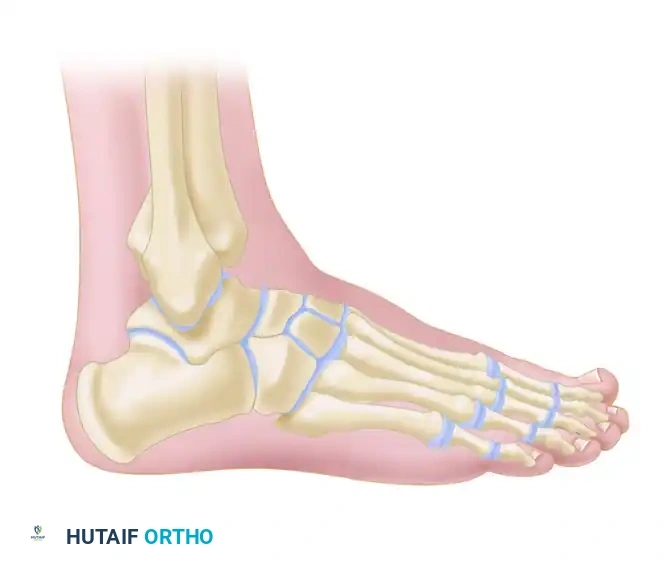
A profound, three-dimensional understanding of the lateral ankle anatomy is an absolute prerequisite for safe surgical exposure, accurate diagnosis of intraoperative pathology, and precise biomechanical restoration. The lateral compartment of the leg, bounded by the anterior and posterior intermuscular septa, houses the primary evertors of the foot.
Osteology and the Retromalleolar Groove
The osseous architecture of the posterolateral distal fibula is the foundational element of peroneal tendon stability. The retromalleolar groove is bounded laterally by a prominent fibrocartilaginous ridge, which serves as the primary attachment site for the superior peroneal retinaculum. Morphological cadaveric and advanced imaging studies have demonstrated significant variability in the shape of this groove. Approximately 82% of the population possesses a concave groove, 11% have a flat groove, and 7% exhibit a convex morphology. Patients with flat or convex grooves are at a significantly elevated risk for recurrent peroneal tendon subluxation, as the osseous constraint is fundamentally compromised.
Distal to the fibula, the lateral wall of the calcaneus provides further anatomical guidance. The peroneal tubercle, located on the lateral calcaneal surface, separates the peroneus brevis (which courses superior to the tubercle) from the peroneus longus (which courses inferiorly). Hypertrophy of the peroneal tubercle can lead to localized stenosis, causing tenosynovitis and attritional tearing of either tendon. Additionally, the presence of an os peroneum, a sesamoid bone located within the substance of the peroneus longus tendon at the level of the calcaneocuboid joint, can be a source of localized pathology, including painful os peroneum syndrome (POPS) and acute ruptures.
Myotendinous Architecture and Variants
The peroneus brevis (PB) originates from the distal two-thirds of the lateral fibular shaft and the adjacent intermuscular septa. Its muscle belly extends distally, often continuing into the retromalleolar groove before transitioning entirely into a tendinous structure, which inserts onto the tuberosity of the base of the fifth metatarsal. The peroneus longus (PL) originates more proximally from the head and proximal two-thirds of the lateral fibula. It runs posterior and lateral to the brevis in the retromalleolar groove, traverses the cuboid tunnel on the plantar aspect of the foot, and inserts on the plantar-lateral aspect of the base of the first metatarsal and the medial cuneiform.
Anomalous myotendinous anatomy is a frequent, yet often overlooked, contributor to peroneal pathology. The presence of a peroneus quartus muscle—reported in 10% to 22% of cadaveric specimens—or an abnormally low-lying muscle belly of the peroneus brevis crowds the fibro-osseous tunnel. This crowding exponentially increases intrasheath pressure during active muscle contraction, precipitating ischemic tenosynovitis, longitudinal fissuring of the peroneus brevis, and eventual subluxation. The operating surgeon must routinely inspect the proximal extent of the tendon sheath during exploration to identify and excise these space-occupying variants.
