Comprehensive Introduction and Patho-Epidemiology
Injuries to the flexor tendons of the foot and ankle, specifically encompassing the flexor hallucis longus (FHL) and the peroneal tendon complex, represent a challenging spectrum of pathologies that demand a high index of clinical suspicion and a profound understanding of hindfoot biomechanics. Historically, these entities were frequently overshadowed by the more ubiquitous Achilles tendinopathy or posterior tibial tendon dysfunction. However, contemporary orthopedic literature and advanced imaging modalities have illuminated the significant morbidity associated with FHL and peroneal disorders. These conditions are no longer relegated to the realm of niche sports medicine but are increasingly recognized as primary sources of debilitating posteromedial and lateral hindfoot pain in both athletic and general populations.
The patho-epidemiology of flexor hallucis longus tendinitis is classically associated with classical ballet dancers, gymnasts, and athletes whose disciplines require repetitive, explosive forefoot push-off and extreme plantar flexion, often referred to as the en pointe or demi-pointe positions. This repetitive mechanical loading forces the FHL tendon to glide under immense tension through its constrained fibro-osseous tunnel posterior to the talus. Over time, this mechanical attrition results in tenosynovitis, nodular hypertrophy, and eventual stenosis, creating a functional tethering of the tendon. While "dancer's tendinitis" remains a prevalent moniker, modern epidemiological studies indicate that FHL tendinopathy frequently occurs in non-athletic populations, often secondary to subtle biomechanical malalignments, such as hindfoot valgus or unrecognized posterior ankle impingement syndromes involving an os trigonum or an elongated Stieda process.
Conversely, the peroneal tendons—comprising the peroneus brevis and peroneus longus—are the primary dynamic stabilizers of the lateral ankle and the primary evertors of the foot. Pathologies here typically arise in the setting of chronic lateral ankle instability, acute inversion injuries, or anatomical variants that predispose the tendons to mechanical wear. Longitudinal split tears of the peroneus brevis are particularly common, driven by the "bowstringing" effect where the tendon is compressed between the unyielding posterior fibula and the overlying, more robust peroneus longus tendon during repetitive dorsiflexion and eversion. Epidemiologically, peroneal tendon tears are found in up to 30% of patients undergoing surgical stabilization for chronic lateral ankle instability, highlighting the critical need for comprehensive lateral compartment evaluation in these patients.
Understanding the demographic distribution and the mechanical etiology of these injuries is paramount for the orthopedic surgeon. The transition from acute tenosynovitis to chronic tendinosis, and ultimately to structural failure (tears or ruptures), dictates the therapeutic algorithm. Early recognition can often allow for successful non-operative management, whereas delayed diagnosis typically necessitates complex surgical reconstruction, tendon transfers, or tenodesis to restore the intricate biomechanical balance of the foot and ankle.
Detailed Surgical Anatomy and Biomechanics
Flexor Hallucis Longus Anatomy and Kinematics
The flexor hallucis longus muscle originates from the inferior two-thirds of the posterior aspect of the fibula, the lower interosseous membrane, and the transverse intermuscular septum. Its muscle belly extends notably distal, often reaching the level of the tibiotalar joint, a critical anatomical feature that can contribute to volume-related impingement within the posterior ankle compartment. As the FHL transitions into its tendinous portion, it enters a highly constrained fibro-osseous tunnel. The anterior border of this tunnel is formed by the posterior aspect of the talus, specifically nestled between the medial and lateral tubercles. The posterior border is formed by the robust flexor retinaculum.
Distal to the talar tunnel, the FHL courses beneath the sustentaculum tali of the calcaneus, utilizing it as a fulcrum to redirect its vector of pull. It then advances into the plantar aspect of the midfoot, where it crosses dorsal to the flexor digitorum longus (FDL) tendon at the anatomical landmark known as the knot of Henry. At this juncture, there are highly variable tendinous slips connecting the FHL and FDL, which have significant implications for tendon harvesting and functional deficits post-transfer. The FHL finally courses between the two sesamoids of the first metatarsophalangeal (MTP) joint to insert onto the base of the distal phalanx of the hallux. Biomechanically, the FHL is the primary flexor of the interphalangeal joint of the great toe and acts as a vital secondary plantar flexor of the ankle. During the terminal stance phase of the gait cycle, the FHL stabilizes the medial longitudinal arch and provides the critical propulsive force required for toe-off.
