Secondary Repair and Reconstruction of Flexor Tendons: A Comprehensive Surgical Guide
Key Takeaway
Secondary repair of flexor tendons is indicated when primary repair is delayed beyond 10 to 14 days. Successful reconstruction requires meticulous assessment of the injury zone, tendon retraction, and joint suppleness. Techniques range from direct delayed repair and profundus advancement to single-stage tendon grafting and distal joint arthrodesis. Strict adherence to biomechanical principles and staged rehabilitation is paramount for restoring optimal hand function and preventing contractures.
INTRODUCTION TO SECONDARY FLEXOR TENDON REPAIR
The management of flexor tendon injuries remains one of the most exacting challenges in hand surgery. While primary repair (within 24 to 48 hours) is universally preferred to optimize functional outcomes and minimize peritendinous adhesions, clinical realities often dictate a delayed approach. When flexor tendons cannot be repaired within the acute window, the surgeon enters the realm of secondary repair and reconstruction.
Secondary repairs are temporally classified into two distinct phases:
1. Delayed Primary Repair (10 to 14 days): The biological environment is still amenable to direct end-to-end repair, though early fibrotic changes and mild myotendinous retraction have begun.
2. Late Secondary Repair (Greater than 4 weeks): Direct repair is frequently impossible due to fixed muscle contracture, advanced tendon retraction, and obliteration of the flexor sheath. Reconstruction typically mandates tendon grafting, advancement, tenodesis, or arthrodesis.
This comprehensive guide delineates the indications, biomechanical considerations, and operative techniques required for the secondary reconstruction of flexor tendons across various anatomical zones, with a specific focus on the Flexor Digitorum Profundus (FDP) and Flexor Digitorum Superficialis (FDS).
PREREQUISITES FOR SECONDARY RECONSTRUCTION
Before embarking on any secondary tendon reconstruction, the hand must meet strict physiological and anatomical criteria. Failure to respect these prerequisites invariably leads to poor functional outcomes, severe contractures, or graft rupture.
- Tissue Equilibrium: The soft tissue envelope must be healed, pliable, and free of active infection or severe induration.
- Joint Suppleness: Passive range of motion (PROM) must be maximized. A tendon graft cannot mobilize a stiff joint. Preoperative hand therapy is mandatory to achieve full passive flexion and extension.
- Sensibility: Adequate protective sensation (or improving sensibility following nerve repair) is critical. A functionally blind digit will not be integrated into the patient's grip biomechanics.
- Pulley System Integrity: The critical A2 and A4 pulleys must be intact or reconstructable to prevent bowstringing and ensure mechanical efficiency.
Clinical Pearl: The "Lumbrical Plus" finger is a notorious complication of FDP division distal to the lumbrical origin. As the FDP retracts proximally, it pulls the lumbrical with it, increasing tension on the lateral bands. When the patient attempts to flex the finger, the force is transmitted through the lumbrical, resulting in paradoxical extension of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints.
ZONE II INJURIES: ISOLATED PROFUNDUS LACERATIONS
Zone II, historically termed "no man's land" by Bunnell, contains both the FDS and FDP within a tight fibro-osseous sheath. Management of an isolated FDP laceration in this zone depends entirely on the time elapsed since injury.
The Delayed Primary Period (10 to 14 Days)
When the FDP alone has been divided in Zone II, the intact FDS (sublimis) tendon continues to provide ample flexion of the PIP joint. In a highly flexible hand, the loss of DIP flexion might be functionally tolerated, but repair is generally indicated to restore terminal grip strength.
During the 10 to 14-day window, meticulous direct repair of the flexor profundus can result in highly satisfactory function. The tendon ends can usually be retrieved, and the myotendinous unit retains sufficient elasticity to permit an end-to-end coaptation without excessive tension.
