
Comprehensive Introduction and Patho-Epidemiology
Obtaining adequate anterior exposure of the knee joint can present a formidable challenge using standard surgical approaches during revision total knee arthroplasty (TKA). As the complexity of revision arthroplasty increases—often involving massive bone loss, severe arthrofibrosis, retained bulky hardware, and altered joint lines—the demand for extensile exposure techniques becomes paramount. While a standard medial parapatellar arthrotomy is sufficient for primary arthroplasty and straightforward revisions, the presence of dense adhesions and fibrosis within the extensor mechanism often restricts patellar eversion and severely limits visualization. The inability to safely translate or evert the patella places the patellar tendon insertion at extreme risk for iatrogenic avulsion, a catastrophic complication that significantly compromises postoperative function.
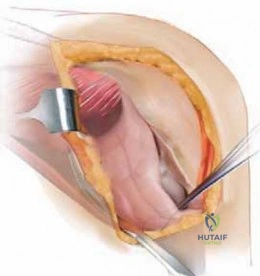

The options available for managing difficult exposure in revision scenarios include the extensor mechanism snip (typically performed 5 to 8 cm proximal to the superior pole of the patella), the V-Y quadriceps turndown, and the tibial tubercle osteotomy (TTO). Among these, the tibial tubercle osteotomy has emerged as a highly reliable and reproducible technique to obtain extensile exposure of the knee during difficult revision procedures. Unlike soft-tissue-only exposures, the TTO mobilizes the distal attachment of the extensor mechanism, allowing the entire quadriceps-patella-tendon complex to be retracted laterally as a single, continuous unit.


Epidemiologically, the requirement for an extensile exposure in revision total knee arthroplasty is reported in approximately 10 to 15 percent of cases, with higher utilization rates observed in tertiary referral centers managing complex periprosthetic joint infections, severe stiffness, and massive component extractions. The natural history of attempting to bypass an extensile exposure in a stiff knee is fraught with risk. Inadequate exposure combined with continued forceful retraction of the extensor mechanism dramatically increases the risk of avulsion of the patellar ligament from the tibial tubercle. Avulsion of the patellar ligament necessitates complex reconstruction, results in prolonged immobilization, frequently leads to a persistent extensor lag, and ultimately yields a poor functional outcome.


The incidence of revision total knee arthroplasty continues to rise globally, driven by an aging population and the expansion of primary arthroplasty indications to younger, more active patients. Consequently, the absolute number of cases requiring extensile exposures is increasing. The tibial tubercle osteotomy is particularly advantageous in this epidemiological landscape because it relies on bone-to-bone healing. Bone-to-bone healing is generally more robust, predictable, and allows for earlier postoperative rehabilitation compared to tendinous repairs, which are prone to stretching, attenuation, or outright failure under cyclic loading.
The Burden of Revision Arthroplasty and Exposure Challenges
The sheer volume of primary total knee arthroplasties performed annually has created a proportional, if not exponential, increase in revision burdens. Data extracted from national joint registries indicate that aseptic loosening, periprosthetic joint infection (PJI), instability, and arthrofibrosis represent the primary indications for revision surgery. In the setting of PJI, patients frequently undergo multiple surgical interventions, including irrigation and debridement, articulating or static spacer placement, and eventual reimplantation. Each successive surgical intervention exacerbates the formation of dense, unyielding scar tissue within the suprapatellar pouch and the medial and lateral gutters.

This obliteration of the normal anatomic gliding planes results in secondary patella baja or functional shortening of the extensor mechanism. When the surgeon attempts to flex the knee to 90 degrees or more to access the posterior compartment or to deliver the tibia anteriorly for explantation of well-fixed stems, the tension placed on the patellar tendon insertion increases exponentially. The tibial tubercle osteotomy directly addresses this mechanical limitation by mobilizing the insertion site itself, thereby converting a high-tension environment into a manageable, tension-free surgical field.