Peroneal Tendon Complex Anatomy
The lateral compartment of the leg houses the peroneus longus and peroneus brevis muscles. The peroneus brevis originates from the distal two-thirds of the lateral fibular shaft and the adjacent intermuscular septa. Its tendon forms proximal to the lateral malleolus and lies directly against the posterior fibular groove. The peroneus longus originates more proximally from the head and proximal two-thirds of the lateral fibula. Its tendon courses superficial and posterior to the peroneus brevis. Both tendons share a common synovial sheath as they pass posterior to the lateral malleolus, tightly constrained within the retromalleolar groove by the superior peroneal retinaculum (SPR).
The morphology of the retromalleolar fibular groove is highly variable and clinically significant. Cadaveric studies demonstrate that the groove is concave in approximately 82% of individuals, flat in 11%, and convex in 7%. A flat or convex groove drastically reduces the osseous constraint, placing excessive reliance on the SPR and predisposing the patient to peroneal tendon subluxation and subsequent longitudinal split tears. Distal to the fibula, the tendons separate at the peroneal tubercle of the calcaneus, constrained by the inferior peroneal retinaculum. The peroneus brevis inserts onto the styloid process (base) of the fifth metatarsal. The peroneus longus, however, dives sharply into the cuboid groove, traversing the plantar aspect of the foot to insert onto the plantar-lateral aspect of the medial cuneiform and the base of the first metatarsal.
Vascularity and Zones of Hypovascularity
The vascular supply to the flexor and peroneal tendons is a critical determinant of their healing capacity and susceptibility to degeneration. Injection studies have demonstrated distinct zones of relative hypovascularity in both tendon groups. For the FHL, a watershed zone exists within the fibro-osseous tunnel posterior to the talus, corresponding precisely to the most common site of nodular tendinosis and rupture.
Similarly, the peroneal tendons exhibit areas of diminished vascularity. The peroneus brevis has a hypovascular zone as it curves around the lateral malleolus, extending approximately 2 to 3 centimeters proximal to the tip of the fibula. The peroneus longus possesses two distinct watershed zones: one at the level of the lateral malleolus and another as it acutely changes direction at the cuboid notch. These avascular regions are mechanically stressed during physiological loading, creating a perfect storm for degenerative microtrauma, impaired healing, and eventual structural failure that necessitates surgical intervention.
Exhaustive Indications and Contraindications
The decision to proceed with operative management for flexor and peroneal tendon pathologies must be meticulously individualized, balancing the patient's functional demands, the duration of symptoms, and the structural integrity of the tendons as assessed by advanced imaging. Surgical intervention is rarely indicated as a first-line treatment, except in cases of acute traumatic dislocation with massive retinacular avulsion or acute complete tendon ruptures in high-level athletes.
For FHL tendinitis and posterior impingement, the primary indication for surgery is recalcitrant posteromedial ankle pain and functional limitation that has failed a comprehensive non-operative regimen for a minimum of 3 to 6 months. This regimen must include strict activity modification, immobilization in a CAM boot, targeted physical therapy focusing on eccentric stretching, and judicious corticosteroid injections into the tendon sheath (strictly avoiding intratendinous administration). When conservative measures fail, and clinical examination combined with MRI confirms stenosing tenosynovitis, nodular FHL thickening, or a symptomatic os trigonum causing mechanical tethering, operative decompression and synovectomy are highly indicated.
In the lateral compartment, indications for peroneal tendon surgery include symptomatic longitudinal split tears of the peroneus brevis or longus, chronic tendon subluxation or dislocation secondary to superior peroneal retinaculum incompetence, and severe stenosing tenosynovitis that limits active eversion and causes lateral retromalleolar pain. Furthermore, the presence of an enlarged peroneal tubercle or a symptomatic os peroneum with associated peroneus longus tearing warrants surgical exploration and debridement. If intraoperative assessment reveals that less than 50% of the tendon's cross-sectional area is viable, primary repair is contraindicated, and tenodesis or tendon transfer must be performed.
