Flexor Tendon Repair in Zones III, IV, and V: Surgical Guide

Key Takeaway
Flexor tendon injuries in Zones III, IV, and V present unique anatomical and biomechanical challenges. Successful outcomes depend on meticulous surgical technique, accurate identification of neurovascular structures, and appropriate postoperative rehabilitation. This guide details the step-by-step surgical approaches, suture configurations, and evidence-based mobilization protocols—including Kleinert and Duran techniques—required to optimize tendon gliding, prevent bowstringing, and restore functional hand mechanics in complex volar lacerations.
INTRODUCTION TO PROXIMAL FLEXOR TENDON INJURIES
Flexor tendon lacerations occurring proximal to the fibro-osseous digital sheath—specifically in Zones III (the palm), IV (the carpal tunnel), and V (the volar forearm)—present a distinct set of anatomical and surgical challenges compared to the notorious "no man's land" of Zone II. While the absence of a tight, restrictive flexor tendon sheath in these proximal zones generally portends a more favorable prognosis for tendon gliding and functional recovery, the dense concentration of neurovascular structures and the frequent multiplicity of injured tendons demand meticulous surgical precision.
The primary goals of repair in these zones are to restore the precise anatomical continuity of the musculotendinous units, prevent postoperative bowstringing, and institute early controlled mobilization to mitigate adhesion formation while protecting the integrity of the repair.
REPAIR IN ZONE III: THE PALM
Zone III encompasses the anatomical region between the distal edge of the transverse carpal ligament (TCL) and the proximal margin of the A1 pulley. This area houses the lumbrical origins from the flexor digitorum profundus (FDP) tendons and the superficial palmar arch.
Surgical Approach and Tendon Retrieval
Flexor tendon repair in Zone III is performed in a manner biomechanically similar to Zone II repairs, though the spatial constraints are less severe.
- Incision Management: Primary traumatic wounds rarely provide adequate exposure for a robust repair. Incisions must be extended proximally and distally. It is imperative to utilize Bruner zigzag or mid-lateral extensions, strictly avoiding crossing flexion creases at right angles to prevent subsequent flexion contractures.
- Neurovascular Protection: The superficial palmar arch and the common digital nerves are highly vulnerable in this zone. Skin flaps must be elevated with full-thickness subcutaneous tissue to avoid devascularization.
- Tendon Retrieval: Achieve proper orientation of the tendon before repair. Due to the proximal pull of the flexor muscle bellies, severed tendons frequently retract into the carpal tunnel or distal forearm. If blind retrieval using a pediatric feeding tube or flexible retriever fails, a partial release of the transverse carpal ligament may be required to deliver the proximal stumps distally into the palm.
Suture Configuration and Repair Technique
Although the restrictive fibro-osseous flexor sheath is not involved in the palm, meticulous suture technique remains paramount.
🔪 Surgical Pearl: Lumbrical Management
Avoid incorporating the lumbrical muscle belly into the FDP repair. Tethering the lumbrical can lead to a "lumbrical plus" syndrome, characterized by paradoxical extension of the interphalangeal joints during attempted active finger flexion.
- Core Suture Placement: It is highly recommended to utilize an intratendinous core suture (e.g., a 4-strand or 6-strand modified Kessler or cruciate configuration) in the palm. This minimizes the exposure of suture material and raw tendon edges to adjacent structures, thereby reducing the risk of dense adhesions to the lumbricals or palmar fascia.
- Epitendinous Repair: A running 6-0 monofilament epitendinous suture should be added to smooth the repair site and increase the biomechanical yield strength of the construct.
Satisfactory healing and excellent functional results are generally expected after isolated Zone III repairs, provided that early mobilization protocols are instituted.
REPAIR IN ZONE IV: THE CARPAL TUNNEL
Zone IV represents the area confined within the carpal tunnel. An injury directly to the base of the palm in this zone almost invariably involves the median nerve due to its superficial and central location beneath the TCL.