Furthermore, the extraction of well-fixed, long-stemmed tibial components or metaphyseal sleeves often requires direct, inline access to the tibial canal. A rigid extensor mechanism blocks this trajectory, forcing the surgeon to work at an angle, which increases the risk of iatrogenic cortical perforation or fracture. By mobilizing the tubercle laterally, the surgeon gains an unimpeded, collinear view down the anatomical axis of the tibia, facilitating the safe use of extraction tools, flexible osteotomes, and ultrasonic devices.
Historical Context and Evolution of Extensile Exposures
The historical evolution of extensile exposures in knee arthroplasty reflects a continuous search for the optimal balance between surgical access and postoperative extensor mechanism competence. Early techniques, such as the Coonse-Adams approach and the V-Y quadriceps turndown, provided excellent exposure but were plagued by high rates of postoperative extensor lag, prolonged rehabilitation requirements, and unpredictable soft-tissue healing. These soft-tissue procedures inherently violate the extensor mechanism's continuity, relying entirely on scar tissue and suture strength during the critical early phases of healing.

The concept of osteotomizing the tibial tubercle to facilitate knee exposure was initially described by Dolin in 1983 for use in difficult primary arthroplasties. Dolin's early technique involved a relatively short osteotomy fragment, which, while effective for exposure, presented challenges regarding rigid internal fixation and union. It was subsequently modified, refined, and popularized for routine use in revision total knee arthroplasty by Whiteside in the mid-1990s. Whiteside's critical modification was the extension of the osteotomy to include a longer segment of the tibial crest (typically 8 to 10 centimeters), which drastically increased the surface area for bone-to-bone healing and allowed for robust bicortical wire or screw fixation.


Today, the Whiteside modification remains the gold standard for tibial tubercle osteotomies in revision TKA. The procedure's evolution has been further refined by an enhanced understanding of the lateral soft-tissue hinge. Preserving the lateral periosteum and the muscular attachments of the anterior compartment prevents the osteotomized fragment from becoming a free, avascular bone graft. This pivotal technical nuance has reduced the historical rates of nonunion and fragment necrosis, solidifying the TTO as the preferred extensile exposure among contemporary adult reconstruction surgeons.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the extensor mechanism anatomy, the local vascular supply, and the biomechanical forces acting upon the proximal tibia is an absolute prerequisite for the successful execution of a tibial tubercle osteotomy. The extensor mechanism of the knee is a complex functional unit comprising the quadriceps muscle group, the quadriceps tendon, the patella, the patellar retinaculum, the patellar ligament, and the tibial tubercle. Altering this mechanism requires meticulous precision to ensure that its mechanical integrity is restored postoperatively.

Osseous Anatomy of the Proximal Tibia and Tubercle
The tibial tubercle is a prominent apophyseal elevation situated on the anterior aspect of the proximal tibia, serving as the distal attachment site for the patellar ligament. Morphologically, the proximal tibia transitions from a broad, cancellous metaphyseal region to a dense, cortical diaphyseal region. The tibial tubercle osteotomy must be meticulously planned to incorporate a sufficient volume of cancellous bone proximally to facilitate rapid osseous union, while simultaneously preserving enough cortical bone distally to allow for rigid internal fixation.
The dimensions of the osteotomy are critical. A fragment that is too short (less than 5 cm) lacks the necessary surface area for reliable healing and is prone to proximal migration under the immense pull of the quadriceps. Conversely, a fragment that is too thin risks fracturing during mobilization or during the insertion of fixation screws. The ideal osteotomy is typically 8 to 10 cm in length, 2 cm in width, and at least 1 to 1.5 cm in depth, tapering smoothly into the anterior tibial crest distally to avoid creating a sharp stress riser that could precipitate a postoperative tibia fracture.


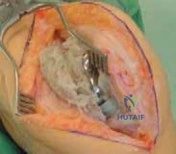
The relationship of the tibial tubercle to Gerdy's tubercle (the insertion site of the iliotibial band) must also be respected. The osteotomy is typically directed from medial to lateral, stopping just short of the lateral cortex to preserve the periosteal hinge. The surgeon must be cognizant of the proximal tibial anatomy, particularly the metaphyseal flare, to ensure the oscillating saw or osteotome does not inadvertently violate the lateral cortex, which would detach the lateral soft-tissue tether and destabilize the fragment.
Vascular Supply and Soft Tissue Envelopes
The vascular network supporting the anterior knee and the extensor mechanism is derived from the genicular anastomotic ring. The superior medial, superior lateral, inferior medial, and inferior lateral genicular arteries form a rich plexus around the patella and the proximal tibia. In the setting of revision arthroplasty, this vascular network is frequently compromised due to prior surgical incisions, extensive soft tissue stripping, and the utilization of a pneumatic tourniquet.

