

Comprehensive Introduction and Patho-Epidemiology
Alright team, let us gather around. Today, we are tackling a hip resurfacing arthroplasty, a procedure that has truly evolved the landscape of hip reconstruction, particularly for our younger, more active patients. This is not merely about replacing a degenerative joint; it is fundamentally about preserving precious femoral bone stock, optimizing biomechanical loading, and restoring high-level, impact-tolerant function. Hip resurfacing represents a significant paradigm shift, offering a mathematically and biologically sound alternative to traditional total hip arthroplasty (THA) by preserving the native femoral head and neck. It is an exquisitely technically demanding procedure, requiring unparalleled intraoperative precision, three-dimensional spatial awareness, and a profound understanding of hip biomechanics and proximal femoral vascularity.
The patho-epidemiology of patients indicated for this procedure typically involves early-onset coxarthrosis in a high-demand demographic. These are frequently males under the age of 60 who present with primary osteoarthritis, post-traumatic arthritis, or secondary degenerative changes stemming from mild childhood dysplasias or slipped capital femoral epiphysis (SCFE). Unlike the traditional THA population, these patients possess robust bone quality and harbor expectations of returning to heavy manual labor or high-impact athletics. The physiological demand placed on the hip joint in this cohort necessitates a bearing surface and fixation method capable of withstanding extreme cyclical loading without catastrophic failure or accelerated wear.


While hip resurfacing is optimally indicated for conditions like primary osteoarthritis, we invariably encounter cases of osteonecrosis of the femoral head. This presents a unique and formidable challenge, as the presence of a necrotic lesion critically compromises the fixation of the femoral component. We know from exhaustive registry data and peer-reviewed literature that survival rates for hip resurfacing in avascular necrosis (AVN) are generally lower than for osteoarthritis. The femoral head is "resurfaced" by inserting a cemented femoral component over a meticulously sculpted bony peg, while the acetabular cup is typically press-fit. If the cement mantle interfaces with necrotic, non-viable bone, the risk of early aseptic loosening or catastrophic femoral neck fracture increases exponentially.
When evaluating the various hip resurfacing systems available on the market, the surgeon must appreciate the nuanced engineering behind each implant. Systems differ vastly in material composition (predominantly high-carbon, as-cast, or forged cobalt-chromium), surface treatments (Vacuum Plasma Sprayed Titanium or sintered CoCr beads with Hydroxyapatite), and cup design geometry (full hemisphere versus truncated 165- or 170-degree designs). Furthermore, variations in manufacturing processes, carbide content, component thickness, and diametrical clearance dictate the tribological behavior and fluid-film lubrication of the metal-on-metal bearing. Familiarity with your chosen system's specific instrumentation and tolerances is paramount to achieving reproducible success.
| Resurfacing System | Material | Fixation (Femoral) | Fixation (Acetabular) | Femoral Size (mm) | Acetabular Size (mm) | Dysplastic Cups | Surface Clearance (nm) | Hip Design | Thickness (mm) |
|---|---|---|---|---|---|---|---|---|---|
| Cormet (Corin) | Cast & Heat-treated high-carbon CoCr | Cemented | Uncemented TiVPS with HA press-fit | 40 to 56 in 4-mm increments | 46 to 62 in 2-mm increments | Available | 10 | Full hemisphere | 3–4 |
| Birmingham Hip Resurfacing (BHR; Smith & Nephew) | As cast high-carbon CoCR | Cemented | Sintered CoCr beads with HA press-fit | 38 to 58 in 4-mm increments | 44 to 66 in 2-mm increments | Available | 20 | Full hemisphere | 3–4 |
| Conserve Plus (Wright Medical) | Cast & Heat-treated high-carbon CoCr | Cemented | Sintered CoCr beads with HA full mantle | 36 mm to 56 mm in 2-mm increments | 42 mm to 64 mm in 2-mm increments | Does not offer | 10 | 170-degree truncated hemisphere | 3 or 3.5 |
| Articular Surface Replacement (ASR; Depuy) | Cast & Heat-treated high-carbon CoCr | Cemented | Sintered CoCr beads with HA thin mantle | 39 to 63 in 2-mm increments | 44 to 70 in 2-mm increments | Does not offer | 10 | 170-degree truncated hemisphere | 2.5–3.5 |
| Durom (Zimmer/Centerpulse) | Forged high-carbon CoCr | Cemented | Uncemented Ti VPS full mantle | 38 to 60 in 2-mm increments | 44 to 66 in 2-mm increments | Does not offer | 5 | 165-degree truncated hemisphere | 4 |


