Hemiresurfacing Case Title: Active Young Patient Beats Osteonecrosis
Key Takeaway
This topic focuses on Hemiresurfacing Case Title: Active Young Patient Beats Osteonecrosis, Case title hemiresurfacing is a surgical treatment for hip osteonecrosis in active young patients with preserved acetabular cartilage and an intact labrum. This procedure resurfaces only the femoral head, offering a less invasive alternative to total hip arthroplasty. It promotes rapid recovery and allows suitable candidates to resume demanding physical activities with positive outcomes.
A 32-year-old active-duty soldier presents with 8 months of worsening groin pain, nocturnal symptoms, and a history of high-dose steroid use. Physical examination reveals an antalgic gait, positive FADIR/FABER tests, and restricted internal rotation. Given the history, what is your initial differential, how do you investigate, and what are the pathognomonic findings you expect to see?

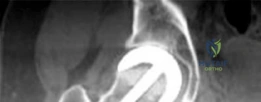
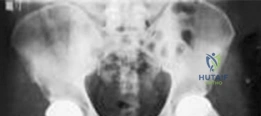
Candidate: I suspect osteonecrosis of the femoral head (ONFH) given the steroid history. I would order AP pelvis and lateral hip radiographs. If negative but symptoms persist, I would order an MRI. I expect to see the crescent sign on X-ray and the double-line sign on MRI.
Failing to mention the staging system (Ficat/Steinberg) or neglecting to include critical differential diagnoses like FAI or Transient Osteoporosis. Candidates often fail to describe the specific MRI sequences (T1 vs T2) that demonstrate the double-line sign.
A structured approach: "I would include ONFH, FAI, and Transient Osteoporosis in my differential. Investigations include AP/Lateral radiographs and non-contrast MRI (the gold standard). On MRI, the 'double-line sign' is pathognomonic: an inner high-signal line (hypervascular granulation tissue) and an outer low-signal line (sclerotic reactive bone) on T2 sequences. I would classify the disease using the Ficat/Arlet or Steinberg systems to guide management."
The patient is diagnosed with Ficat Stage III osteonecrosis with a Kerboul angle > 200 degrees. Discuss the rationale for proceeding with a femoral hemiresurfacing arthroplasty versus a total hip arthroplasty (THA) in this young, active patient.
Candidate: In a 32-year-old, we want to save bone. Hemiresurfacing preserves the femoral neck and acetabulum, making future conversion to a primary THA much simpler. It also allows for higher activity levels and better stability due to the large head size.
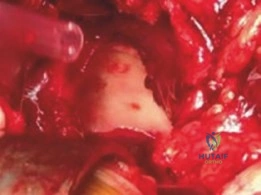
Missing the absolute necessity of an intact acetabulum. Candidates often forget to mention that intraoperative confirmation of acetabular cartilage health is the mandatory "gatekeeper" step for this procedure.
Frame the answer via "Biomechanical, Physiological, and Future-Proofing" arguments: 1. Bone preservation (retaining the neck for easier primary-style revision). 2. Acetabular sparing (avoiding polyethylene wear/osteolysis). 3. Improved biomechanics (large femoral head diameter reduces dislocation risk). 4. Activity requirements (active-duty status). Caution: "The procedure is contingent on pristine intraoperative acetabular cartilage quality; if cartilage is damaged, I must convert to THA."
You are now in theatre. Describe the critical technical step during femoral head preparation to prevent the most common catastrophic failure of a hemiresurfacing implant.
Candidate: You must avoid notching the femoral neck during reaming. If you notch the neck, it creates a stress riser that leads to a femoral neck fracture postoperatively.
Forgetting to mention the importance of guide pin alignment (valgus positioning). Notching is the result, but "inappropriate guide pin placement" is the root cause that needs to be addressed.
Identify the failure mode (femoral neck fracture) and the prevention strategy: 1. Careful guide pin placement (neutral version, slight valgus orientation). 2. Avoiding superior neck notching during cylindrical reaming. 3. Careful handling of cement to avoid thermal necrosis, which can also contribute to neck weakening. A stress-riser on the superior neck is almost always fatal to the construct.