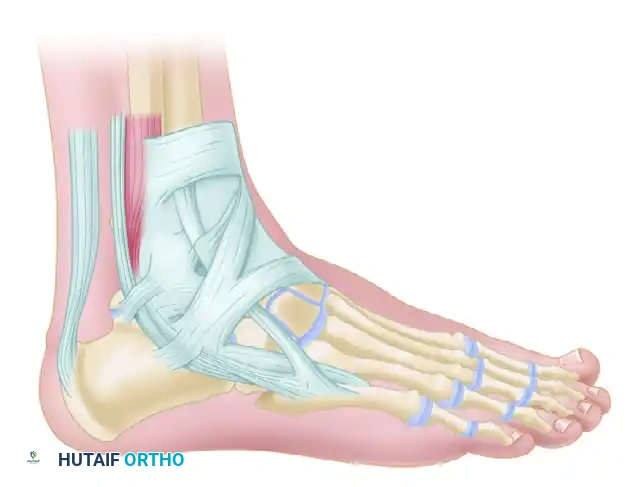
The Retinacular System
The superior peroneal retinaculum (SPR) is the primary static restraint against anterior subluxation of the peroneal tendons. It is a distinct thickening of the superficial aponeurosis of the leg, originating from the posterolateral ridge of the distal fibula and inserting onto the lateral wall of the calcaneus and the Achilles tendon sheath. The SPR functions in concert with the calcaneofibular ligament (CFL), which lies deep to the peroneal tendons, forming the floor of the peroneal tendon sheath.

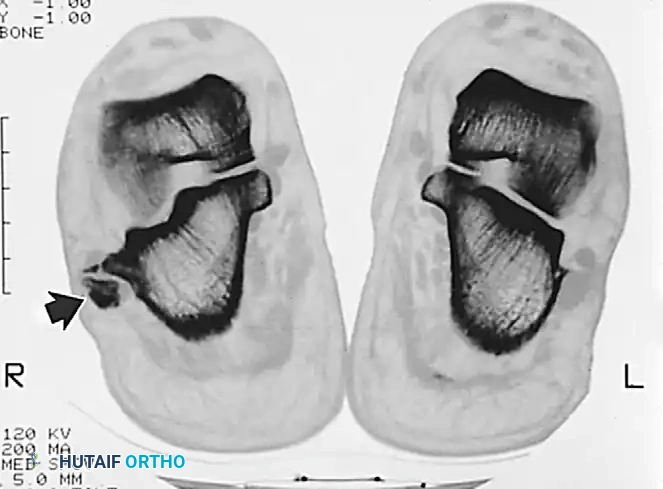
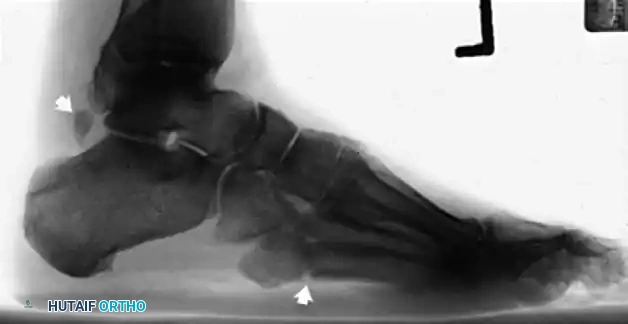
Pathology of the SPR is classified into four distinct grades based on the Eckert and Davis classification, later modified by Oden. Grade I involves the SPR elevating from the fibrocartilaginous ridge with the periosteum. Grade II involves a tear of the fibrocartilaginous ridge itself. Grade III represents a cortical avulsion fracture from the posterolateral fibula (the "fleck sign"). Grade IV, the Oden modification, involves a tear of the SPR from its posterior attachment on the deep fascia. Accurate identification of the specific SPR injury pattern is crucial for determining the appropriate method of retinacular reconstruction.
