Masterclass in Tendon Transfers for Thumb Intrinsic Dysfunction: Modified Royle-Thompson and EIP Techniques
Key Takeaway
The modified Royle-Thompson transfer utilizes the ring finger flexor digitorum superficialis to restore thumb adduction and opposition in intrinsic paralysis. By splitting the tendon and routing it to the extensor pollicis longus and adductor pollicis, surgeons can recreate a dynamic pinch. This guide details the biomechanics, step-by-step surgical technique, and postoperative rehabilitation for the Royle-Thompson, extensor indicis proprius, and abductor pollicis longus tendon transfers.
BIOMECHANICS OF THUMB INTRINSIC PARALYSIS
The human thumb relies on a delicate, highly coordinated balance between extrinsic and intrinsic musculature to achieve circumduction, opposition, and powerful key pinch. In the setting of ulnar nerve palsy, low median nerve palsy, or combined lesions, the loss of intrinsic muscle function—specifically the adductor pollicis, the first dorsal interosseous (FDI), and the opponens pollicis—results in profound functional impairment.
Patients typically present with a weakened key pinch, compensatory interphalangeal (IP) joint hyperflexion driven by the flexor pollicis longus (Froment’s sign), and metacarpophalangeal (MCP) joint hyperextension (Jeanne’s sign). To restore the complex biomechanical vectors required for a stable pinch, orthopedic surgeons employ highly specific tendon transfers. The modified Royle-Thompson transfer and the Extensor Indicis Proprius (EIP) transfer remain cornerstone procedures for re-establishing the adduction moment arm and stabilizing the index finger against the thumb.
Clinical Pearl: Tendon transfers do not create new strength; they redistribute existing power. A transferred muscle will typically lose one grade of motor strength (Medical Research Council scale) following transposition. Therefore, only muscles with a preoperative strength of Grade 4 or 5 should be selected as donors.
THE MODIFIED ROYLE-THOMPSON TRANSFER
The original Royle-Thompson transfer was designed to restore thumb opposition. The modern modified technique utilizes the flexor digitorum superficialis (FDS) of the ring finger. The FDS is an ideal donor due to its excellent excursion (approximately 50 mm), robust cross-sectional area, and the minimal functional deficit incurred by the donor digit, provided the flexor digitorum profundus (FDP) remains intact.
By splitting the FDS tendon into two slips, the surgeon can simultaneously address two biomechanical deficits: restoring the adduction vector at the first metacarpal and stabilizing the MCP joint to prevent the hyperextension characteristic of Jeanne's sign.
Preoperative Planning and Patient Positioning
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) combined with intravenous sedation, or general anesthesia.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg (or 100 mm Hg above systolic blood pressure) after exsanguination with an Esmarch bandage.
- Preparation: Standard surgical prep and drape from the fingertips to the mid-arm.
Surgical Technique: Step-by-Step
1. Harvesting the Flexor Digitorum Superficialis (FDS)
- Make a midlateral incision over the ulnar aspect of the ring finger. This approach avoids the volar tactile surface and minimizes flexion contracture risks.
- Carefully dissect through the subcutaneous tissue to expose the flexor tendon sheath.
- Incise the sheath, taking care to preserve the critical A2 and A4 pulleys to prevent postoperative bowstringing of the remaining FDP tendon.
- Identify the FDS tendon. Free its insertion from the middle phalanx. The FDS bifurcates at Camper's chiasm; ensure both slips of the insertion are sharply detached.
2. Proximal Retrieval and Tendon Preparation
- Make a short transverse incision in the mid-palm, following the distal palmar crease to ensure a cosmetically acceptable scar.
- Identify the FDS tendon of the ring finger within the palmar wound.
- Apply gentle traction to the distal stump in the finger and withdraw the tendon proximally out of the palm through the transverse incision.
- Using a scalpel, meticulously split the harvested FDS tendon longitudinally into two equal slips along its length.
3. Preparation of the Recipient Site
- Make a curved incision on the dorsoradial aspect of the thumb, similar to the approach described for a Riordan transfer. The incision should allow adequate exposure of the extensor pollicis longus (EPL) tendon and the adductor pollicis insertion.
- Create a wide, generous subcutaneous tunnel from the palmar incision to the dorsoradial thumb incision.
- Surgical Warning: The tunnel must be strictly subcutaneous and wide enough to allow frictionless gliding of the transferred tendon. Constriction within the tunnel is a primary cause of transfer failure.
4. Routing and Fixation
- Pass both slips of the split FDS tendon radially through the subcutaneous tunnel into the thumb incision.