Contraindications to surgical intervention include active localized or systemic infection, severe peripheral arterial disease (PAD) that would preclude wound healing, and profound medical comorbidities that make anesthesia unacceptably risky. Relative contraindications encompass poorly controlled diabetes mellitus, active heavy smoking, and patient non-compliance, as the postoperative rehabilitation protocol is rigorous and essential for a successful outcome. Additionally, asymptomatic anatomical variants, such as an incidental os trigonum or a flat retromalleolar groove discovered on imaging for unrelated issues, should never be treated prophylactically.
| Pathology | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| FHL Tendinopathy / Impingement | Failure of 3-6 months conservative care; Symptomatic os trigonum with FHL tethering; Nodular stenosis limiting hallux ROM (positive stretch test). | Active hindfoot infection; Critical limb ischemia; Asymptomatic os trigonum. | Poorly controlled diabetes; Heavy tobacco use; Inability to comply with NWB protocols. |
| Peroneal Tendon Tears | Symptomatic split tears failing PT/bracing; Chronic subluxation/dislocation; >50% cross-sectional tearing requiring tenodesis. | Active lateral ankle infection; Severe vascular compromise; Complete lack of evertor muscle excursion/fatty atrophy. | Concomitant unaddressed severe cavovarus deformity (must be corrected concurrently); Non-compliant patient. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Clinical Evaluation
Pre-operative planning begins with a meticulous clinical examination to differentiate isolated tendinopathy from complex regional syndromes. For FHL pathology, the surgeon must perform the FHL stretch test. With the ankle held in maximal dorsiflexion to tension the FHL across the posterior ankle, the first MTP joint is passively dorsiflexed. A positive test is noted if MTP dorsiflexion is significantly restricted or elicits sharp pain in the posteromedial ankle compared to when the ankle is plantarflexed. Palpation must be precise, differentiating FHL tenderness (deep, posterior to the medial malleolus) from posterior tibial tendon tenderness (superficial, directly on the medial malleolus and navicular insertion).
For the peroneal tendons, provocative testing for subluxation is mandatory. The patient is asked to actively dorsiflex and evert the foot against resistance while the surgeon palpates the retromalleolar groove. A palpable or audible "snap" indicates SPR incompetence. Furthermore, the surgeon must evaluate the overall alignment of the foot and ankle. A subtle, uncorrected cavovarus deformity will continuously overload the lateral compartment; failure to address this osseous malalignment concurrently (e.g., via a lateralizing calcaneal osteotomy or dorsiflexing first metatarsal osteotomy) will inevitably lead to failure of the peroneal tendon repair.
Advanced Imaging Modalities
Imaging is critical for surgical templating. Weight-bearing orthogonal radiographs of the foot and ankle are the first-line modality to assess for an os trigonum, an elongated lateral talar process, os peroneum, or underlying structural deformities (varus/valgus). Ultrasound is highly valuable as a dynamic, real-time assessment tool. It allows the surgeon to visualize FHL excursion during hallux motion and can definitively capture transient peroneal tendon subluxation that might be missed on static imaging.
Magnetic Resonance Imaging (MRI) remains the gold standard for soft tissue evaluation. T2-weighted axial and sagittal sequences are scrutinized for fluid within the tendon sheaths (tenosynovitis), tendon hypertrophy, interstitial tearing, and the presence of low-lying muscle bellies. However, the surgeon must be acutely aware of the "magic angle" artifact. Because the peroneal tendons curve around the lateral malleolus at approximately 55 degrees to the main magnetic field, artificially increased signal intensity can mimic tendinosis or partial tearing on short TE sequences (T1 or PD). Therefore, intraoperative findings frequently dictate the final surgical procedure, and the surgeon must be prepared for extensive debridement or tenodesis regardless of the MRI report.
Patient Positioning and Operating Room Setup
Proper patient positioning is essential for adequate exposure and access. For isolated FHL decompression via a medial approach, the patient is placed supine with a bump under the contralateral hip to externally rotate the operative leg, providing excellent access to the posteromedial ankle. If an endoscopic posterior approach or a posterolateral open approach is chosen for combined os trigonum excision and FHL release, the patient is positioned prone.