Detailed Surgical Anatomy and Biomechanics
A masterful hip resurfacing demands an intimate, almost instinctual understanding of the proximal femoral vascularity. The primary blood supply to the adult femoral head is derived from the deep branch of the medial femoral circumflex artery (MFCA). This vessel traverses posterior to the obturator externus and anterior to the superior gemellus, giving rise to the critical posterosuperior and posteroinferior retinacular vessels. During a posterior approach, meticulous preservation of the obturator externus tendon and careful execution of the capsulotomy are mandatory to avoid devascularizing the remaining femoral head and neck. Iatrogenic disruption of this vascular network is a primary catalyst for postoperative osteonecrosis and subsequent structural failure of the resurfaced construct.
Biomechanically, hip resurfacing offers distinct advantages over standard stemmed THA by preserving the native femoral offset, functional leg length, and normal proximal femoral strain distribution. By retaining the femoral head and neck, the implant facilitates physiological stress transfer directly into the proximal metaphysis, adhering to Wolff's Law and actively preventing the proximal stress shielding and diaphyseal hypertrophy frequently observed with rigid intramedullary stems. This physiological loading is critical for maintaining the dense trabecular bone required to support the cemented femoral component over the patient's lifetime.



The tribology of the large-diameter metal-on-metal articulation is another biomechanical cornerstone of this procedure. The large femoral head closely mimics native anatomy, thereby maximizing the "jump distance"—the vertical distance the head must travel to dislocate from the acetabulum. This inherent geometric stability allows patients to achieve a massive, unconstrained range of motion, essential for deep flexion activities and athletic pursuits. Furthermore, the large bearing surface promotes fluid-film lubrication during active movement, where a microscopic layer of synovial fluid separates the cobalt-chromium surfaces, theoretically reducing volumetric wear to near zero under optimal, well-positioned conditions.
However, the acetabular anatomy presents its own unique challenges when accommodating these large-diameter components. The surgeon must navigate the spatial constraints of the anterior and posterior columns to ensure adequate bony coverage for the press-fit cup without inducing psoas impingement anteriorly. Proper identification and management of the transverse acetabular ligament are essential for establishing the true floor of the acetabulum, ensuring the cup is seated at the correct depth and inclination. Failure to recognize subtle dysplastic changes or over-reaming the subchondral bone can lead to catastrophic loss of press-fit stability, necessitating intraoperative conversion to a standard THA.



Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of long-term success in hip resurfacing arthroplasty. The ideal candidate is a younger, highly active male (typically under 60-65 years of age) presenting with severe primary osteoarthritis, excellent bone stock, and a strong desire to return to high-impact activities. Gender plays a highly significant role in survivorship data; males generally require larger component sizes (typically >50mm), which are biomechanically more forgiving and generate lower rates of edge-loading and subsequent metal ion dissemination. The presence of a degenerative hip joint characterized by debilitating pain and decreased range of motion, particularly when joint-preserving procedures (like osteotomies or arthroscopy) have failed or are not indicated, solidifies the decision to proceed with resurfacing.
Conversely, the indications for female patients and those with secondary osteoarthritis require a highly nuanced, cautious approach. Women generally possess smaller femoral neck diameters, necessitating smaller implant sizes (<48mm). Smaller bearings have a reduced clearance arc and are highly susceptible to edge-loading if the acetabular component is placed in even slight excessive inclination or anteversion. This edge-loading rapidly breaks down the fluid-film lubrication, leading to accelerated wear, elevated cobalt and chromium ion levels, and the devastating complication of Adverse Local Tissue Reaction (ALTR) or pseudotumor formation. Therefore, small-stature females are often better served by a modern ceramic-on-ceramic total hip arthroplasty.



Absolute contraindications must be strictly respected to avoid early, catastrophic failures. Abnormal anatomy of the femoral head or neck, such as severe varus deformity or massive cystic degeneration, precludes proper component seating and drastically increases the risk of postoperative fracture. Severe bone deficiency, whether from advanced osteoporosis or metabolic bone disease, compromises both the cemented femoral fixation and the uncemented acetabular press-fit. Large necrotic lesions (greater than 1/3 of the femoral head) or cysts larger than 1 centimeter in the weight-bearing zone significantly weaken the underlying structural support, making resurfacing an inappropriate choice. Furthermore, known metal hypersensitivity and severe renal impairment are absolute contraindications due to the systemic dissemination and renal clearance of metal ions.
| Parameter | Favorable Indications for Resurfacing | Absolute Contraindications for Resurfacing |
|---|---|---|
| Patient Demographics | Male, Age < 65 years, High activity level | Female of childbearing age, Age > 65 with poor bone stock |
| Primary Diagnosis | Primary Osteoarthritis, Post-traumatic OA | Inflammatory arthropathy (e.g., severe RA), Active infection |
| Bone Quality / Anatomy | Robust trabecular bone, Normal neck-shaft angle | Osteoporosis, Severe dysplasia, Severe varus deformity |
| Femoral Head Pathology | Minimal cystic changes, Intact structural integrity | Large cysts (>1cm), Extensive AVN (>30% of head involvement) |
| Systemic Factors | Normal renal function, No metal allergies | Renal insufficiency, Documented severe metal hypersensitivity |
| Limb Length | Minimal to no leg length discrepancy | Severe leg length discrepancy requiring structural correction |



