Mastering Hip Disarticulation: Through the Hip Joint Capsule
Key Takeaway
Looking for accurate information on Mastering Hip Disarticulation: Through the Hip Joint Capsule? Hip disarticulation is the surgical amputation of the lower extremity through the hip joint capsule. This rare procedure is performed when extensive tumors of the femur and thigh are too advanced for limb-sparing techniques. It is necessary for adequate tumor resection in cases involving proximal transosseous metastases, pathologic fractures, or large adjacent soft tissue masses, ensuring complete removal.
Introduction and Epidemiology
Hip disarticulation is a radical amputation of the lower extremity performed through the hip joint capsule. In the modern era of orthopedic oncology, the vast majority of lower extremity sarcomas and aggressive benign tumors are amenable to limb-salvage techniques. However, hip disarticulation remains an indispensable surgical intervention for massive tumors of the femur and thigh that preclude adequate oncologic resection with limb preservation. Beyond the realm of oncology, this procedure is occasionally necessitated by overwhelming trauma, unsalvageable lower extremity ischemia, or fulminant necrotizing soft tissue infections extending into the proximal thigh.
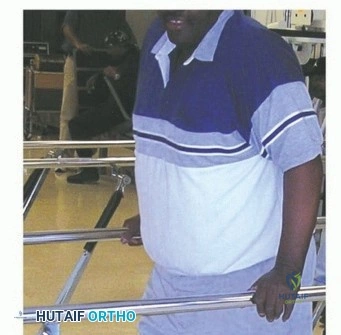
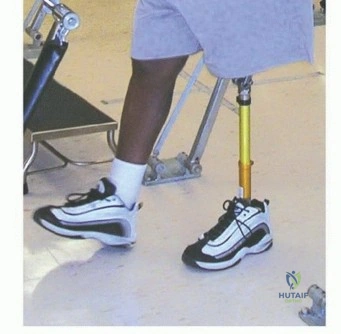
Historically, disarticulation of the hip for malignant tumors was associated with profound functional morbidity. Patients undergoing this procedure are left without a residual limb and, critically, without a fulcrum to power and control an artificial prosthesis. The biomechanical consequences are severe. The energy expenditure required for ambulation following a standard hip disarticulation is reported to be 82% to 100% greater than that of a non-amputee. In stark contrast, a long below-knee amputation increases energy expenditure by only about 10% to 20%. Consequently, when a patient with a hip disarticulation attempts prosthetic ambulation, the cardiopulmonary demands can exceed twice normal baseline requirements, often relegating patients to crutch-assisted ambulation or wheelchair dependence.

Given these formidable functional challenges, any surgical intervention that preserves a functional lever arm can dramatically reduce energy expenditure, thereby increasing the likelihood of prosthetic use and improving overall quality of life. In cases where the proximal thigh soft tissues are free from tumor invasion, reconstructing a functional proximal thigh stump utilizing a modular proximal femur prosthesis has emerged as a superior alternative to standard disarticulation. When this is not oncologically feasible, true disarticulation through the capsule must be executed with meticulous attention to flap viability and neuroma prevention.
Epidemiologically, hip disarticulation represents less than 1% of all major lower extremity amputations. The primary indication remains primary bone sarcomas (such as osteosarcoma and Ewing sarcoma) and high-grade soft tissue sarcomas of the proximal thigh with extensive neurovascular involvement. Secondary indications include massive trauma resulting in a mangled extremity with proximal vascular avulsion, and severe infections such as clostridial myonecrosis or Group A streptococcal necrotizing fasciitis that threaten the patient's life.

Surgical Anatomy and Biomechanics
A thorough mastery of the regional anatomy is critical to executing a hip disarticulation efficiently, minimizing intraoperative blood loss, and ensuring adequate soft tissue margins for oncologic clearance. The procedure requires navigation through multiple anatomical compartments, necessitating an intimate understanding of the vascular and nervous networks.
Vascular Anatomy
The hip joint and proximal thigh are supplied by a robust collateral network. The primary arterial supply includes the common femoral, superficial femoral, and profunda femoris arteries. Additional critical vessels that must be meticulously identified and ligated include the medial and lateral femoral circumflex arteries, the obturator artery, and the superior and inferior gluteal arteries.