The anterior tibial recurrent artery provides substantial blood flow to the anterior proximal tibia and the region of the tibial tubercle. When performing a tibial tubercle osteotomy, the surgeon must balance the need for adequate exposure with the imperative to preserve blood supply. The lateral border of the tibial tubercle serves as the attachment site for the anterior compartment musculature, predominantly the tibialis anterior muscle. The deep fascia covering this musculature is continuous with the periosteum of the lateral tibia.

Preserving this lateral periosteal and muscular hinge during the osteotomy is a critical technical maneuver. This hinge not only provides a robust vascular supply to the osteotomized bone fragment but also acts as a mechanical tether, preventing catastrophic lateral or proximal displacement of the fragment during patellar eversion and subsequent knee flexion. Complete detachment of the osteotomized fragment from its lateral soft tissue attachments converts the segment into a free avascular bone graft, dramatically increasing the risk of nonunion, fragmentation, and subsequent failure of the extensor mechanism.
Biomechanics of the Extensor Mechanism
The extensor mechanism operates as a dynamic pulley system, with the patella acting as a fulcrum to increase the moment arm of the quadriceps muscle group. The forces transmitted through the patellar tendon to the tibial tubercle are immense, frequently exceeding multiple times the patient's body weight during activities such as stair climbing or rising from a seated position. These biomechanical realities dictate that any disruption of the tibial tubercle must be repaired with a construct capable of withstanding significant cyclic tensile loading.


During revision arthroplasty in a stiff knee, attempting to forcefully flex the joint beyond its soft-tissue limits concentrates extreme tensile stress directly on the patellar tendon insertion. If the tendon avulses, the extensor mechanism is functionally destroyed. The TTO mitigates this risk by shifting the point of mobility from the tendinous insertion to a large osseous flap. When the knee is flexed after a TTO, the tubercle fragment simply hinges laterally and proximally, entirely dissipating the tension on the patellar tendon.
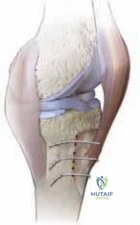
Postoperatively, the fixation of the TTO must adhere to the principles of absolute stability to promote primary bone healing. The construct—typically utilizing cortical screws or heavy-gauge cerclage wires—must compress the osteotomy site and neutralize the proximal shear forces generated by the quadriceps. If the fixation is inadequate, the cyclic loading of early rehabilitation will lead to micromotion, fibrous nonunion, and proximal migration of the tubercle fragment, resulting in a profound and often irreversible extensor lag.
Exhaustive Indications and Contraindications
The decision to perform a tibial tubercle osteotomy should not be made lightly. While it is an incredibly powerful tool in the revision arthroplasty armamentarium, it carries specific risks and requires meticulous technique. The surgeon must carefully weigh the necessity of extensile exposure against the patient's biological capacity for bone healing and compliance with postoperative rehabilitation protocols.


Primary Indications for Tibial Tubercle Osteotomy
The primary indication for a TTO is the inability to achieve adequate surgical exposure of the knee joint without placing the patellar tendon at imminent risk of avulsion. This scenario is most frequently encountered in the setting of severe arthrofibrosis, where the suprapatellar pouch is obliterated, and the medial and lateral gutters are scarred down. In such cases, the patella becomes functionally tethered to the anterior femur, preventing eversion or even lateral subluxation.
Another major indication is the presence of patella baja (infera), either primary or secondary to previous surgeries. In patella baja, the absolute length of the patellar tendon is shortened, drastically reducing the arc of motion available before tension limits further flexion. A TTO allows the surgeon to not only gain exposure but also potentially proximalize the tubercle during fixation to correct the patella baja, thereby restoring more normal patellofemoral kinematics.

