Advanced Principles of Skin Coverage and Scar Management in the Hand
Key Takeaway
Effective skin coverage in hand surgery is paramount for restoring function and preventing debilitating contractures. This guide details the management of granulating areas and complex scars, emphasizing the biomechanics of hand skin. It provides step-by-step surgical approaches for linear and area scar revision, including Z-plasty and full-thickness grafting, ensuring optimal outcomes for orthopedic and reconstructive hand surgeons.
INTRODUCTION TO SKIN COVERAGE IN THE HAND
The soft tissue envelope of the hand is a highly specialized, dynamic structure that must accommodate extreme ranges of motion while providing durable, sensate coverage for underlying neurovascular, tendinous, and osseous structures. In the context of acute trauma, burns, or post-surgical complications, achieving definitive skin coverage is a paramount objective. Failure to restore a pliable, gliding soft tissue envelope inevitably leads to debilitating contractures, joint stiffness, and profound functional impairment.
This comprehensive guide delineates the evidence-based principles of managing granulating areas, the biomechanics and pathophysiology of hand scars, and the advanced surgical techniques required for linear and area scar revision.
MANAGEMENT OF GRANULATING AREAS
A granulating wound bed on the hand represents a critical juncture in surgical decision-making. Healing by secondary intention (allowing a granulating area to heal with a scar) is rarely acceptable in hand surgery, as the resulting cicatrix is invariably contracted, nonelastic, and functionally restrictive.
Indications and Timing for Coverage
If the hand has not been completely covered with skin during the initial treatment of an acute injury, definitive coverage must be achieved as soon as the wound bed is optimized.
- Split-Thickness Skin Grafts (STSG): An STSG should be applied as soon as the granulating surface is clean, vascularized, and devoid of necrotic debris or active infection. Even if the entire granulating surface is not uniformly clean, any discrete portion that is capable of supporting a graft should be covered to halt the inexorable process of myofibroblast-mediated wound contraction.
- Flap Coverage: It is a fundamental tenet of reconstructive surgery that avascular structures cannot support a free skin graft. Exposed tendons (devoid of paratenon), joints (devoid of capsule), or cortical bone (devoid of periosteum) mandate coverage with vascularized flap grafts (e.g., local rotational flaps, regional pedicled flaps, or free tissue transfer).
Surgical Warning: Attempting to place a split-thickness or full-thickness skin graft directly over bare tendon or denuded cortical bone will result in 100% graft failure, subsequent desiccation of the underlying structures, and severe functional loss.
PATHOPHYSIOLOGY AND BIOMECHANICS OF HAND SCARS
A scar is a biologically inferior substitute for native skin. Understanding the limitations of scar tissue is essential for the reconstructive surgeon.
Biomechanical Limitations
- Loss of Elasticity: Normal skin possesses a complex network of elastin and collagen that allows for multidirectional stretch. Scar tissue, composed predominantly of dense, disorganized Type I collagen, is entirely nonelastic. This absence of elasticity restricts the motion of otherwise unobstructed underlying joints and interferes with the microvascular nutrition of adjacent tissues.
- Deep Adhesions: Scars rarely exist in isolation within the epidermis and dermis. They frequently adhere to underlying joints, tendons, and ligaments. This tethering effect abolishes the independent glide of flexor and extensor tendons, profoundly limiting active range of motion.
- Contracture Mechanics: A scar inherently contracts during the remodeling phase of healing and does not spontaneously stretch later. When a linear scar spans a joint (particularly across flexor creases), the intermittent stretching from active motion induces microtrauma. This mechanical stress stimulates further fibroblast proliferation, causing the scar to hypertrophy.
- Rupture and Fissuring: Forced passive stretching of a mature, contracted scar does not yield increased length. Instead, it causes the inelastic scar to rupture and fissure. These micro-tears heal with secondary inflammation, ultimately resulting in a thicker, more rigid scar.
- Neuromatous Pain: A scar not only lacks normal tactile and protective sensation but may become exquisitely painful if it adheres to or entraps regenerating nerve endings, leading to localized neuromas.
SURGICAL MANAGEMENT OF SCARS: PRINCIPLES AND INDICATIONS
While scars cannot be entirely eliminated—as the very process of surgical intervention relies on the production of new scar tissue—they can be strategically replaced, redirected, or altered to minimize functional interference.
Indications for Scar Revision
Surgical intervention for a hand scar is indicated to achieve one or more of the following objectives:
1. Eliminate Deformity: Correcting aesthetic and structural distortions caused by tissue contraction.
2. Restore Joint Motion: Releasing tethered skin that prevents full flexion or extension.
3. Provide Durable Coverage: Replacing unstable, ulcerating scars over vulnerable parts to permit future operations on deeper structures (e.g., prior to a planned tendon graft or nerve repair).
4. Relieve Pain: Excisional release of painful neuromatous scars.
5. Improve Appearance: Occasionally indicated for severe cosmetic disfigurement, though function always supersedes aesthetics in the hand.
Timing of Surgical Intervention
The timing of scar revision requires a delicate balance between allowing tissue maturation and preventing irreversible joint contractures.
- The Maturation Rule: Whenever possible, a scar should not be surgically replaced or revised until it has fully matured. This process typically requires a minimum of 3 to 6 months. A mature scar is characterized by a decrease in erythema, softening of the tissue, and stabilization of contracture.
- The Contracture Exception: Early intervention is absolutely mandated when a scar severely limits joint motion in a manner that threatens the joint capsule or collateral ligaments. For example, if a metacarpophalangeal (MCP) joint is held in rigid extension, or a proximal interphalangeal (PIP) joint is held in rigid flexion, a severe secondary capsular contracture will develop rapidly. In these instances, the offending scar must be released and grafted immediately, without awaiting full maturation.
OPERATIVE TECHNIQUES FOR LINEAR SCARS
Disabling linear scars typically result from surgical incisions placed perpendicular to the lines of tension (violating Brunner's principles) or from traumatic lacerations that cross flexor creases.
The Z-Plasty Release
When a linear scar on a digit is narrow and surrounded by supple, normal tissue, it can be effectively released and lengthened using a Z-plasty.