Preoperative angiography or computed tomography (CT) angiography can be a valuable adjunct in delineating these structures, particularly the external iliac, common femoral, and profundus arteries, in the setting of large, distorting tumor masses. The posterior myocutaneous flap, which is the workhorse for soft tissue coverage in a standard hip disarticulation, relies heavily on the inferior gluteal artery. Compromise of this vessel during the posterior dissection will result in catastrophic flap necrosis.
Key Anatomical Landmarks and Compartments
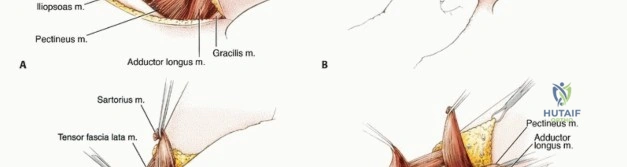
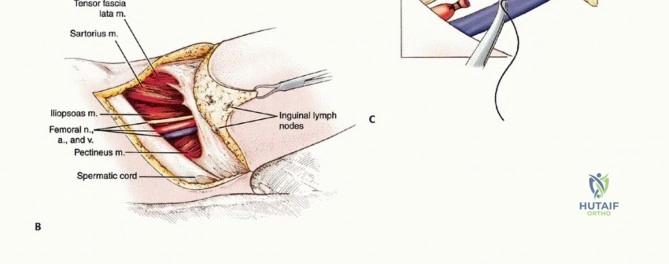
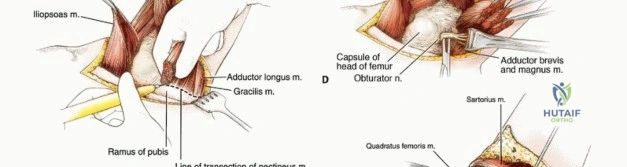
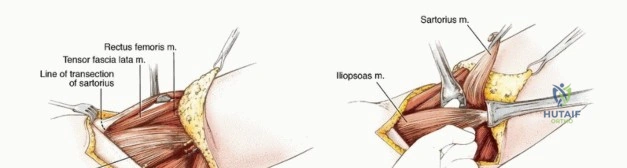
The femoral triangle is the gateway to the anterior neurovascular bundle. It is bordered superiorly by the inguinal ligament, laterally by the sartorius muscle, and medially by the adductor longus muscle. Accessing this triangle allows for early and definitive control of the femoral artery and vein, as well as the femoral nerve. Early ligation of the vein is critical in oncologic cases to prevent tumor embolization during subsequent limb manipulation.

The hip joint capsule itself is a dense, fibrous envelope that covers the anterior hip down to the intertrochanteric line but leaves a significant portion of the posterior femoral neck extracapsular. The capsule is reinforced anteriorly by the robust iliofemoral ligament (Y ligament of Bigelow), inferiorly by the pubofemoral ligament, and posteriorly by the ischiofemoral ligament.
Posteriorly, the ischiorectal fossa must be carefully evaluated preoperatively via magnetic resonance imaging (MRI) and CT. This space is bounded medially by the sphincter ani externus and anal fascia, laterally by the ischial tuberosity and obturator fascia, anteriorly by the transversus perinei superficialis fascia, and posteriorly by the gluteus maximus and sacrotuberous ligament. Tumor extension into this fossa dictates flap design and may alter the feasibility of a standard posterior flap, occasionally necessitating an anterior thigh flap or a modified hemipelvectomy.

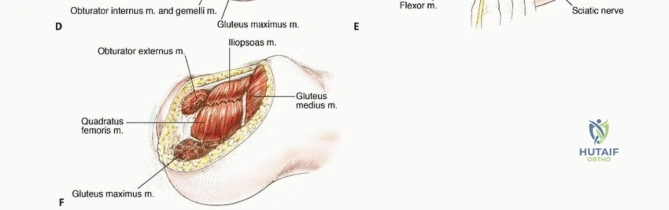
The muscular envelope of the hip comprises the tensor fascia lata (TFL), gluteus maximus, and the iliotibial band. At least one of these structures typically requires longitudinal splitting to gain adequate surgical access to the joint capsule. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris) must be systematically divided at their femoral insertions to access the posterior capsule and protect the underlying sciatic nerve.
Biomechanical Considerations
From a biomechanical standpoint, the absence of a femoral lever arm fundamentally alters the mechanics of ambulation. In a healthy individual, the hip abductors (gluteus medius and minimus) stabilize the pelvis during the single-leg stance phase of gait. Following hip disarticulation, pelvic stability must be achieved entirely through the prosthetic socket interface.