Additionally, TTO is highly indicated when massive component extraction is required. Removing well-fixed, fully porous-coated or cemented long tibial stems necessitates direct, inline access to the tibial diaphysis. Attempting to lever extraction instruments around an intact extensor mechanism frequently results in posterior cortical blowout or anterior tibial crest fractures. The TTO clears the anterior access portal, allowing the surgeon to work safely down the anatomical axis of the tibia.
Absolute and Relative Contraindications
While highly versatile, the TTO is not universally applicable. Absolute contraindications include the presence of an active, untreated local soft-tissue infection overlying the anterior tibia, as placing hardware into an infected bed guarantees treatment failure. Similarly, a severely compromised anterior soft-tissue envelope—such as thin, irradiated skin or previous rotational muscle flaps covering the proximal tibia—precludes the safe execution of a TTO, as the surgical trauma will likely result in catastrophic wound breakdown and exposed bone.


Relative contraindications include severe osteopenia or osteoporosis, where the structural integrity of the proximal tibia is insufficient to hold cortical screws or cerclage wires. In such osteoporotic bone, the hardware may simply pull through the cortex under the tension of the quadriceps, leading to fixation failure. A history of prior high tibial osteotomy (HTO) or proximal tibial fractures can also complicate a TTO, as the altered local anatomy and preexisting hardware tracts may compromise the creation of a robust osteoperiosteal flap.
Furthermore, patient non-compliance is a significant relative contraindication. The success of a TTO relies heavily on strict adherence to phased postoperative rehabilitation, particularly regarding weight-bearing restrictions and limitations on active knee extension. Patients with severe cognitive impairment or those who are unable or unwilling to follow complex rehabilitation protocols are at an unacceptably high risk for early mechanical failure of the osteotomy.
| Indication / Contraindication Parameter | Specific Clinical Scenarios | Rationale |
|---|---|---|
| Primary Indications | Severe Arthrofibrosis, Patella Baja, PJI Two-Stage Exchange | Tension-free exposure, prevention of patellar tendon avulsion, access for massive hardware extraction. |
| Mechanical Indications | Well-fixed long tibial stems, Metaphyseal sleeves/cones | Requires inline, collinear access to the tibial diaphysis to prevent iatrogenic cortical blowout. |
| Absolute Contraindications | Active anterior soft-tissue infection, Prior local radiation | High risk of wound necrosis, exposed hardware, and failure of osseous union. |
| Relative Contraindications | Severe Osteoporosis, Prior proximal tibial fracture/HTO | Poor bone stock limits rigid internal fixation; altered anatomy complicates osteotomy execution. |
| Patient Factors | Severe cognitive impairment, Non-compliance | Inability to adhere to strict postoperative brace and weight-bearing protocols leads to mechanical failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful revision TKA requiring a tibial tubercle osteotomy. The surgeon must anticipate the need for an extensile exposure well before the initial incision is made. Reactive, poorly planned osteotomies performed in the heat of a difficult exposure are prone to technical errors, such as inadequate fragment length or violation of the lateral hinge.

Clinical and Radiographic Evaluation
The clinical evaluation must focus on the patient's current range of motion, the presence of extensor lag, and a detailed assessment of the soft-tissue envelope. Previous surgical incisions must be mapped, and the mobility of the skin over the anterior tibia assessed. A rigid, immobile knee with extensive anterior scarring should immediately alert the surgeon to the high probability that a TTO will be required.

Radiographic evaluation must include weight-bearing anteroposterior (AP), lateral, and skyline (Merchant or sunrise) views of the knee. The lateral radiograph is critical for assessing patellar height using indices such as the Insall-Salvati ratio or the Caton-Deschamps index. The presence of patella baja strongly supports the preemptive planning of a TTO. Additionally, the lateral radiograph allows the surgeon to evaluate the anterior bone stock of the proximal tibia, ensuring there is sufficient depth to create a robust osteotomy fragment.
In complex revisions involving massive bone loss or distorted anatomy, a computed tomography (CT) scan with metal artifact reduction sequence (MARS) is invaluable. The CT scan provides a three-dimensional understanding of the tibial bone stock, the exact location of existing hardware, and the presence of osteolysis behind the tibial tubercle, which could compromise the fixation of the osteotomy.
Digital Templating and Pre-Operative Strategy
Digital templating is essential for predicting the size and position of the revision components and for planning the level and length of the TTO. The surgeon must template the anticipated length of the new tibial stem to ensure that the distal extent of the TTO does not terminate exactly at the tip of the stem. A stress riser created by the convergence of the osteotomy apex and the stem tip dramatically increases the risk of a postoperative periprosthetic tibial fracture.