Pre-Operative Planning, Templating, and Patient Positioning
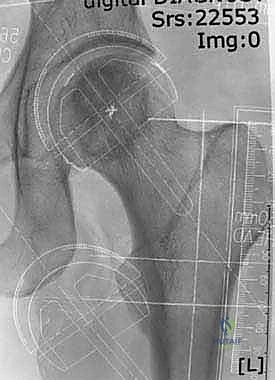
Before a scalpel ever touches the skin, meticulous and exhaustive preoperative planning is mandatory. This procedure demands mathematical precision in component sizing and alignment; there is zero margin for error. Radiographic evaluation begins with high-quality, standardized conventional radiographs—specifically, an AP pelvis, a cross-table lateral, and a false profile view. We explicitly utilize standard-sized films with a known magnification marker (typically a 20% coin or sphere) rather than relying solely on uncalibrated digital interfaces. The primary objective of templating is to select a femoral component size that completely covers the prepared femoral head without over-reaming the peripheral bone or, disastrously, notching the superior femoral neck.
Femoral component alignment is the crux of the preoperative plan. The surgeon must aim for a neutral or slight valgus alignment (typically 5 to 10 degrees in the coronal plane) relative to the native femoral neck axis. The target is to establish a 135- to 140-degree angle with the long axis of the femoral shaft. This specific orientation converts deleterious shear stresses into compressive forces across the head-neck junction, drastically minimizing the risk of postoperative femoral neck fracture. Varus positioning is an unforgivable technical error in resurfacing. Using the ruler printed on the template, we measure the precise distance from the tip of the greater trochanter to the anticipated guide pin insertion point on the lateral femoral cortex, allowing us to reproduce this exact entry point intraoperatively.



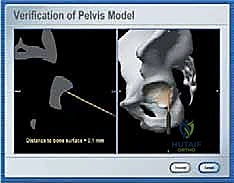
Patient positioning and the integration of intraoperative technology play a pivotal role in executing the preoperative plan. The patient is placed in the lateral decubitus position on a specialized, rigid orthopedic table. Impeccable padding of all pressure points is verified, and the pelvis is locked securely using anterior and posterior supports to prevent any spatial shifting during heavy reaming. While hip resurfacing has been historically performed using manual jigs, the integration of Computer-Assisted Navigation (CAN) systems has revolutionized the accuracy of this procedure. Image-free CAN systems provide real-time, three-dimensional localization, enabling flawless bone cuts and exact implant positioning, thereby virtually eliminating the risk of undetected varus malposition or neck notching.
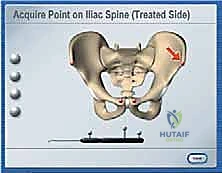
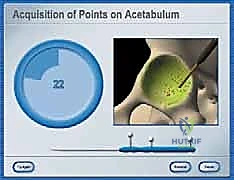
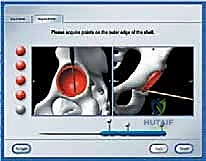
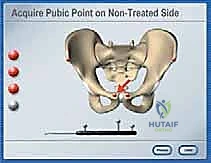
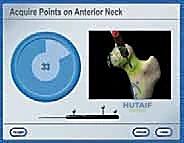
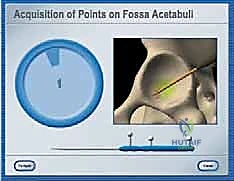
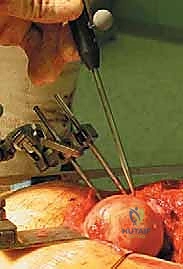
When deploying an image-free navigation system, the initial and most critical step is the accurate digitization of the patient's pelvic and femoral anatomical landmarks. The surgeon uses a tracked probe to register the anterior superior iliac spines (ASIS), the pubic symphysis, and the epicondylar axis of the distal femur. This establishes the individual, patient-specific coordinate systems essential for precise prosthesis positioning. While navigation offers tremendous benefits in mitigating human error, surgeons must remember that registration procedures require meticulous attention to detail; irregular soft tissue distribution or osteophytic overgrowth around the femoral neck can introduce registration errors, compromising the entire navigational matrix.