The traditional Canadian hip disarticulation prosthesis relies on a pelvic basket that captures the iliac crests to suspend the prosthesis and transmit weight-bearing forces through the ischial tuberosity. Forward progression of the prosthetic limb is achieved not through hip flexion, but through a combination of pelvic tilt and truncal momentum. This non-physiologic gait pattern explains the profound metabolic cost associated with prosthetic ambulation in this patient population.
Indications and Contraindications
The decision to proceed with a hip disarticulation requires a rigorous multidisciplinary approach, weighing the necessity of life preservation against the inevitable functional deficits.

Indications Summary Table
| Clinical Category | Operative Indications for Hip Disarticulation | Non-Operative / Alternative Management |
|---|---|---|
| Oncologic | High-grade sarcoma of proximal thigh with neurovascular encasement; massive fungating tumors; failure of limb-salvage with local recurrence; palliative resection for intractable pain/bleeding. | Limb-salvage with endoprosthesis (if neurovascular bundle and adequate margins can be preserved); modified hemipelvectomy (if tumor extends into pelvis/acetabulum). |
| Traumatic | Mangled extremity with proximal avulsion of femoral vessels and sciatic nerve disruption; unsalvageable crush injury with profound myonecrosis. | Revascularization and complex soft tissue reconstruction (if nerve continuity is present and warm ischemia time is minimized). |
| Infectious | Fulminant necrotizing fasciitis or gas gangrene extending to the proximal thigh/groin; intractable chronic osteomyelitis of the proximal femur with systemic sepsis. | Aggressive serial debridement and targeted antibiotic therapy (if infection is localized distal to the proximal third of the thigh). |
| Vascular | End-stage peripheral arterial disease with unsalvageable proximal ischemia and ascending wet gangrene. | Endovascular or open bypass procedures (if distal runoff and viable tissue remain). |
Strict Contraindications
Absolute contraindications to standard hip disarticulation include tumor extension into the hip joint, acetabulum, or pelvic ring, which mandates a hemipelvectomy (hindquarter amputation) to achieve negative oncologic margins. Similarly, involvement of the common iliac vessels proximal to the inguinal ligament requires a more proximal vascular control strategy and often a transpelvic approach.

Relative contraindications include severe cardiopulmonary instability precluding major surgery, though in cases of ascending sepsis or hemorrhage, the procedure may be a lifesaving necessity.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount. In oncologic cases, recent staging studies (chest CT, whole-body bone scan, or PET-CT) are mandatory. Local imaging must include a high-resolution MRI of the entire femur and pelvis to precisely delineate the proximal extent of the tumor, the relationship to the neurovascular bundle, and the presence of any skip lesions.

Multidisciplinary Tumor Board Review
All oncologic cases must be discussed in a multidisciplinary sarcoma tumor board. The surgical margins are mapped out based on the MRI. If the tumor closely approaches the anterior compartment, the standard posterior flap may need to be lengthened. Conversely, if the posterior compartment is involved, an atypical anterior or medial flap must be designed.
Blood Management and Anesthesia
Hip disarticulation is associated with significant blood loss, primarily from the extensive muscular transections and large venous collaterals. Preoperative type and crossmatch for a minimum of 4 units of packed red blood cells is standard. Cell salvage systems (e.g., Cell Saver) are contraindicated in oncologic and infectious cases due to the risk of systemic dissemination.
Anesthetic management typically involves general endotracheal anesthesia combined with regional techniques (such as an epidural or lumbar plexus block) to manage the profound postoperative pain and reduce phantom limb phenomena.
Patient Positioning and Draping
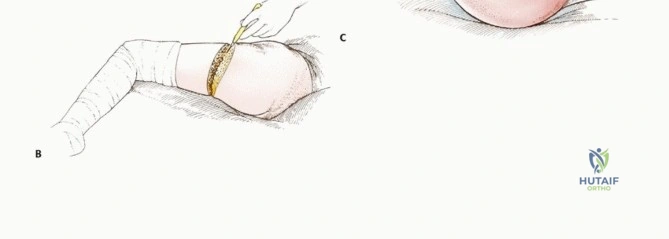
The patient is typically positioned in the lateral decubitus position, resting on the unaffected side, using a beanbag or pegboard for rigid stabilization. This "floppy lateral" position allows the surgeon to easily rotate the patient anteriorly to access the groin and posteriorly to elevate the gluteal flap.