Neurovascular Considerations
The vascular supply to the peroneal tendons is segmental, supplied primarily by branches of the peroneal and anterior tibial arteries. Injection studies have identified a critical avascular watershed zone within the peroneus brevis tendon, typically located 1 to 2 centimeters proximal to the tip of the lateral malleolus. This zone of relative ischemia corresponds precisely to the most common site of longitudinal split tears and degenerative tendinosis, underscoring the role of vascular compromise in the pathogenesis of tendon failure. The mesotenon, carrying these delicate vessels, enters the tendons from the posterior aspect of the sheath and must be meticulously preserved during synovectomy.
The sural nerve presents the most significant neurological hazard during lateral ankle surgery. It courses distally along the posterolateral aspect of the calf, running in close proximity to the small saphenous vein. As it approaches the lateral malleolus, it typically divides into the lateral dorsal cutaneous nerve and lateral calcaneal branches, providing critical sensation to the lateral hindfoot and midfoot. The nerve is highly vulnerable to iatrogenic transection, traction injury, or entrapment within postoperative scar tissue. Meticulous blunt dissection in the subcutaneous tissues and careful retraction are imperative to prevent debilitating postoperative neuromas.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for peroneal tendon pathology must be based on a comprehensive clinical assessment, advanced imaging correlation, and the exhaustion of non-operative modalities. Surgical indications are stratified based on the chronicity of the symptoms, the structural integrity of the tendons, and the stability of the superior peroneal retinaculum.
Primary indications for surgical intervention include acute, high-grade traumatic tears of the peroneus brevis or longus, and acute avulsions of the SPR presenting with frank, irreducible subluxation. In the chronic setting, indications encompass persistent tenosynovitis that has remained refractory to a minimum of 3 to 6 months of conservative management, including immobilization in a CAM boot, physical therapy, and NSAID therapy. Furthermore, symptomatic longitudinal split tears, chronic recurrent subluxation, and painful os peroneum syndrome with associated peroneus longus tearing are definitive indications for operative management.
Contraindications to peroneal tendon surgery must be rigorously respected to avoid catastrophic postoperative complications. Absolute contraindications include active local or systemic infection, severe peripheral vascular disease precluding adequate wound healing, and profound peripheral neuropathy (such as advanced Charcot neuroarthropathy) where the patient lacks protective sensation and cannot comply with strict postoperative non-weight-bearing protocols. Relative contraindications include poorly controlled diabetes mellitus, heavy tobacco use, and significant psychiatric or cognitive disorders that impede rehabilitation compliance.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Tenosynovectomy | Refractory tenosynovitis > 3 months; Hypertrophic synovium on MRI; Intact tendon substance. | Active local infection; Severe peripheral arterial disease. | Uncontrolled diabetes; Active smoking. |
| Primary Tendon Repair | Longitudinal split tears involving < 50% of the tendon cross-sectional area; Acute lacerations. | Tendon defect > 50% cross-sectional area; Severe degenerative tendinosis. | Chronic corticosteroid use; Advanced age with low demand. |
| Tenodesis (Side-to-Side) | Tears or degeneration involving > 50% of the tendon; Non-viable tendon segments requiring excision. | Both PB and PL tendons severely degenerated/non-viable (requires allograft). | Severe hindfoot varus (must be corrected concurrently). |
| Fibular Groove Deepening | Recurrent peroneal subluxation; Convex/flat fibular groove morphology; Failed conservative casting. | Open physes (pediatric patients - modifies technique); Local osteomyelitis. | Inadequate soft tissue envelope for closure. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential for anticipating intraoperative challenges and ensuring the availability of appropriate surgical equipment, including high-speed burrs, suture anchors, and potential allograft tissues. The clinical evaluation and imaging review form the cornerstone of this preparatory phase.
Clinical Evaluation and Diagnostic Imaging
Patients typically present with localized posterolateral ankle pain, swelling along the tendon sheath, and a sensation of weakness or "giving way." In cases of subluxation, patients may report a palpable or audible "snap" during resisted eversion and dorsiflexion from an inverted position. The physical examination must include a thorough assessment of hindfoot alignment, as a rigid varus hindfoot will place excessive stress on any lateral soft tissue repair, inevitably leading to failure if not addressed concurrently with a calcaneal osteotomy.
