Patient Case: Resurfacing Primary Hip Arthroplasty for Lasting Relief

Key Takeaway
We review everything you need to understand about Patient Case: Resurfacing Primary Hip Arthroplasty for Lasting Relief. Primary hip arthroplasty, specifically hip resurfacing, addresses severe osteoarthritis causing debilitating hip pain and limited mobility, as illustrated by a 52-year-old male with chronic left groin pain. Treatment options, including total hip arthroplasty, are evaluated, with resurfacing selected for its optimal performance. This procedure aims to restore function and alleviate discomfort when conservative measures are insufficient.
A 45-year-old active male presents with chronic, refractory right hip pain. His examination shows restricted range of motion, and his radiographs are provided. What is your primary radiographic diagnosis, and what are the specific features you are looking for on this AP pelvis and Dunn lateral view?
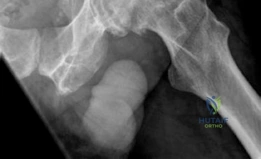
Candidate: The patient has end-stage osteoarthritis of the right hip secondary to femoroacetabular impingement (FAI). The AP pelvis shows joint space narrowing, subchondral sclerosis, and osteophyte formation. The Dunn lateral shows a cam morphology at the head-neck junction with a high alpha angle.
Candidates often provide a descriptive list of findings without synthesizing them into a structured diagnosis. Failing to quantify the alpha angle or mention the Tönnis grade demonstrates a lack of clinical precision required at this level.
Start with the diagnosis: End-stage secondary osteoarthritis due to cam-type FAI. Key features: On the AP pelvis, note the Tönnis Grade 3 changes (obliteration of joint space, sclerosis, cysts). On the Dunn lateral, identify the cam lesion at the anterolateral head-neck junction. Crucially, quantify the alpha angle (e.g., 72 degrees) and state that the lateral center-edge angle is normal, ruling out dysplasia or pincer/protrusio components.
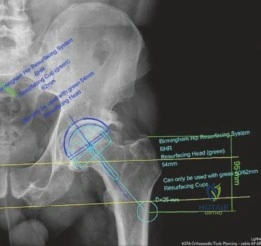
Given this patient's age and high functional demands, he is requesting a Hip Resurfacing Arthroplasty (HRA). What are the specific selection criteria, and which patient factors would make you abandon this plan in favor of a standard Total Hip Arthroplasty (THA)?
Candidate: The ideal candidate is a male under 65 with good bone stock. I would avoid HRA if there is femoral head necrosis, large cysts, or significant dysplasia. I also worry about metal ion sensitivity in women.
Providing a vague list. Failing to mention absolute clinical contraindications like impaired renal function (metal excretion) or specific radiographic contraindications like cystic lesions >1cm or poor bone mineral density.
Structure the answer into Patient and Biological Factors: Young, active male with primary OA and normal bone mineral density (Dorr A). Anatomical Factors: No significant leg length discrepancy, no severe dysplasia or protrusio, and no large femoral head cysts (>1cm). Contraindications: Documented metal allergy, renal insufficiency, and female gender (due to higher failure rates and smaller component sizing).
During the femoral preparation, you are concerned about the risk of fracture. What is the most common technical error that causes early catastrophic failure of the femoral component, and how do you mitigate this risk?

Candidate: The biggest risk is notching the superior femoral neck during reaming. This acts as a stress riser. You prevent this by using the jig correctly and ensuring you don't ream too deeply.
Failing to mention the concept of valgus positioning. Simply saying "don't notch" is insufficient; the examiner wants to hear how the alignment of the guide pin influences the stress distribution.
The primary technical error is superior femoral neck notching, which creates a critical stress riser in an area of high tensile stress. To mitigate this, place the guide pin in a relative valgus position (135–140 degrees) to convert tensile forces to compressive forces across the neck. If a notch is created, the surgeon must be prepared to abandon the HRA and proceed to a standard THA to avoid an imminent subcapital fracture.