The entire hemipelvis, lower abdomen, flank, and the entire operative extremity are prepped and draped free. The foot and lower leg are wrapped in an impervious stockinette to allow the limb to be manipulated as a lever during the disarticulation. A sterile tourniquet is generally not applicable for a true hip disarticulation, though in cases of massive trauma, temporary proximal aortic control via a REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) or open retroperitoneal iliac clamping may be utilized.

Detailed Surgical Approach and Technique
The classical approach to hip disarticulation utilizes a racquet-shaped incision with a large posterior gluteal myocutaneous flap. The operation proceeds systematically through distinct anatomical phases to ensure vascular control, oncologic clearance, and minimal blood loss.

Phase One Incision and Anterior Dissection
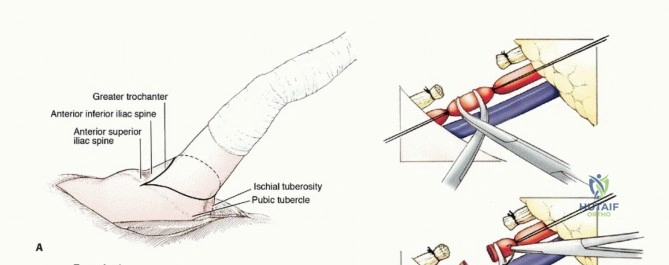
The incision begins anteriorly at the level of the anterior superior iliac spine (ASIS), sweeping medially and distally parallel to the inguinal ligament toward the pubic tubercle. It then drops distally along the medial thigh, crosses the posterior thigh distal to the gluteal fold, and ascends laterally over the greater trochanter to meet the starting point at the ASIS.
The anterior incision is deepened through the subcutaneous tissue to the deep fascia. The femoral triangle is immediately accessed. The femoral sheath is opened, and the femoral artery and vein are isolated.
The femoral artery is doubly ligated with heavy non-absorbable suture and transfixed. The femoral vein is similarly ligated and divided. It is critical to dissect high enough to ligate the vessels proximal to the origin of the profunda femoris to avoid troublesome bleeding later in the case.

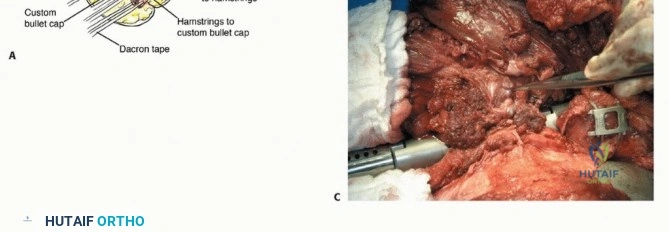
The femoral nerve is identified lateral to the artery, drawn distally, sharply transected, and allowed to retract deep into the psoas muscle bed to prevent symptomatic neuroma formation in the groin. At this stage, targeted muscle reinnervation (TMR) can be performed by coapting the proximal stump of the femoral nerve to a nearby expendable motor branch, significantly reducing the incidence of phantom limb pain.
Phase Two Medial Compartment Release
With the anterior neurovascular bundle controlled, the limb is abducted and externally rotated. The dissection proceeds medially. The adductor muscle group (adductor longus, brevis, and magnus) and the pectineus are identified and transected near their pubic and ischial origins.
During this medial dissection, the obturator nerve and obturator vessels are encountered as they exit the obturator foramen. These vessels must be meticulously isolated, ligated, and divided. The obturator nerve is placed under tension, transected sharply, and allowed to retract into the pelvis.

