Surgical Management of Acromioclavicular Joint Dislocations: Resection and Reconstruction Techniques
Key Takeaway
The surgical management of acromioclavicular (AC) joint dislocations requires a nuanced understanding of coracoclavicular ligament integrity. While the Mumford procedure (distal clavicle resection) is highly effective for chronic, symptomatic Grade I and II injuries with intact ligaments, high-grade chronic dislocations (Grades III-V) necessitate robust coracoclavicular reconstruction, such as the Weaver-Dunn or Rockwood techniques, to restore biomechanical stability and prevent debilitating shoulder hypermobility.
ACROMIOCLAVICULAR JOINT DISLOCATIONS: PRINCIPLES AND BIOMECHANICS
The acromioclavicular (AC) joint is a diarthrodial joint that serves as the sole articular linkage between the axial skeleton and the upper extremity. Its stability is governed by a complex interplay of static and dynamic stabilizers. The static stabilizers include the AC capsule and ligaments (which primarily resist anteroposterior translation) and the robust coracoclavicular (CC) ligaments—comprising the conoid and trapezoid bundles—which are the primary restraints to superior and axial translation of the clavicle relative to the scapula. The dynamic stabilizers consist of the deltoid and trapezius musculature, which envelop the joint via the deltotrapezial fascia.
The Rockwood classification system remains the gold standard for categorizing AC joint injuries and is universally applied to both acute and old unreduced (chronic) dislocations. Surgical decision-making hinges heavily on this classification, the chronicity of the injury, and the functional demands of the patient.
Clinical Pearl: The critical distinction in surgical planning for AC joint pathology is the integrity of the coracoclavicular ligaments. Procedures designed for intact CC ligaments (Grades I and II) will fail catastrophically if applied to high-grade injuries (Grades III, IV, and V) without concurrent ligamentous reconstruction.
SURGICAL INDICATIONS AND DECISION MAKING
Low-Grade Injuries (Grades I and II)
In Grade I and II injuries, the coracoclavicular ligaments remain structurally intact, though the AC ligaments may be sprained or torn. Acute injuries in this category are universally managed non-operatively. However, a subset of these patients will develop chronic, debilitating symptoms secondary to post-traumatic osteolysis, meniscoid tear, or degenerative osteoarthritis of the AC joint. For these chronic, symptomatic, unreduced Grade I or II dislocations, resection of the distal end of the clavicle (the Mumford procedure) is highly indicated.
High-Grade Injuries (Grades III, IV, and V)
In these severe injuries, both the AC and CC ligaments are completely disrupted, leading to gross instability of the shoulder girdle.
Surgical Warning: The Mumford procedure is strictly contraindicated as an isolated operation for acutely injured Grade I or II joints, and it is absolutely contraindicated for any Grade III, IV, or V injury. If distal clavicle resection is performed in the presence of torn CC ligaments, the clavicle will remain hypermobile, leading to severe, intractable irritation of the surrounding soft tissues and profound shoulder dysfunction.
Therefore, in chronic unreduced dislocations of Grades III, IV, and V, the surgical strategy must pivot to anatomical or non-anatomical reconstruction of the coracoclavicular ligaments, often combined with distal clavicle resection to prevent painful impingement.
RESECTION OF THE LATERAL END OF THE CLAVICLE (MUMFORD / GURD PROCEDURE)
The open resection of the distal clavicle, originally described independently by Mumford and Gurd, remains a reliable, time-tested procedure for isolated AC joint pathology with intact CC ligaments.
Preoperative Planning and Positioning
- Anesthesia: General endotracheal anesthesia is typically employed, often supplemented with an interscalene regional nerve block for optimal postoperative pain control.
- Positioning: The patient is placed in the beach-chair position with the head secured in a neutral posture. The operative arm must be draped free to allow for full intraoperative range of motion, which is critical for assessing impingement post-resection.
- Fluoroscopy: A C-arm should be available to confirm the extent of the resection, ensuring adequate decompression without compromising the trapezoid ligament insertion.
Surgical Technique 61-7 (Mumford; Gurd)
- Incision and Exposure: Expose the lateral end of the clavicle through a short, 3 to 4 cm curved incision centered over the AC joint. The incision should follow Langer’s lines where possible, typically running in a sagittal or slightly oblique plane.