Biomechanics of the Z-Plasty:
The Z-plasty serves two primary functions: it lengthens the contracted scar and reorients the direction of the central limb to fall within the neutral lines of tension. A standard 60-degree Z-plasty theoretically increases the length of the central limb by 73%.
Surgical Steps:
1. Design: The central limb of the "Z" is drawn directly over the contracted linear scar. Two lateral limbs are drawn at 60-degree angles to the central limb. The lengths of all three limbs must be exactly equal.
2. Incision and Elevation: The incisions are made through the dermis into the subcutaneous fat. The two triangular flaps are elevated. Care must be taken to preserve the subdermal vascular plexus to prevent flap necrosis.
3. Transposition: The flaps are transposed, interchanging their positions. This maneuver breaks up the linear line of tension and introduces healthy, elastic tissue into the concavity of the contracture.
4. Closure: The flaps are sutured with fine, non-absorbable monofilament (e.g., 5-0 or 6-0 nylon) using minimal tension.

Clinical Pearl: While highly effective on the dorsal surface or for narrow volar scars, a scar more than 2 mm wide on the volar surface is exceedingly difficult to correct with a simple Z-plasty. The volar skin is highly specialized, tethered by Cleland's and Grayson's ligaments, and lacks the mobility of dorsal skin. In such instances, the scar must be excised entirely and replaced by a full-thickness free graft.
OPERATIVE TECHNIQUES FOR AREA SCARS
Area scars involve a broader expanse of tissue loss and cannot be managed with local tissue rearrangement alone. They require the importation of new tissue, typically via skin grafting. The approach differs significantly depending on whether the defect is dorsal or volar.
Dorsal Area Scars
The dorsum of the hand requires a massive amount of skin redundancy to accommodate full flexion of the wrist and digits.