Step-by-Step Surgical Approach and Fixation Technique
For total hip resurfacing, the posterolateral approach remains our absolute standard and the most globally utilized technique. It provides unparalleled, extensile exposure of both the acetabulum and the proximal femur without unduly compromising postoperative abductor muscle function, which is critical for high-level athletic recovery. Following a straight incision centered over the posterior edge of the greater trochanter, the fascia lata is split, and the gluteus maximus is bluntly split in line with its fibers. The sciatic nerve is carefully identified and protected. The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) are tagged and sharply detached close to their femoral insertion. A precise, T-shaped capsulotomy is performed, ensuring the preservation of the critical retinacular vessels running along the posterosuperior neck.
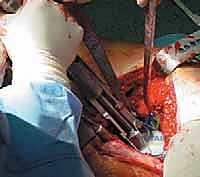
Once the hip is dislocated, acetabular preparation commences. This step is conceptually similar to traditional THA but requires heightened vigilance to preserve subchondral bone. The acetabulum is sequentially reamed to a perfect hemisphere. Because resurfacing cups do not typically utilize supplemental screw fixation, achieving an absolute, rigid press-fit is mandatory. The subchondral plate must be preserved to provide structural support for the implant. The acetabular component is then impacted into place, targeting an abduction angle of 40 to 45 degrees and an anteversion of 15 to 20 degrees. Any deviation into excessive inclination or anteversion will precipitate edge-loading of the metal-on-metal bearing, leading to catastrophic metallosis.



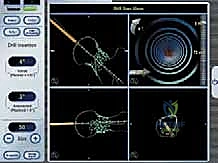
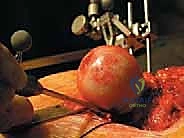
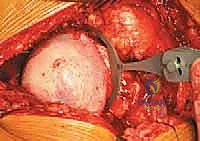
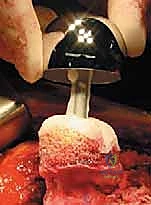
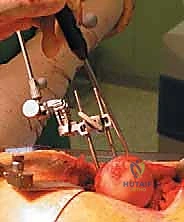
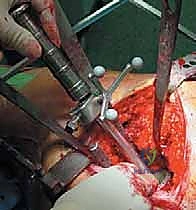
Femoral preparation is the true masterclass element of this operation. Using either navigation or precise mechanical jigs, a central guide pin is passed from the lateral femoral cortex, through the center of the femoral neck, and out the center of the femoral head. This pin dictates the entire trajectory of the femoral preparation. A cylindrical reamer is passed over the pin to machine the peripheral equator of the femoral head, strictly avoiding any notching of the superior neck cortex. Subsequently, a chamfer reamer is utilized to sculpt the dome of the head into a precise geometric peg that perfectly matches the internal contours of the chosen femoral implant. In cases of mild AVN, all necrotic bone must be meticulously curetted out and grafted, or the cement mantle must be carefully managed to bridge the defect without causing thermal necrosis to the remaining viable bone.

Component implantation requires a highly choreographed sequence. The femoral head is thoroughly lavaged with pulsatile lavage and dried completely to ensure optimal micro-interlock of the cement. Low-viscosity polymethylmethacrylate (PMMA) bone cement is introduced into the femoral component—not directly onto the bone—to prevent excessive cement penetration into the cancellous bed, which could cause thermal necrosis or elevate intraosseous pressure. The component is then firmly impacted onto the prepared femoral peg. The surgeon must meticulously clear any extruded cement from the head-neck junction to prevent third-body wear or impingement. The hip is then reduced, and a rigorous assessment of stability, impingement, and leg length is performed before meticulous, layered closure of the capsule and external rotators.




Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, hip resurfacing carries a distinct profile of complications that the operating surgeon must be fully prepared to manage. The most dreaded early complication is a femoral neck fracture, which typically occurs within the first 3 to 6 months postoperatively. The etiology is almost universally mechanical: varus malposition of the femoral component, unrecognized intraoperative notching of the superior femoral neck cortex, or failure to respect the presence of extensive osteonecrosis. When a neck fracture occurs, the structural integrity of the construct is lost, and the patient presents with acute, severe groin pain and an inability to bear weight.
Adverse Local Tissue Reaction (ALTR), Aseptic Lymphocyte-Dominated Vasculitis-Associated Lesion (ALVAL), and pseudotumor formation represent the most significant mid-to-late complications specific to metal-on-metal bearings. These pathologies are driven by the release of nano-particulate cobalt and chromium debris, usually secondary to edge-loading from a malpositioned acetabular cup or a component size mismatch. Patients may present with subtle groin pain, a palpable mass, or unexplained mechanical symptoms. Diagnosis relies on heavily T1-weighted Metal Artifact Reduction Sequence (MARS) MRI to identify cystic or solid soft-tissue masses, combined with serial monitoring of whole-blood cobalt and chromium ion levels.













































Detailed Chapters & Topics
Dive deeper into specialized chapters regarding hip-resurfacing