Imaging begins with weight-bearing plain radiographs of the ankle and foot. Anteroposterior, lateral, and mortise views are scrutinized for the "fleck sign" (indicating an avulsion fracture of the SPR from the lateral fibula), hypertrophy of the peroneal tubercle, or degenerative changes at the calcaneocuboid joint. Radiographs also assist in evaluating overall foot morphotype and lateral column alignment.


Magnetic Resonance Imaging (MRI) is the gold standard for evaluating tendon integrity, the extent of fluid within the tendon sheath, and the osseous morphology of the retromalleolar groove. Axial T2-weighted fat-suppressed sequences are particularly critical for identifying the classic "C-sign" or "boomerang" shape of a flattened peroneus brevis tendon, which precedes frank longitudinal fissuring. The surgeon must be cautious of the "magic angle" artifact, which occurs when the tendon courses at a 55-degree angle to the main magnetic field, artificially increasing signal intensity and mimicking tendinosis.

Anesthesia and Patient Positioning
The procedure is typically performed under general anesthesia or regional anesthesia, supplemented with a popliteal sciatic nerve block for extended postoperative analgesia. The choice of anesthesia must be discussed with the patient, taking into consideration their cardiopulmonary status and the anticipated duration of the surgery. A well-placed popliteal block significantly reduces the need for postoperative opioids and facilitates early discharge in the ambulatory setting.
Patient positioning is critical for optimal surgical access. The patient is most commonly placed in the lateral decubitus position, heavily padded at all bony prominences, with an axillary roll in place. Alternatively, the patient can be placed supine with a large bump under the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus into a direct anterior-facing orientation. A thigh or proximal calf tourniquet is applied over generous padding. After sterile preparation and draping, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to standard pressures (typically 250-300 mmHg) to ensure a bloodless surgical field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires meticulous soft tissue handling, precise osteocartilaginous manipulation, and robust biomechanical reconstruction of the retinacular restraints. The sequence of steps must be strictly adhered to in order to minimize iatrogenic morbidity.
Surgical Incision and Superficial Dissection
The surgical approach utilizes a curvilinear incision that meticulously follows the anatomical course of the peroneal tendons. The incision begins 3 to 4 centimeters proximal to the tip of the lateral malleolus, extending distally along the posterior border of the fibula, and curves gently anteriorly toward the base of the fifth metatarsal. This specific trajectory provides comprehensive access to the retromalleolar groove, the peroneal tubercle, and the distal insertions.


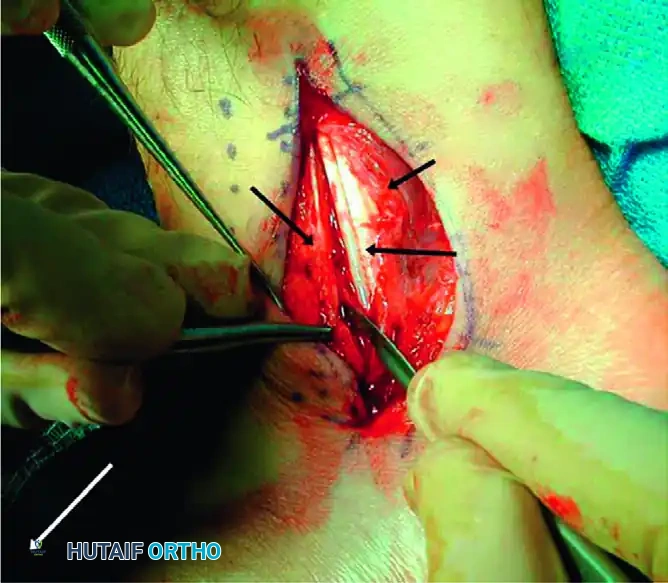
Deepening the incision through the subcutaneous tissue requires extreme vigilance. The sural nerve and the short saphenous vein lie immediately deep to the superficial fascia and often cross the surgical field. Meticulous blunt dissection using a hemostat or surgical scissors is employed to identify these structures. Once identified, the neurovascular bundle is gently mobilized and protected with a vessel loop or a blunt retractor. Dissection continues deep to the subcutaneous fat to expose the glistening white fibers of the superior peroneal retinaculum (SPR).