Phase Three Lateral and Posterior Dissection
The limb is then adducted and internally rotated. The lateral limb of the incision is deepened through the tensor fascia lata and the iliotibial band. The gluteus maximus is identified. Depending on the oncologic margins required, the gluteus maximus is either elevated as part of the posterior flap or transected at its insertion on the gluteal tuberosity of the femur.
To preserve the vascularity of the posterior flap, the inferior gluteal artery must be protected as it exits the greater sciatic foramen inferior to the piriformis muscle.

The short external rotators (piriformis, gemelli, obturator internus, and quadratus femoris) are sharply detached from their insertions on the greater trochanter and posterior femur. This exposes the sciatic nerve.
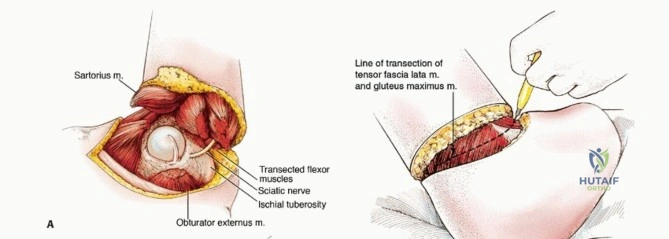
The sciatic nerve is a massive structure that contains a significant intrinsic blood supply (the arteria comitans nervi ischiadici). It must be securely ligated prior to transection to prevent profound hemorrhage from the vasa nervorum. The nerve is drawn distally, ligated, transected sharply, and allowed to retract deep to the piriformis. Again, TMR is highly recommended here, coapting the sciatic nerve fascicles to motor branches of the gluteus maximus or surrounding musculature.
Phase Four Capsulotomy and Disarticulation
With all muscular and neurovascular connections severed, the hip joint capsule is exposed circumferentially. The capsule is incised anteriorly, superiorly, and posteriorly.

The limb is forcefully externally rotated and extended to dislocate the femoral head anteriorly from the acetabulum. The ligamentum teres (ligament of the head of the femur) is visualized and transected with heavy curved Mayo scissors or a scalpel.
Any remaining inferior capsular attachments or muscular fibers are divided, and the limb is delivered from the operative field.

Phase Five Hemostasis and Closure
The empty acetabulum and surrounding soft tissues are rigorously inspected for hemostasis. The acetabular cartilage is typically left intact unless involved by disease, as denuding the cartilage increases bleeding and offers no functional benefit.
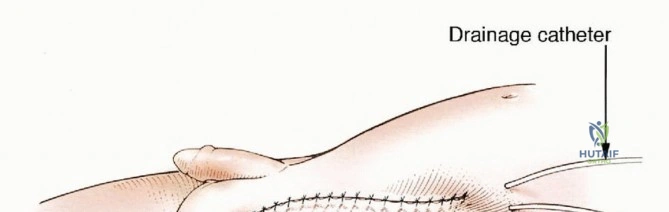
A large bore closed-suction drain is placed deep in the acetabular void and brought out through a separate stab incision laterally. A second drain is placed in the subfascial layer.

The posterior gluteal flap is swung anteriorly to cover the defect. Myodesis is performed by suturing the deep fascia of the gluteus maximus to the origin of the pectineus and the inguinal ligament anteriorly. This creates a robust, muscular pad over the pelvis.
The subcutaneous tissues are closed in multiple layers with absorbable suture, and the skin is reapproximated with non-absorbable sutures or surgical staples. The final suture line should lie anteriorly and superiorly, away from the perineum and the dependent ischial weight-bearing area, to minimize the risk of contamination and pressure necrosis.
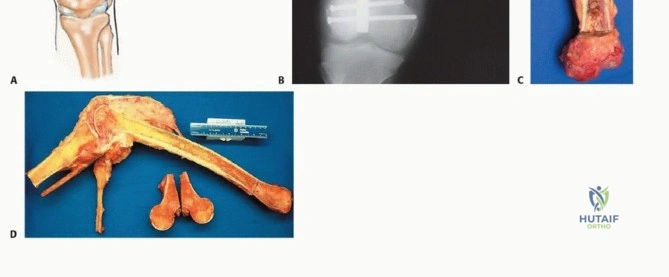
Clinical & Radiographic Imaging