- Slip 1 (EPL Fixation): Suture the first slip to the extensor pollicis longus (EPL) tendon distal to the metacarpophalangeal joint. This vector acts as a dynamic tenodesis to prevent MCP hyperextension and IP hyperflexion during pinch.
- Slip 2 (Adductor Fixation): Tunnel the second slip dorsally over the first metacarpal. Suture it securely on the ulnar side of the thumb to the tendinous insertion of the adductor pollicis. This restores the primary adduction moment arm.
- Set the tension with the wrist in neutral, the thumb in full adduction, and the MCP joint in slight flexion. Use a Pulvertaft weave or multiple figure-of-eight sutures with 3-0 non-absorbable braided suture for robust fixation.
Postoperative Care Protocol
- Immobilization (0-3 Weeks): Close the wounds in layers. Apply a bulky, non-compressive dressing followed by a rigid, forearm-based thumb spica splint. The splint must hold the thumb in adduction and the wrist in moderate flexion (approximately 30 degrees) to remove tension from the transfer.
- Early Mobilization (3-6 Weeks): At 3 weeks postoperatively, the static splint is removed. Active range-of-motion exercises are initiated under the guidance of a certified hand therapist.
- Protection: Between exercise sessions, the patient must wear a removable, protective forearm-based thumb spica splint that specifically prevents thumb hyperextension for an additional 3 weeks.
- Strengthening (6+ Weeks): Progressive resistance and pinch strengthening begin at 6 weeks, with full unrestricted activity typically permitted by 10 to 12 weeks.
TRANSFER OF THE EXTENSOR INDICIS PROPRIUS (EIP) TENDON
In the paralytic hand, restoring thumb adduction is only half the battle. The index finger must provide a stable, rigid post against which the thumb can pinch. This stability is normally provided by the first dorsal interosseous (FDI) muscle, which abducts the index finger and flexes its MCP joint. When the FDI is paralyzed, the index finger drifts ulnarly during pinch, severely compromising grip strength.
The Extensor Indicis Proprius (EIP) transfer is the gold standard for restoring FDI function. The EIP has an appropriate line of pull, adequate excursion, and its harvest leaves the index finger with independent extension via the extensor digitorum communis (EDC).
Surgical Technique: Step-by-Step
1. Incision and Exposure
- Begin a curved incision at the midlateral point on the radial side of the index finger proximal phalanx.
- Carry the incision proximally over the radial aspect of the metacarpophalangeal joint.
- Curve the incision dorsally to end at the middle of the second metacarpal.
2. Tendon Harvest and Elongation
- Identify the EIP tendon over the dorsum of the hand. It is consistently located ulnar and deep to the EDC tendon of the index finger.
- To add critical length to the EIP tendon, elevate a small, rectangular flap of the dorsal extensor expansion over the metacarpophalangeal joint where it attaches to the insertion of the tendon.
- Withdraw the tendon proximally into the dorsal wound.
- Crucial Step: Meticulously close the resulting defect in the extensor expansion with 4-0 absorbable sutures to prevent postoperative extensor lag or subluxation of the EDC tendon.
3. Routing and Fixation
- Free the EIP tendon throughout the proximal wound to ensure unrestricted excursion.
- Pass the tendon radially in a gentle, sweeping subcutaneous curve toward the base of the index finger.
- Identify the tendinous insertion of the paralyzed first dorsal interosseous muscle.
- Roughen the surface of the FDI tendon to promote biological healing.
- Securely suture the transferred EIP tendon to the FDI tendon using a weave technique under appropriate tension (index finger in full radial abduction and slight MCP flexion).
ABDUCTOR POLLICIS LONGUS (APL) TRANSFER FOR FIRST DORSAL INTEROSSEOUS REPLACEMENT (NEVIASER TECHNIQUE)
When the EIP is unavailable or contraindicated, the Abductor Pollicis Longus (APL) transfer, as described by Neviaser, Wilson, and Gardner, serves as an excellent alternative for restoring first dorsal interosseous function. The APL frequently possesses multiple accessory slips inserting into the trapezium or thenar fascia, making it an ideal donor that does not compromise primary thumb abduction.
Surgical Technique and Image Integration
Biomechanical Advantage: The APL transfer provides a robust, powerful vector that closely mimics the native FDI. Because the APL is already a thumb motor, cortical re-education for pinch is often faster than with an EIP transfer.
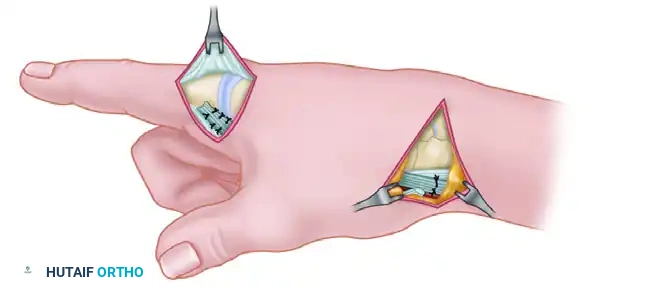
Step 1: Harvesting the Accessory Slip
Identify the first dorsal compartment. The APL typically has a functional slip inserting into the base of the first metacarpal and one or more accessory slips inserting into the trapezium.