Retinaculum Incision and Tenosynovectomy
The superior peroneal retinaculum is incised longitudinally. It is of paramount importance to leave a 1- to 2-millimeter cuff of retinacular tissue attached to the posterior border of the fibula. This cuff serves as a vital anchor point for the subsequent repair and imbrication of the SPR at the conclusion of the procedure. Once the retinaculum is opened, the common peroneal tendon sheath is exposed.
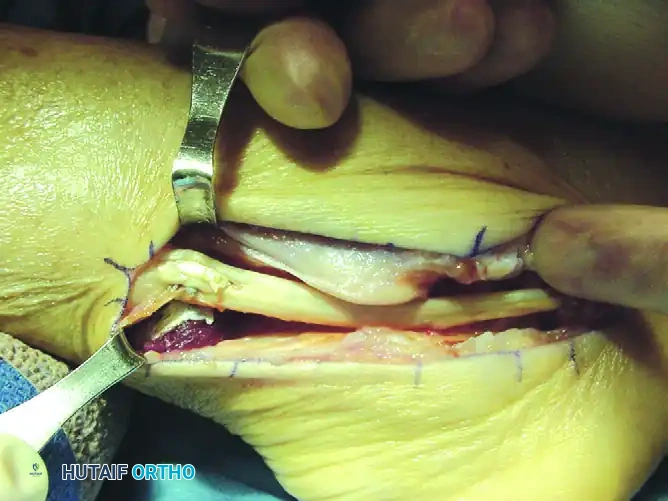
In cases of chronic tenosynovitis, hypertrophic, highly vascularized, and inflamed synovium will be immediately evident, often obscuring the underlying tendons. A meticulous tenosynovectomy is performed using a combination of sharp dissection and rongeurs to excise all pathological inflammatory tissue. During this debridement, the surgeon must exercise extreme caution to preserve the mesotenon—the delicate vascular tether located on the deep, posterior aspect of the tendons—to prevent devascularization and subsequent ischemic necrosis of the tendon substance.
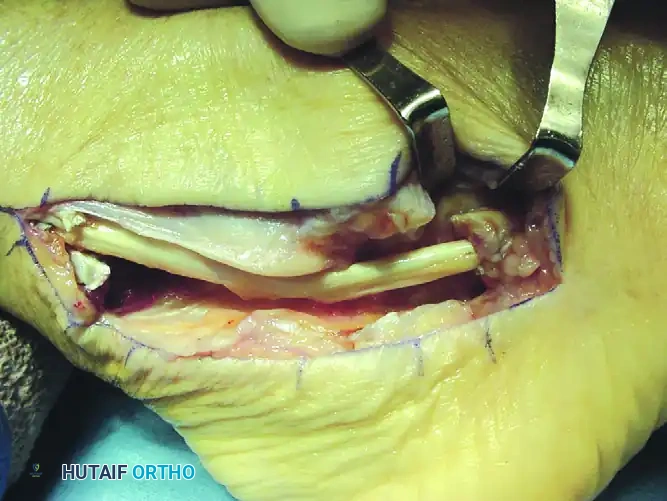
Tendon Inspection, Debridement, and Primary Repair
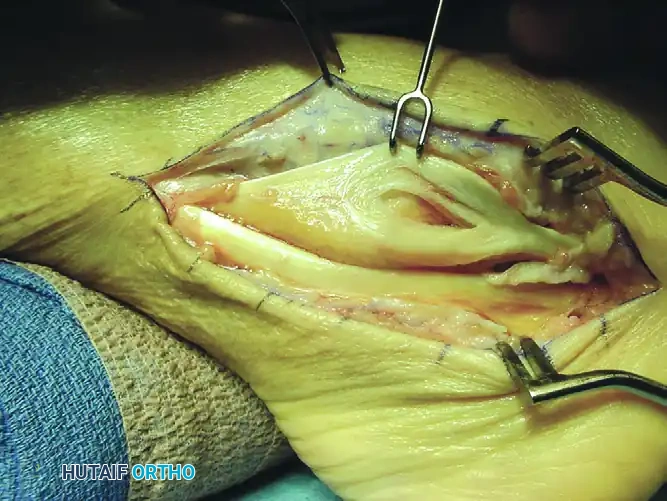
Once the synovectomy is complete, both the peroneus brevis and peroneus longus tendons are delivered from the wound using blunt retractors or Penrose drains. The tendons are systematically inspected along their entire length for areas of attenuation, degenerative nodularity, and longitudinal fissuring. The peroneus brevis is most commonly affected, presenting with a longitudinal split tear caused by the mechanical compression of the peroneus longus against the fibula.