- Subperiosteal Dissection: Incise the deltotrapezial fascia directly over the superior aspect of the distal clavicle. By dissecting strictly subperiosteally, free the lateral 2.5 cm of the clavicle from all soft tissue attachments.
- Bone Resection: Using a microsagittal saw or sharp bone-cutting rongeurs, resect approximately 2.5 cm of the distal clavicle.
- Surgical Pitfall: The trapezoid ligament inserts approximately 3 cm medial to the distal articular surface of the clavicle. Resecting more than 2.5 cm risks iatrogenic detachment of the trapezoid, converting a stable joint into an unstable one. Modern modifications often advocate for a more conservative resection of 1 to 1.5 cm, which is usually sufficient to prevent bony impingement.
- Contouring the Clavicle: Smooth the superior and posterior borders of the remaining lateral end of the clavicle with a rasp or file. This step is crucial to eliminate any sharp bony ridges beneath the skin that could cause postoperative pain or hardware-like prominence. It is unnecessary to disturb the cartilaginous surface of the acromion unless concurrent subacromial impingement dictates an acromioplasty.
- Soft Tissue Plication: Meticulously plicate and suture the periosteum and the deltotrapezial fascia over the raw, cancellous end of the clavicle. A robust repair of this fascia provides a dynamic stabilizing force and prevents superior migration of the clavicle. Use heavy, non-absorbable or long-lasting absorbable sutures (e.g., #2 FiberWire or #1 PDS) in an interrupted fashion.
Postoperative Care
The shoulder is immobilized in a Velpeau dressing or a standard shoulder sling for 1 week to allow the soft tissue plication to begin healing. Following this brief period of immobilization, active use and progressive range of motion are encouraged. Heavy lifting and overhead resistance exercises should be delayed until 6 to 8 weeks postoperatively to ensure complete fascial healing.
RECONSTRUCTION OF THE CORACOCLAVICULAR LIGAMENTS
In chronic, unreduced AC dislocations of Grades III, IV, and V, the primary surgical objective is the restoration of the coracoclavicular restraint. Over the decades, numerous techniques have been developed, ranging from dynamic muscle transfers to static ligamentous reconstructions.
The Neviaser Technique
Historically, Neviaser described an operation in which the coracoacromial (CA) ligament is detached from the coracoid and utilized to reconstruct the superior acromioclavicular ligament.
While this technique addresses the AC capsule, it possesses a critical biomechanical flaw: it does not reconstruct the primary vertical stabilizers—the coracoclavicular ligaments. Because the CC ligaments remain incompetent, the Neviaser method is frequently followed by recurrent superior migration and redislocation of the clavicle. Consequently, it is rarely used in modern practice as an isolated procedure for high-grade injuries.
The Weaver-Dunn Procedure
To address the shortcomings of isolated AC capsular repairs, Weaver and Dunn described a landmark technique that shifts the focus to the CC interval. In this procedure, the coracoacromial (CA) ligament is detached from its insertion on the acromion and transferred to the remaining end of the distal clavicle.
Biomechanical Rationale:
The Weaver-Dunn procedure is almost universally combined with a resection of the lateral end of the clavicle (to prevent AC impingement). The transferred CA ligament acts as a surrogate for the ruptured CC ligaments. However, biomechanical studies have demonstrated that the native CA ligament possesses only about 25% of the tensile strength of the native intact CC ligaments.
Clinical Pearl: The Weaver-Dunn transfer provides a dynamic reduction force on the distal clavicle, but it lacks sufficient static strength to hold the clavicle reduced during the early healing phase. Therefore, this procedure must be combined with some form of stabilizing fixation (a static stabilizer) to protect the ligamentous repair until biologic healing occurs.
Surgical Steps of the Weaver-Dunn Transfer:
1. Exposure: A saber incision is made over the AC joint, extending down to the tip of the coracoid process.
2. Distal Clavicle Resection: A standard Mumford-style resection of the distal 1 to 1.5 cm of the clavicle is performed.
3. Ligament Harvest: The CA ligament is identified. It is carefully detached from the acromion. Modification: Many surgeons harvest the CA ligament with a small fleck of acromial bone to allow for bone-to-bone healing when transferred to the clavicle.