The Late Secondary Period (4 Weeks and Beyond)
After 4 weeks, the proximal FDP stump has typically retracted into the palm, the vincula have ruptured, and the muscle belly has undergone fixed contracture. Under these circumstances, it is highly doubtful that a direct repair would be successful. Attempting to force a direct repair under high tension will result in the Quadrigia Effect—a phenomenon where the overtensioned FDP restricts the proximal excursion of the adjacent, uninjured FDP tendons sharing the same common muscle belly, thereby limiting global hand flexion.
Extensive surgical treatment for an isolated late FDP laceration is rarely necessary unless the distal joint is extremely hyperextensible and "flail." Depending on the functional demands of the patient, the following salvage options are considered:
- Distal Joint Arthrodesis: Fusing the DIP joint in 10 to 15 degrees of flexion provides a stable post for pinch. This is highly recommended for the index and long fingers, where tip pinch is paramount.
- Distal Tenodesis: Anchoring the distal FDP stump to the middle phalanx to stabilize the DIP joint.
- Profundus Advancement (Wagner Technique): Applicable only if the tendon has retracted minimally and the gap is less than 1 cm.
SURGICAL TECHNIQUE: WAGNER PROFUNDUS ADVANCEMENT
The Wagner technique is a classic method for advancing a distally lacerated FDP tendon and anchoring it directly into the distal phalanx. It is strictly indicated for Zone I or very distal Zone II injuries where the tendon length allows advancement without inducing a Quadrigia effect.
Step 1: Exposure and Tendon Retrieval
Under tourniquet control and loupe magnification, utilize a Bruner zigzag or mid-lateral incision over the distal and middle phalanges. Expose the flexor tendon sheath, preserving the A4 pulley. Identify the divided FDP tendon.
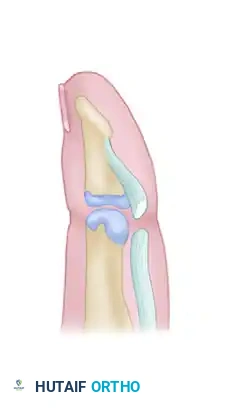
Figure 1: Illustration demonstrating a divided flexor digitorum profundus tendon near its insertion at the base of the distal phalanx.
Step 2: Preparation of the Insertion Site
Elevate a small osteoperiosteal flap at the anatomical footprint of the FDP on the volar base of the distal phalanx. Use a curette or a small burr to create a shallow bony trough to enhance tendon-to-bone healing.
Step 3: Suture Placement
Place a heavy, non-absorbable core suture (e.g., 3-0 or 4-0 Prolene) into the proximal stump of the FDP using a modified Kessler or Bunnell configuration. Ensure the suture grasps the tendon securely.
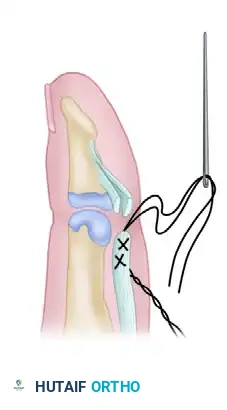
Figure 2: Placement of a locking core suture through the proximal stump of the flexor digitorum profundus tendon.
Step 4: Transosseous Fixation
Using a Keith needle or a small drill bit, create two divergent holes from the volar bony trough exiting through the dorsal cortex of the distal phalanx, just proximal to the germinal matrix of the nail. Pass the two ends of the core suture through these transosseous tunnels.
Step 5: The Pull-Out Button
Draw the tendon stump firmly into the bony trough. Tie the suture ends over a sterile, padded button resting on the dorsal aspect of the nail plate. This pull-out wire/suture technique provides rigid fixation while bone-to-tendon healing occurs.
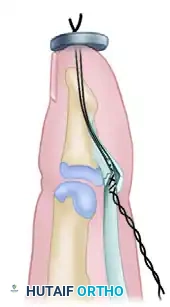
Figure 3: The completed Wagner technique of profundus advancement, showing the tendon secured into the distal phalanx and tied over a dorsal pull-out button.
Surgical Warning: Do not advance the FDP more than 1 cm. Excessive advancement will tether the common profundus muscle belly, severely restricting the flexion of the adjacent, uninjured digits (Quadrigia Effect). If the gap exceeds 1 cm, abandon advancement in favor of arthrodesis or grafting.