For peroneal tendon reconstruction, the patient is placed in the lateral decubitus position. A beanbag is utilized to secure the patient, ensuring the operative leg is uppermost and parallel to the floor. All bony prominences are meticulously padded. A well-padded pneumatic thigh tourniquet is applied to provide a bloodless surgical field. The fluoroscopy unit (C-arm) should be positioned to enter from the anterior aspect of the patient, allowing for unhindered intraoperative orthogonal imaging, particularly if concurrent osseous procedures (e.g., groove deepening or osteotomies) are planned.
Step-by-Step Surgical Approach and Fixation Technique
FHL Decompression and Os Trigonum Excision
When addressing FHL stenosis and posterior impingement, the posterior endoscopic approach has gained significant popularity due to decreased morbidity and faster recovery. With the patient prone, posteromedial and posterolateral portals are established adjacent to the Achilles tendon. The crural fascia is incised, and the posterior ankle compartment is accessed. The FHL tendon is identified by its characteristic dynamic motion when the hallux is flexed. The fibro-osseous tunnel is carefully released using arthroscopic scissors or a retrograde knife. If an os trigonum is present, it is sharply dissected from its capsular attachments and excised using a grasper and arthroscopic shaver. The FHL is then tracked distally to ensure unhindered excursion.
If an open medial approach is utilized, a longitudinal incision is made posterior to the medial malleolus, curving distally toward the sustentaculum tali. The neurovascular bundle (posterior tibial artery and tibial nerve) is identified and gently retracted posteriorly. The FHL tendon sheath, located deep and lateral to the neurovascular bundle, is incised longitudinally. A thorough tenosynovectomy is performed, and any intratendinous nodules are sharply excised. The retinaculum is left open to prevent recurrent stenosis.
Peroneal Tendon Reconstruction
The surgical management of peroneal tendon injuries requires a meticulous, adaptable approach, as intraoperative pathology often exceeds preoperative imaging estimates.
Step 1: Positioning and Exposure
With the patient in the lateral decubitus position, a longitudinal incision is made along the posterior border of the distal fibula, extending 2 to 3 centimeters proximal to the tip of the lateral malleolus and curving gently toward the base of the fifth metatarsal. Extreme care is taken during subcutaneous dissection to identify, mobilize, and protect the sural nerve, which typically crosses the operative field at the distal extent of the incision.
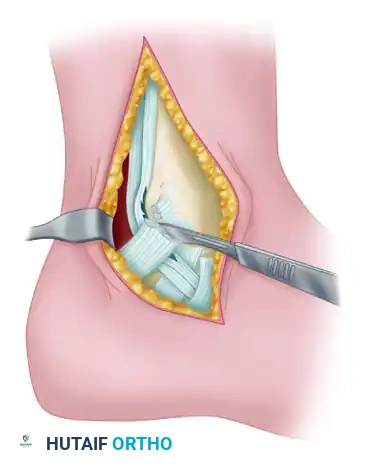
The deep fascia is incised to expose the superior peroneal retinaculum (SPR). The SPR is carefully incised longitudinally, approximately 2 to 3 millimeters posterior to its fibular attachment, leaving a sufficient cuff of tissue on the bone to facilitate a robust repair at the conclusion of the procedure.