4. Preparation of the Clavicle: The medullary canal of the resected distal clavicle is broached and prepared to receive the CA ligament. Drill holes are placed through the superior cortex of the clavicle.
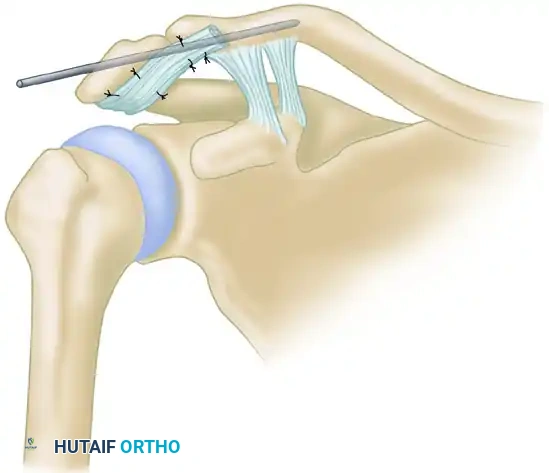
5. Transfer and Fixation: Heavy non-absorbable sutures are woven through the CA ligament (or its bone block). The ligament is drawn into the medullary canal of the clavicle and secured by tying the sutures over the superior bony bridge.
6. Supplemental Fixation: Because the CA ligament is weak, the reduction must be protected. This is traditionally achieved using heavy non-absorbable suture loops (e.g., cerclage) passed under the coracoid and over the clavicle, or via metallic fixation.
The Rockwood Modification
Recognizing the need for rigid static protection of the CA ligament transfer, Rockwood described a highly effective modification. In this technique, the transfer of the coracoacromial ligament from the acromion to the clavicle is performed simultaneously while the clavicle is held in a perfectly reduced anatomical position using a Bosworth screw.
The Bosworth Screw Technique:
- A heavy, fully threaded cancellous screw (the Bosworth screw) is passed through a drill hole in the superior aspect of the clavicle and driven directly into the base of the coracoid process.
- This screw acts as an unyielding static stabilizer, completely offloading the transferred CA ligament and allowing it to heal without tension.
- Outcomes: Pavlik et al. reported the use of a similar technique with highly satisfactory results. In their series of 17 patients with chronic AC dislocations, 11 patients achieved excellent clinical and radiographic results. Complications were minimal but notable: two patients experienced a partial loss of reduction, and one patient experienced loosening of the Bosworth screw.
Surgical Warning: Rigid metallic fixation between the clavicle and the coracoid (such as a Bosworth screw) eliminates the normal physiologic rotation of the clavicle that occurs during shoulder elevation. Therefore, the screw must be routinely removed at 8 to 12 weeks postoperatively, once the ligament transfer has healed, to restore normal shoulder biomechanics and prevent hardware breakage.
MODERN PERSPECTIVES AND COMPLICATIONS
While the Weaver-Dunn and Rockwood modifications laid the foundation for chronic AC joint reconstruction, modern orthopedic surgery has increasingly shifted toward anatomic CC ligament reconstructions using free tendon allografts or autografts (e.g., semitendinosus). These modern techniques aim to recreate both the conoid and trapezoid bundles, providing superior biomechanical strength compared to the CA ligament transfer.
Regardless of the technique chosen, surgeons must be vigilant regarding potential complications:
- Loss of Reduction: The most common complication, often due to premature failure of the supplemental fixation or stretching of the transferred ligament.
- Hardware Complications: Migration of pins, breakage of screws, or osteolysis around suture buttons.
- Infection and Wound Healing: The subcutaneous nature of the AC joint makes it susceptible to wound breakdown, particularly if bulky knots or hardware are placed directly beneath the incision.
- Clavicle Fracture: Over-drilling the clavicle for suture passage or screw placement creates stress risers, predisposing the patient to postoperative clavicle fractures.
Meticulous surgical technique, strict adherence to biomechanical principles, and carefully phased postoperative rehabilitation are paramount to achieving successful, long-term outcomes in the surgical management of acromioclavicular joint dislocations.
You Might Also Like