ZONE II INJURIES: COMBINED FDP AND FDS LACERATIONS
When both the FDP and FDS tendons have been divided in Zone II, and conditions do not permit primary or delayed primary repair, the digit is rendered functionally useless.
If all prerequisites are met (healed and stable wound, flexible joints, and good or improving sensibility), flexor function can be restored with a single-stage tendon graft.
Principles of Single-Stage Tendon Grafting
- Donor Selection: The palmaris longus is the graft of choice due to its expendability and appropriate caliber. Alternatives include the plantaris tendon or a toe extensor.
- Excision of Fibrosis: The scarred remnants of the FDS and FDP must be meticulously excised from the fibro-osseous canal.
- Pulley Preservation: The A2 and A4 pulleys must be rigorously preserved. If destroyed, they must be reconstructed (using tendon slips or extensor retinaculum) prior to or concurrently with grafting.
- Proximal Coaptation: The graft is typically woven into the proximal FDP motor in the palm (Zone III) or distal forearm (Zone V) using a Pulvertaft weave to ensure a strong, early-active-motion-compatible repair.
- Distal Fixation: The distal end of the graft is anchored to the distal phalanx using a pull-out button technique or suture anchors.
ZONES III, IV, AND V: FOREARM AND PALM RECONSTRUCTION
Injuries in the palm (Zone III), carpal tunnel (Zone IV), and distal forearm (Zone V) carry a generally better prognosis than Zone II injuries because the tendons lie in an extrasynovial environment with abundant vascularity and lack tight fibro-osseous constraints.
Delayed Repair (3 to 4 Weeks)
Flexor tendons in the forearm and palm can often be repaired 3 or 4 weeks after injury by direct suture. The inherent elasticity of the muscle-tendon unit, combined with the ability to flex the wrist, usually accommodates the gap sufficiently to overcome muscle retraction.
Late Reconstruction (Beyond 4 to 5 Weeks)
After 4 or 5 weeks, the flexor muscles become tightly contracted. Attempting to drag the tendon distally by acutely flexing the wrist will result in severe flexion contractures and poor functional excursion. At this stage, a graft is necessary to bridge the gap between the tendon ends.
The "Minigraft" Technique
In the palm or distal forearm, a short segmental graft (often termed a "minigraft") can be interposed between the retracted tendon ends. This avoids excessive tension while restoring continuity.
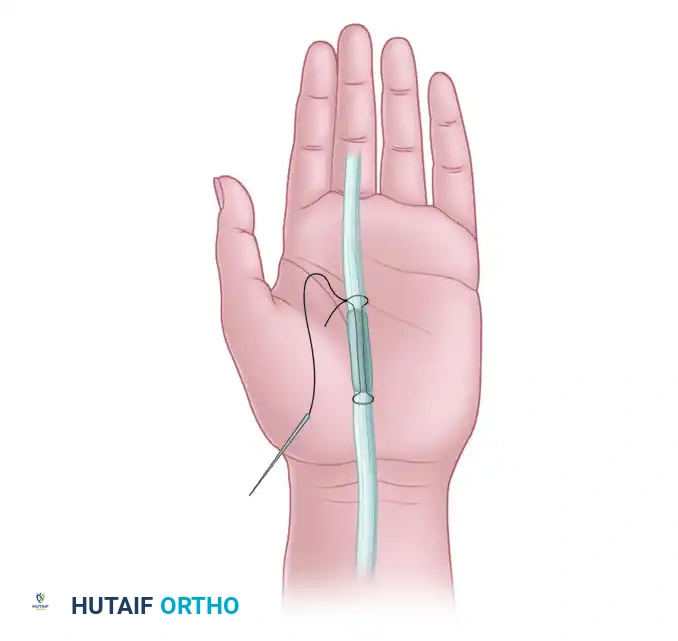
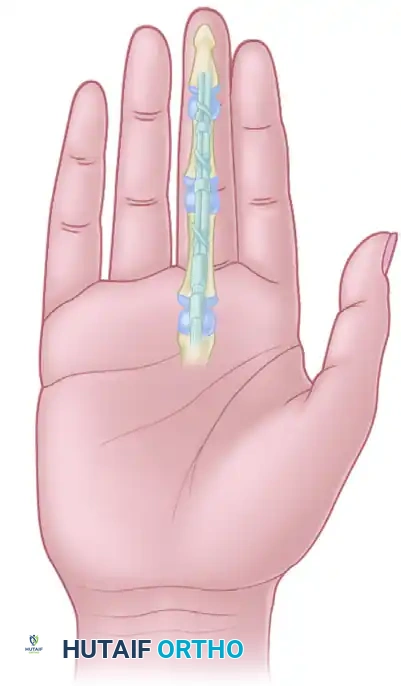
Figure 4: Long-standing flexor tendon interruptions in the palm may require a short segmental graft or “minigraft” to bridge the defect and avoid excessive tension on the repair.