The surgical management of the tendon tear is dictated by the cross-sectional area of involvement. For longitudinal split tears involving less than 50% of the tendon's cross-sectional area, the degenerative, frayed margins of the split are sharply excised. The remaining healthy tendon is then tubularized. This is achieved using a running 2-0 or 3-0 nonabsorbable braided suture (such as Ethibond or FiberWire). The knots must be meticulously buried within the tendon substance to minimize friction and prevent postoperative adhesions within the tendon sheath.
For severe tears or advanced tendinosis involving greater than 50% of the cross-sectional area, the remaining tendon tissue is deemed non-viable and mechanically insufficient. The diseased segment of the peroneus brevis is excised completely. A side-to-side tenodesis of the proximal and distal stumps of the peroneus brevis to the adjacent, intact peroneus longus tendon is then performed. This is executed using interrupted 2-0 nonabsorbable sutures. Crucially, during the tenodesis, the foot must be held in neutral dorsiflexion and slight eversion to establish the correct resting tension of the musculotendinous units, ensuring optimal postoperative biomechanics.
Fibular Groove Deepening and Retinacular Reconstruction
In the presence of chronic peroneal subluxation or a demonstrably shallow fibular groove, osseous reconstruction is required. The osteocartilaginous flap technique is the gold standard, as it deepens the sulcus while preserving the smooth, gliding cartilaginous surface essential for tendon function. The peroneal tendons are retracted anteriorly to fully expose the posterior aspect of the distal fibula.
Using a sharp scalpel or a very fine, thin osteotome, a rectangular osteocartilaginous flap is created. The cartilaginous surface of the sulcus is carefully elevated from its lateral margin, hinging it delicately on its medial periosteal attachment. The flap is elevated out of its bed for a total length of approximately 1.5 to 2.0 centimeters, exposing the underlying cancellous bone of the distal fibula.
Once the flap is elevated, a high-speed burr, curette, or small gouge is utilized to excavate the underlying cancellous bone. The goal is to create a rectangular trough to a depth of 4 to 5 millimeters. The surgeon must be careful not to breach the anterior cortex of the fibula during this excavation.
After the trough is adequately prepared, the osteocartilaginous flap is gently tamped back into the deepened groove using a broad, flat impactor. The flap should sit flush, creating a deep, concave sulcus that will physically contain the tendons. Bone wax is applied generously to any exposed cancellous bone edges at the periphery of the flap to prevent hematoma formation and subsequent postoperative adhesions between the raw bone and the healing tendons.
The peroneus longus and brevis tendons are then relocated into the newly deepened retromalleolar groove. The posterior flap of the SPR is drawn over the tendons. To promote biological healing, the posterolateral ridge of the fibula is roughened with a small rasp. The SPR is then tightly imbricated and sutured to the fibular ridge or the preserved retinacular cuff using 2-0 nonabsorbable sutures. If the native tissue cuff is insufficient, small suture anchors (typically 2.4mm or 2.9mm) are placed into the posterolateral fibula to achieve a robust, mechanical repair of the retinaculum. The stability of the construct is verified by taking the ankle through a full range of motion,
Clinical & Radiographic Imaging Archive