Step 2: Tendon Assessment and Debridement
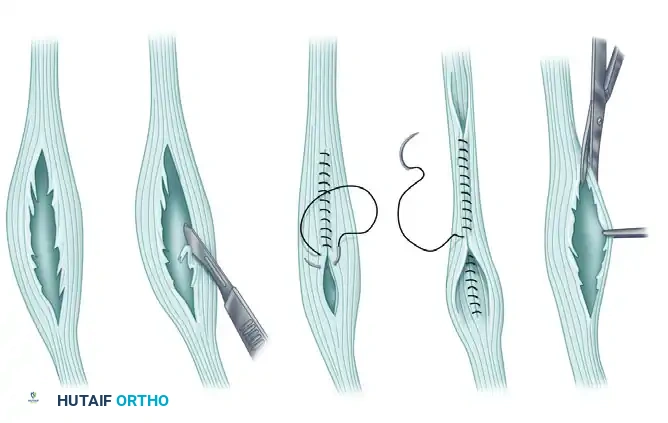
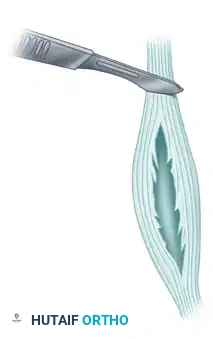
The peroneal tendons are luxated anteriorly out of the retromalleolar groove. The surgeon must systematically inspect both tendons for longitudinal split tears, nodular tendinosis, and low-lying muscle bellies. The peroneus brevis is most commonly injured, presenting as a flattened, frayed structure. If a longitudinal split tear involves less than 50% of the cross-sectional area of the tendon, the degenerative, non-viable margins of the split are meticulously excised using a scalpel or tenotomy scissors.
Following debridement, the remaining healthy tendon is tubularized. This is achieved by suturing the edges together using a running, locking, non-absorbable suture (e.g., 2-0 or 3-0 FiberWire). Tubularization restores the cylindrical architecture of the tendon, minimizing friction and allowing it to glide smoothly within the fibular groove. Any low-lying muscle belly of the peroneus brevis that extends into the retromalleolar groove is excised to decompress the space.
Step 3: Tenodesis for Severe Degeneration
If intraoperative inspection reveals that the peroneus brevis is severely degenerated, heavily frayed, and comprises less than 50% viable tendinous tissue, primary repair is doomed to fail. In these advanced scenarios, the diseased segment of the peroneus brevis is entirely resected.
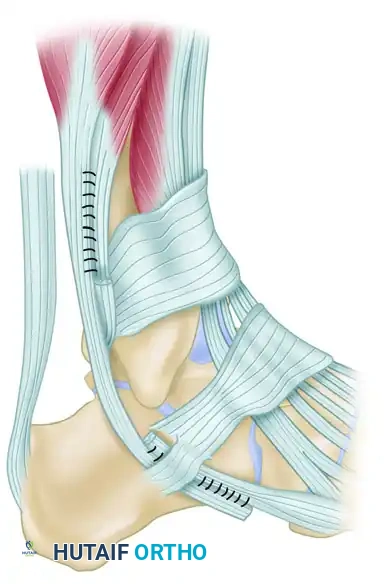
The remaining healthy proximal and distal stumps of the peroneus brevis are then tenodesed directly to the adjacent, intact peroneus longus tendon. This side-to-side tenodesis is executed using a Pulvertaft weave or a robust Krackow suturing technique with heavy non-absorbable sutures. It is imperative to set the tension correctly; the foot must be held in neutral dorsiflexion and slight eversion while the tenodesis is secured to ensure appropriate resting tension and preserve the mechanical advantage of the evertor complex.
Step 4: Retromalleolar Groove Deepening
Attention is then turned to the posterior fibula. If the retromalleolar groove is palpated and found to be shallow, flat, or convex, a groove deepening procedure is mandatory to prevent postoperative subluxation. Using an oscillating saw or an osteotome, a thin cortical flap is elevated from the posterior fibula, hinged medially. The underlying cancellous bone is excavated using a curette or a high-speed burr. The cortical flap is then tamped back into the newly created void, resulting in a deep, concave sulcus that securely houses the repaired tendons.
Step 5: Superior Peroneal Retinaculum Repair
The final, crucial step is the meticulous repair of the SPR. If the native retinaculum is attenuated or has been avulsed from the fibula (a Bankart-like lesion of the ankle), suture anchors must be utilized to secure the SPR directly to the osseous ridge.

A drill guide is utilized to prepare 2 to 3 pilot holes along the posterolateral ridge of the fibula, spaced approximately 1 centimeter apart.

Small-diameter (e.g., 2.5mm or 3.0mm) titanium, PEEK, or biocomposite suture anchors are selected based on surgeon preference and bone quality.
The anchors are inserted into the prepared fibular holes. The surgeon must strictly angle the drill and anchors slightly anteriorly and medially to avoid penetrating the articular cartilage of the distal tibiofibular syndesmosis or the tibiotalar joint.