Surgical Steps for Minigrafting:
1. Debridement: Freshen the ends of the proximal and distal tendon stumps until healthy, parallel collagen bundles are visible.
2. Graft Harvest: Harvest a short segment of palmaris longus.
3. Interposition: Place the graft between the stumps.
4. Repair: The tendons can be attached with a strong multiple-strand technique (e.g., 4-strand or 6-strand core suture) using 4-0 nonabsorbable suture (Prolene or braided polyester). In the distal forearm, where bulk is less of an issue, a Pulvertaft weave or monofilament wire mattress sutures may be utilized for maximum strength.
Tendon Transfers in Severe Destruction
When tendons have been extensively destroyed (e.g., crush injuries, severe infections), the profundus tendons take absolute priority for reconstruction to restore terminal grip. If the proximal FDP muscle belly is fibrosed or destroyed, an adjacent, available proximal FDS tendon (e.g., FDS of the ring or middle finger) can be transferred and attached to the distal FDP stumps. This transfer provides a reliable, synergistic motor to restore satisfactory gross grip function.
POSTOPERATIVE REHABILITATION PROTOCOLS
The success of any secondary flexor tendon repair or reconstruction is inextricably linked to the postoperative rehabilitation protocol. The goal is to apply enough controlled stress to stimulate intrinsic tendon healing and encourage longitudinal collagen alignment, while preventing gap formation or rupture.
Early Passive Motion (Modified Duran Protocol)
- Splinting: A dorsal blocking splint is applied immediately postoperatively. The wrist is positioned in 20-30 degrees of flexion, MCP joints in 50-70 degrees of flexion, and IP joints in neutral extension.
- Exercises: The patient performs controlled passive flexion and active extension within the constraints of the dorsal block. This promotes tendon gliding (excursion) to prevent dense peritendinous adhesions.
Early Active Motion Protocols
For robust repairs (4-strand or 6-strand core sutures combined with an epitendinous repair) or secure tendon grafts, early active motion protocols may be initiated.
* Place and Hold: The therapist passively flexes the digits, and the patient gently contracts the flexor muscles to "hold" the position.
* True Active Motion: Light, unresisted active flexion is initiated under strict supervision, typically starting at 3 to 5 days postoperatively.
Pitfall: Overly aggressive early active motion in a delayed repair or minigraft setting can lead to silent elongation of the repair site or catastrophic rupture. The tensile strength of a healing tendon drops significantly between days 5 and 21 (the inflammatory and early fibroblastic phases). Progression of therapy must be meticulously tailored to the specific surgical technique utilized.
CONCLUSION
Secondary repair and reconstruction of flexor tendons demand a profound understanding of hand biomechanics, precise surgical execution, and rigorous patient compliance. Whether performing a delayed primary repair, a Wagner profundus advancement, or a complex single-stage tendon graft, the surgeon must respect the delicate balance between tendon tension and joint mobility. By adhering to established prerequisites and employing meticulous tissue handling, excellent functional restoration can be achieved even in the chronically injured hand.
===END===
You Might Also Like