Diagnostic Considerations
If a volar laceration occurs just proximal to the wrist flexion crease, the surgeon must maintain a high index of suspicion for a Zone IV flexor tendon injury. This is especially true if the patient's fingers were tightly flexed into a fist at the moment of injury; the distal tendon stumps will glide distally into the palm once the fingers are extended, masking the true level of the tendon laceration.
Surgical Approach and Transverse Carpal Ligament Management
- Incision Extension: Extend the laceration distally into the palm and proximally into the forearm, taking care to cross the wrist flexion creases obliquely.
- TCL Release: If the laceration occurs directly beneath the transverse carpal ligament, partial or complete release of the TCL is usually required to gain adequate exposure and retrieve retracted tendons.
🚨 Surgical Warning: Prevention of Bowstringing
Complete, unrepaired release of the transverse carpal ligament in the setting of multiple flexor tendon repairs can lead to severe postoperative bowstringing of the flexor tendons, significantly reducing mechanical advantage and grip strength.
- Z-Lengthening: If the TCL cannot be preserved intact, it should be released in a Z-lengthening or step-cut configuration. This allows for a lengthened repair at the conclusion of the procedure, accommodating postoperative edema while maintaining a retinacular restraint against bowstringing.
Tendon Identification and Repair
In the carpal tunnel, ensuring the proper orientation and location of individual tendons is critical.
* Anatomical Arrangement: Recall the standard anatomical arrangement of the flexor digitorum superficialis (FDS) tendons within the carpal tunnel: the tendons to the middle and ring fingers lie superficial to the tendons of the index and small fingers.
* Suture Technique: Repair the FDP and FDS tendons using an intratendinous locking core suture. This holds the tendons securely with minimal exposure of the cut surface.
* Tenosynovectomy: A partial tenosynovectomy may be required to diminish the bulky, edematous tissue that inevitably follows multiple tendon repairs within the tight confines of the carpal tunnel.
REPAIR IN ZONE V: THE VOLAR FOREARM
Zone V encompasses the volar forearm proximal to the transverse carpal ligament up to the musculotendinous junctions. Major lacerations in this area—often resulting from broken glass, industrial accidents, or violent altercations—frequently result in the division of multiple tendons, nerves, and vessels, a clinical scenario classically termed the "spaghetti wrist."
Anatomical Identification and Matching
In Zone V, the sheer volume of severed structures makes accurate identification the most critical and time-consuming step of the procedure.
- Group Retrieval: Because of their common muscle origins, when the FDS and FDP tendons are divided at the wrist, they can often be delivered into the wound as a group by finding and pulling distally on one identified tendon.
- Matching Ends: Properly match the tendon ends by paying careful attention to:
- Their location and level in the wound.
- Their relationship to neighboring structures.
- Their cross-sectional diameters and shapes.
- The specific angle and bevel of the laceration through each tendon.
🔪 Surgical Pearl: Nerve vs. Tendon Identification
It is not a disgrace to open an anatomical atlas in the operating room to confirm relationships; however, it is an inexcusable technical error to anastomose the median nerve to the flexor pollicis longus (FPL), the palmaris longus, or an FDS tendon.
- Median Nerve Identification: The proximal and distal ends of the median nerve can usually be identified by their appropriate anatomical location, their slightly yellowish hue (compared to the pearly white of tendons), the presence of a longitudinal volar midline epineural vessel, and the distinct nerve fascicles visible on the severed cross-section.
Repair Hierarchy and Suture Selection
- Suture Caliber: While 4-0 sutures are standard in the palm and digits, 3-0 nylon or braided synthetic sutures may be sufficient and appropriate for suturing the larger muscle-tendon units in the distal forearm.
- Configuration: Repairs performed in the proximal forearm (near the musculotendinous junction) do not absolutely require a complex intratendinous core repair. A double right-angled (e.g., Krackow) or robust mattress suture configuration is often satisfactory in the muscular forearm.