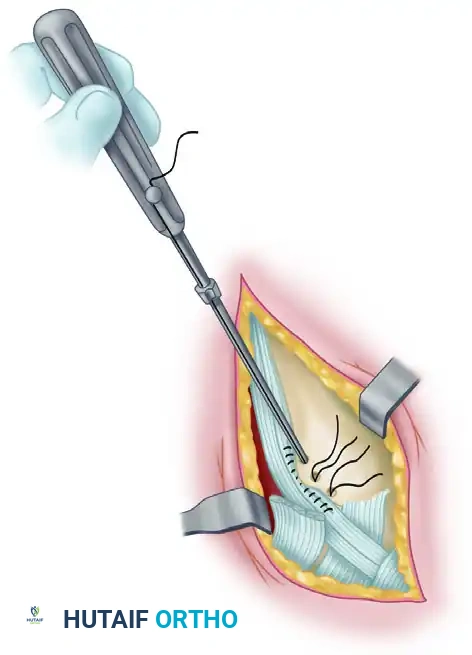
The sutures are passed through the free edge of the SPR in a horizontal mattress fashion. The tendons are reduced into the newly deepened groove, the ankle is held in slight eversion and plantar flexion to remove tension, and the sutures are tied. This securely imbricates the retinaculum over the tendons, eliminating any potential space for subluxation. The stability is dynamically confirmed by taking the ankle through a full, uninhibited range of motion prior to layered closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative management of flexor and peroneal tendon injuries carries a distinct complication profile. The most frequent complication across lateral compartment procedures is iatrogenic injury to the sural nerve. The sural nerve is highly variable in its course, often crossing the operative field at the distal aspect of the fibula or near the base of the fifth metatarsal. Injury can occur via direct transection, vigorous retraction causing neuropraxia, or entrapment within the superficial scar tissue. Patients present with paresthesias, numbness along the lateral border of the foot, or a painful neuroma.
Recurrent tendon subluxation or re-rupture is a catastrophic complication, typically resulting from inadequate initial debridement, failure to recognize and deepen a flat fibular groove, or an overly aggressive postoperative rehabilitation protocol before the SPR has fully healed. Over-tightening of the superior peroneal retinaculum is another significant technical error. If the SPR is imbricated too tightly over the tendons, it creates a localized stenosis, leading to severe postoperative pain, restricted active eversion, and secondary tenosynovitis.
In the medial compartment, FHL decompression carries the risk of injury to the medial calcaneal nerve branches or the main posterior tibial neurovascular bundle, particularly during open approaches. Endoscopic approaches carry a specific risk of injury to the sural nerve (posterolateral portal) or the tibial nerve (posteromedial portal) if anatomical landmarks are not strictly adhered to.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Sural Nerve Injury / Neuroma | 5% - 9% | Direct trauma, aggressive retraction, scar entrapment during lateral approaches. | Initial: Gabapentinoids, desensitization therapy. Salvage: Surgical exploration, neurolysis, or neuroma excision with proximal nerve burying into muscle. |
| Recurrent Peroneal Subluxation | 2% - 5% | Failure to deepen a flat fibular groove; inadequate SPR repair; premature return to sport. | Revision surgery: Formal groove deepening, robust SPR reconstruction with anchors, potential Achilles tendon allograft augmentation of the retinaculum. |
| SPR Over-tightening (Stenosis) | 3% - 6% | Excessive imbrication of the retinaculum during anchor repair. | Initial: Corticosteroid injection into the sheath. Salvage: Surgical release/lengthening of the SPR. |
| Medial Neurovascular Injury | < 2% | Straying anterior to the FHL sheath during open or endoscopic medial approaches. | Immediate intraoperative vascular repair if arterial; primary nerve repair or grafting if tibial nerve is transected. |
| Persistent Pain / Stiffness | 10% - 15% | Inadequate synovectomy, unaddressed osseous impingement, or severe preoperative tendinosis. | Aggressive physical therapy, custom orthotics to correct underlying biomechanics, pain management. |
Phased Post-Operative Rehabilitation Protocols
The success of flexor and peroneal tendon surgery is inextricably linked to a structured, phased postoperative rehabilitation protocol. The delicate balance between protecting the surgical repair and preventing debilitating arthrofibrosis requires meticulous patient compliance and close communication between the surgeon and the physical therapist.