Figure A: The accessory slip inserting into the trapezium is sharply detached distal to the extensor retinaculum. The primary functional slip, inserting into the first metacarpal, is carefully preserved to maintain native thumb abduction.
Step 2: Tunnel Creation
Once the accessory slip is mobilized, a pathway must be created to redirect its line of pull toward the index finger.
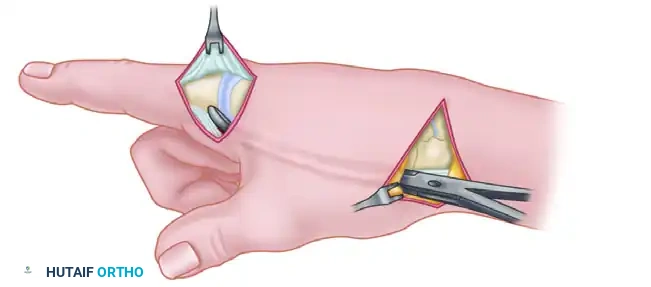
Figure B: A wide subcutaneous tunnel is created using blunt dissection from the radial styloid across the first web space to the tendinous insertion of the first dorsal interosseous on the radial aspect of the index finger.
Step 3: Grafting and Fixation
Because the accessory slip of the APL is often too short to reach the FDI insertion directly, a free tendon graft (commonly the palmaris longus) is required to bridge the defect.
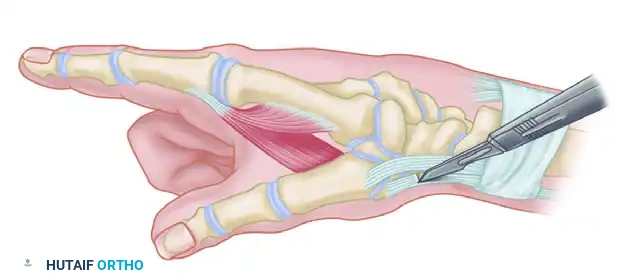
Figure C: The free tendon graft is meticulously woven into the native tendon of the first dorsal interosseous distally, passed through the subcutaneous tunnel, and sutured to the mobilized accessory slip of the APL proximally under appropriate tension.
MANAGEMENT OF THE UNSTABLE THUMB METACARPOPHALANGEAL JOINT
Tendon transfers rely on stable skeletal foundations. If the thumb metacarpophalangeal joint exhibits global instability, fixed hyperextension deformity, or advanced degenerative joint disease (DJD), soft tissue transfers alone will fail to provide a powerful pinch.
In these scenarios, arthrodesis of the thumb MCP joint is strictly indicated. Fusion is typically performed at 10 to 15 degrees of flexion and slight pronation.
Surgical Pearl: If fusion of the thumb MCP joint is necessary, the extensor pollicis brevis (EPB) tendon becomes functionally redundant. Rather than discarding it, the EPB tendon can be harvested and transferred to the first dorsal interosseous to restore index finger abduction, thereby sparing the EIP or APL.
COMPLICATIONS AND PITFALLS IN TENDON TRANSFERS
To achieve mastery in tendon transfer surgery, the orthopedic surgeon must anticipate and mitigate potential complications:
- Improper Tensioning: The most common cause of transfer failure. A transfer set too loose will fail to generate sufficient force (due to the Blix curve of muscle length-tension). A transfer set too tight may cause joint contractures or undergo ischemic necrosis.
- Adhesions: Rough handling of the tendon, inadequate hemostasis, or failure to create a wide subcutaneous tunnel will lead to restrictive adhesions. Always handle tendons with moist sponges and avoid crushing forceps.
- Donor Site Morbidity: Harvesting the FDS can occasionally lead to a swan-neck deformity or PIP joint stiffness in the donor digit. Preserving the FDP and initiating early, controlled mobilization mitigates this risk.
- Extensor Lag: When harvesting the EIP, failure to meticulously repair the extensor hood over the index MCP joint will result in a noticeable extensor lag and potential ulnar subluxation of the EDC tendon.
By adhering to strict biomechanical principles, executing meticulous surgical technique, and enforcing rigorous postoperative rehabilitation, the modified Royle-Thompson and EIP tendon transfers reliably restore functional pinch and opposition to the paralytic hand.
You Might Also Like