- Order of Repair: Work systematically from deep to superficial. Repair the deep flexors (FDP, FPL), followed by the superficial flexors (FDS). Once the biomechanical tendon repairs are complete, proceed to the microsurgical repair of the nerves (median, ulnar) and vessels (radial, ulnar arteries), ensuring that the manipulation required for tendon repair does not disrupt delicate microvascular anastomoses.
PEDIATRIC CONSIDERATIONS IN FLEXOR TENDON REPAIR
The diagnosis of tendon and associated neurovascular injuries is notoriously difficult in children, as clinical examination is often unreliable due to pain and anxiety.
- Surgical Technique: Because of the extremely small tolerances between the flexor sheath and flexor tendons in pediatric patients, meticulous, atraumatic technique is mandatory. Finer sutures are required; 5-0 core sutures and 6-0 or 7-0 monofilament sutures for the circumferential epitendinous repair are standard.
- Immobilization: Very young children lack the cognitive ability to cooperate with complex postoperative early mobilization programs. Therefore, immobilization is more extensive and prolonged. This frequently requires the use of a long-arm cast extending to the axilla, with the elbow flexed to 90 degrees, the wrist flexed, and the fingers positioned in 50 to 60 degrees of MCP flexion with full interphalangeal extension.
- Outcomes: Studies indicate that the specific postoperative regimen has less effect on the final outcome in young children compared to adults. Total active motion correlates best with age at the time of injury: children older than 10 years regain the most motion (approx. 82%), compared with children 4 to 10 years of age (77%), and children younger than 4 years (54%).
POSTOPERATIVE CARE AND REHABILITATION PROTOCOLS
The ultimate success of a flexor tendon repair relies as much on the postoperative rehabilitation protocol as it does on the surgical execution. The goal is to apply enough controlled stress to the tendon to promote intrinsic healing and prevent restrictive adhesions, without exceeding the tensile strength of the repair.
Excellent results can be achieved using established postoperative mobilization techniques, primarily categorized into active extension/passive flexion (Kleinert) and controlled passive motion (Duran).
The Kleinert Protocol (Dynamic Traction)
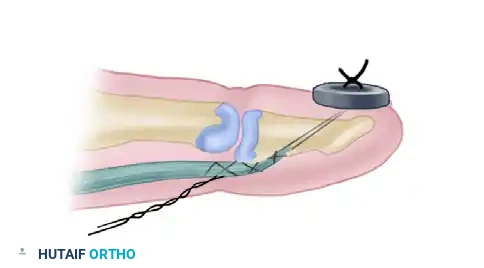
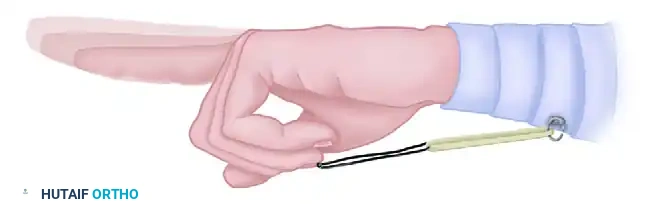
In the Kleinert protocol, active finger extension is permitted within the confines of a dorsal blocking splint, while passive flexion is achieved using a dynamic rubber band traction system attached to the fingernail and anchored at the wrist.
- Splinting: The wrist and hand are held in a posterior plaster or thermoplastic splint. The wrist is positioned in 20 to 30 degrees of flexion, and the MCP joints at 40 to 60 degrees of flexion. The interphalangeal joints are splinted in extension.
- Traction Setup: A suture is passed through the tip of the fingernail, or a garment hook is glued to the nail, allowing the attachment of an elastic band. The rubber band is passed beneath a roller or a safety pin in the palm (to alter the line of force and ensure a perpendicular pull) and secured to the distal forearm.