Phase I: Maximum Protection (Weeks 0-2)
Immediately following surgery, the patient is placed in a well-padded, short-leg plaster splint. For peroneal reconstructions, the ankle is immobilized in slight plantar flexion and mild eversion to minimize tension on the repaired superior peroneal retinaculum and the tubularized tendons. For FHL repairs, the ankle is placed in neutral to slight plantar flexion. The patient is strictly non-weight-bearing on the operative extremity, utilizing crutches or a knee scooter. Strict elevation above the level of the heart is mandated to control edema and facilitate wound healing.
Phase II: Early Mobilization and Protected Weight-Bearing (Weeks 2-6)
At the two-week postoperative mark, the splint and sutures are removed. The patient is transitioned into a controlled ankle motion (CAM) boot. Weight-bearing is gradually progressed from touch-down to full weight-bearing as tolerated over the next four weeks. Gentle, active range of motion exercises are initiated out of the boot. For peroneal repairs, isolated active dorsiflexion and plantar flexion are permitted, but active eversion and passive inversion are strictly prohibited to protect the healing SPR and tendon repair. For FHL repairs, active and passive range of motion of the hallux is initiated to prevent tendon tethering in the fibro-osseous tunnel.
Phase III: Strengthening and Proprioception (Weeks 6-12)
By week six, the CAM boot is typically weaned, and the patient transitions to a supportive athletic shoe, often supplemented with a lace-up ankle brace for lateral procedures. Formal, aggressive physical therapy commences. For peroneal injuries, therapy focuses on isometric, progressing to isotonic, eversion strengthening using resistance bands. Proprioceptive training on a BAPS board or Bosu ball is critical to restore the dynamic stabilizing function of the lateral compartment. FHL rehabilitation emphasizes eccentric loading of the gastroc-soleus complex and intrinsic foot muscle strengthening.
Phase IV: Return to Sport and High-Impact Activity (Months 3-6)
The final phase focuses on sport-specific functional training. Patients may begin straight-line jogging, progressing to cutting, pivoting, and explosive jumping activities. Return to competitive sports or classical dance (en pointe) is permitted only when the patient demonstrates symmetric lower extremity strength, full and pain-free range of motion, and the ability to perform single-leg heel raises without apprehension. This milestone is typically achieved between 4 and 6 months postoperatively, though elite athletes may require up to 9 months for complete biomechanical recovery.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative management for flexor and peroneal tendon injuries is heavily grounded in several landmark anatomical and clinical studies. Michelson and Dunn’s seminal evaluation of FHL pathology radically shifted the paradigm, demonstrating that FHL tendinitis is not exclusively a dancer's affliction but a common source of posterior ankle pain in the general population. Their work established the diagnostic utility of the FHL stretch test and the necessity of differentiating soft-tissue tendinopathy from osseous posterior impingement. Furthermore, Hamilton's extensive work on classical ballet dancers defined the surgical indications for FHL release, emphasizing that while conservative care is the mainstay, surgical decompression yields excellent return-to-dance rates when non-operative measures fail.
In the realm of peroneal tendon pathology, Krause and Brodsky’s classification of peroneus brevis split tears remains the cornerstone of surgical decision-making. They articulated the mechanical etiology of the split tear—the compression of the brevis between the fibula and the longus—and standardized the treatment algorithm: tubularization for <50% involvement and tenodesis for >50% degeneration. More recently, biomechanical and clinical consensus, driven by authors such as Title and Myerson, has cemented the necessity of fibular groove deepening. Current clinical guidelines strongly advocate for routine assessment and deepening of the retromalleolar groove in all cases of peroneal subluxation or significant tearing, as isolated soft-tissue repair of the superior peroneal retinaculum has an unacceptably high failure rate in the presence of a convex or shallow fibular morphology. These evidence-based principles ensure that the modern orthopedic surgeon can approach these complex hindfoot pathologies with a robust, reliable, and anatomically sound surgical strategy.