Biomechanical Considerations:
* Longitudinal Redundancy: The normal adult hand possesses approximately 5 cm of extra skin longitudinally on the dorsum to allow for simultaneous flexion of the wrist and fingers.
* Transverse Redundancy: There is approximately 2.5 cm of extra skin transversely to allow for the development of the metacarpal arch when making a fist.
Surgical Approach:
An area scar on the dorsum of the hand involving only the skin may be replaced by a medium or thick split-thickness skin graft (STSG) or a full-thickness skin graft (FTSG) of carefully planned size.
- Excision: The scar is excised entirely down to healthy, gliding paratenon or areolar tissue. If tendons or nerves must be exposed for concurrent procedures, the incision should be planned along the edge of the proposed flap/graft, never directly through the center of it.
- Positioning for Grafting: A graft placed on the dorsum must account for the required extra skin, the previous shrinkage of the scar, and the anticipated secondary contraction of the graft itself.
- The "Fist" Position: The graft must be placed and secured while the hand is immobilized in the position of maximum skin tension. Burm et al. demonstrated that the greatest amount of skin can be grafted to the dorsum with the hand in the "fist" position (MCPs, PIPs, and DIPs fully flexed). This anatomical position allows for significantly more skin incorporation than the traditional "safe" (James) position.

Pitfall: While the fist position maximizes dorsal skin length, maintaining the fingers in extreme flexion for prolonged periods postoperatively risks severe interphalangeal flexion contractures. The surgeon must balance the need for dorsal skin length with the risk of volar capsular contracture, often necessitating early, supervised mobilization.
Volar and Palmar Area Scars
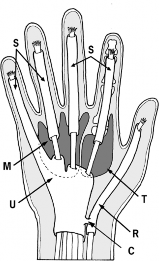
The skin of the palm is anatomically unique. It is glabrous, highly sensitive, possesses a thick stratum corneum, and is firmly anchored to the underlying palmar aponeurosis by dense fibrous septa. This architecture allows it to withstand immense friction and shear forces during grip.
Graft Selection:
* Similar replacement skin is found only on the sole of the foot.
* If the palmar scar is strictly superficial, a thick split-thickness graft may be utilized.
* If deep, vulnerable structures are involved, or if the area is subjected to heavy functional wear, a full-thickness skin graft (FTSG) is strongly preferred.
Challenges of FTSG:
While FTSGs provide superior durability and less secondary contraction, they are more technically demanding. They require a pristine, highly vascular wound bed to survive (plasmatic imbibition followed by inosculation). Furthermore, their size is limited by the donor site morbidity, as the donor defect must typically be closed primarily after extensive undermining of the edges.

Incision Planning:
When a graft is applied to the palm, the margins of the excision must strictly follow the rules that guide the location and direction of hand incisions (e.g., utilizing mid-axial lines, avoiding perpendicular crossing of flexor creases). The graft will heal to the normal skin with a linear scar at its periphery; if this peripheral scar crosses a crease improperly, a new contracture will form.
Specialized Coverage: Neurovascular Island Flaps
For an insensitive, large area scar located in a critical zone of function—most notably the radial side of an otherwise normal index finger or the ulnar aspect (area of pinch) of the thumb—simple skin grafting is insufficient. These areas require not only durable coverage but also protective and tactile sensation to function effectively in pinch and grasp.
In these specific scenarios, a neurovascular island flap (e.g., a Littler flap transferred from the ulnar aspect of the ring finger or the radial aspect of the middle finger) is indicated. This technique transfers a composite island of skin, subcutaneous tissue, and its intact neurovascular bundle, instantly restoring durable, sensate coverage to the critical pinch area.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of skin coverage and scar revision relies heavily on meticulous postoperative care.
- Immobilization: Skin grafts must be protected from shear forces during the initial phase of healing. A tie-over bolster dressing is typically applied to apply uniform pressure, prevent hematoma formation, and ensure intimate contact between the graft and the wound bed. The hand is splinted in a functional or anti-deformity position depending on the graft location.
- Graft Inspection: The bolster is generally removed at 5 to 7 days postoperatively to inspect for graft take.
- Rehabilitation: Once the graft is fully adherent and the margins are sealed (typically 10-14 days), gentle active range of motion is initiated.
- Scar Management: As the graft matures, aggressive scar management is instituted. This includes deep friction massage, the application of silicone gel sheeting, and the use of custom-molded compression garments (e.g., Isotoner gloves) to minimize hypertrophic scarring and maximize tissue pliability. Night splinting may be required for several months to counteract the forces of secondary graft contraction.
You Might Also Like