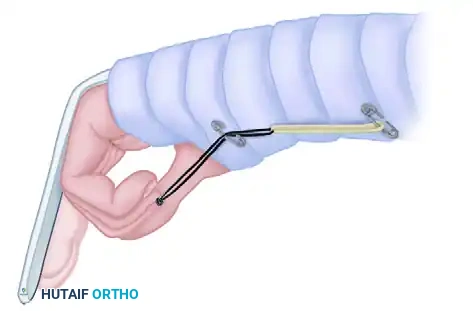
- Mechanics: The safety pin maintains the finger in flexion of 40 to 60 degrees at the proximal interphalangeal (PIP) joint with no tension on the rubber band at rest. The patient actively extends the digit against the light resistance of the rubber band. When the extensor muscles relax, the rubber band passively pulls the finger back into flexion, gliding the repaired flexor tendon without active muscle contraction.
The Modified Duran Protocol (Controlled Passive Motion)
The Duran technique involves a controlled passive motion program utilizing a dorsal blocking splint without dynamic rubber band traction.
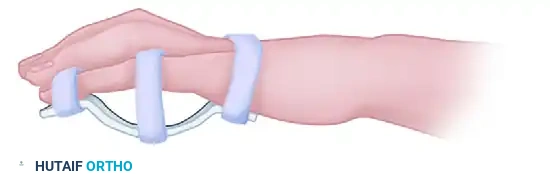
- Splinting: A nonremovable postoperative dorsal splint is applied. The wrist is positioned in 20 to 45 degrees of flexion, with the MCP joints in 50 to 70 degrees of flexion, and the IP joints left in a neutral, extended position.
- Intraoperative Excursion Check: Before closure of the wound, the surgeon determines the amount of passive movement of the fingertip required to create a 3- to 5-mm excursion of the tendon. This minimal excursion is sufficient to prevent dense adhesion formation.
- Exercise Regimen: Beginning on the first postoperative day, passive flexion and extension of the PIP and DIP joints are demonstrated. The patient is instructed to perform eight repetitions of PIP, DIP, and composite passive flexion and extension twice daily.

Early Active Motion (EAM) and Multistrand Repairs
The margin of safety with early mobilization is significantly increased if the tendon repairs have been performed using stronger multistrand techniques (four, six, or eight core strands).
- Place and Hold: If a robust multistrand repair has been achieved, a "place and hold" exercise may be added for highly compliant patients. The therapist passively flexes the digits, and the patient gently contracts their flexor muscles to "hold" the position.
- Progression: At 3 to 4 weeks, the dorsal blocking splint can be transitioned to a removable splint. By 6 to 8 weeks, dynamic extension splinting may be introduced to address any PIP joint flexion contractures. Strengthening exercises commence at 8 to 10 weeks, with a return to normal, unrestricted hand use expected by 10 to 12 weeks post-repair.

Special Splinting Considerations for Zone IV
If the transverse carpal ligament was completely released during a Zone IV repair and could not be repaired or Z-lengthened, standard splinting protocols must be altered. The wrist should be brought nearly to neutral (rather than 45 degrees of flexion), and the fingers flexed more acutely. This positioning diminishes pressure on the volar skin flaps and minimizes the risk of the repaired tendons bowstringing out of the carpal vault. If the TCL is partially intact or repaired, standard immobilization with the wrist in 45 degrees of flexion is maintained.
📚 Medical References
- Flexor tendon repair in zone 2 followed by early active mobilization, J Hand Surg 21B:624, 1996.
- Boyer MI, Strickland JW, Engles D, et al: Flexor tendon repair and rehabilitation, state of the art in 2002, Instr Course Lect 52:137, 2003.
- Browne EZ, Ribik CA: Early dynamic splinting for extensor tendon injuries, J Hand Surg 14A:72, 1989.
- Bruner S, Wittemann M, Jester A, et al: Dynamic splinting after
You Might Also Like