Mastering Upper Extremity Preparation, Draping, and Tourniquet Management

Key Takeaway
A bloodless surgical field is paramount in upper extremity and hand surgery to ensure precise dissection and protect vital neurovascular structures. This comprehensive guide details the standardized protocols for patient preparation, sterile draping, and evidence-based tourniquet management. By adhering to strict pneumatic pressure guidelines and exsanguination techniques, orthopedic surgeons can minimize ischemic complications and optimize operative outcomes.
PREPARATION AND DRAPING FOR ELECTIVE SURGERY
Irrespective of the specific operative intervention to be performed, the methodology for preparing and draping the upper extremity and hand must remain rigidly standardized. Standardization of the preoperative routine is a hallmark of high-level orthopedic practice; it reduces cognitive load, streamlines operating room efficiency, and allows the surgical team unimpeded movement about the operative field while strictly minimizing the risk of bacterial contamination.
The preparation of secondary anatomical areas for graft donor sites (e.g., iliac crest for cancellous bone, lower extremity for sural nerve or split-thickness skin grafts) will vary depending on the precise reconstructive requirements of the procedure. If skin, tendon, bone, nerve, or composite grafts are anticipated, the patient must be positioned on the operating table to allow simultaneous, unhindered access to these specific donor areas without compromising the primary sterile field.
Meticulous care must be taken during positioning to pad and protect all peripheral neurovascular structures. The ulnar nerve at the cubital tunnel and the common peroneal nerve at the fibular neck are particularly vulnerable to compression neuropraxia during prolonged procedures. Furthermore, electrocautery grounding pads must be attached to a well-vascularized muscular bed in a safe, secure manner, avoiding bony prominences to prevent thermal injury.
Hair Removal and Skin Antisepsis
Usually, the patient's hand and forearm are subjected to a preliminary surgical scrub prior to entering the operating theater. Once the patient arrives in the operating room and is transferred to the surgical table, hair removal is performed.
Surgical Warning: Hair removal must strictly be performed using electric clippers rather than razors. Micro-abrasions caused by razors significantly increase the risk of surgical site infections (SSIs) by providing a nidus for bacterial colonization. Hair should only be removed from the immediate areas where skin incisions will be made on the hand, forearm, and any secondary donor sites.
Following the induction of satisfactory anesthesia, the hand and forearm are scrubbed by a surgical assistant while the primary surgeon performs their own surgical hand antisepsis. The surgeon then dons sterile gloves to prepare the patient's skin with an evidence-based antiseptic solution.
Current literature strongly supports the use of combinations of chlorhexidine gluconate (CHG) and isopropyl alcohol, or iodophor-based soaps and paints. CHG-alcohol combinations are highly effective due to their rapid onset and sustained residual bactericidal activity.
Clinical Pearl: It is imperative to avoid wetting the cotton padding beneath the uninflated tourniquet with antiseptic solutions. Pooling of alcohol-based or iodophor solutions beneath the tourniquet cuff can lead to severe chemical burns, blistering, and subsequent skin necrosis under the pressure of the inflated cuff.
Draping Protocols and Ergonomics
Following skin antisepsis, a waterproof sheet is placed over the well-padded hand surgery table (arm board), followed by a sterile drape-sheet. A standardized combination of sterile towels and extremity drapes is applied. The draping must isolate the sterile field while leaving the upper extremity, hand, and any necessary secondary access sites fully exposed and freely mobile.
Once the field is established, the gloves used during the skin preparation are discarded. The surgeon dons a sterile surgical gown and a fresh pair of gloves. Ergonomics play a critical role in microsurgery and hand surgery; the surgeon typically sits on the axillary side of the patient's forearm, allowing optimal visualization and stabilization of the operative hand. The operating room lights are adjusted to eliminate shadows, and the planned skin incisions are carefully outlined using a sterile skin marking pencil or methylene blue applied with wooden applicator sticks.
PRINCIPLES OF TOURNIQUET APPLICATION
A completely bloodless field is an absolute prerequisite for accurate dissection in hand and upper extremity surgery. The intricate anatomy of the hand demands pristine visualization to avoid iatrogenic damage to microscopic vital structures, including digital nerves, vessels, and delicate tendinous insertions.
However, the inherent dangers of tourniquet use are profound. The primary risks are prolonged ischemia and mechanical compression, which can lead to devastating complications, including ischemic muscle contracture, nerve paralysis (neuropraxia or axonotmesis), and post-tourniquet syndrome.
Biomechanics and Pathophysiology of Tourniquet Injury
Because compressive pressure can be monitored and controlled with high reliability using a modern pneumatic tourniquet, complications are significantly less likely with this modality compared to primitive elastic or rubber bandage tourniquets. Nevertheless, regardless of the tourniquet system utilized, temporary or permanent complications may arise, including disproportionate or prolonged edema, joint stiffness, diminished sensibility, and motor weakness.
Based on foundational animal studies, Pedowitz et al. emphasized that tourniquet-induced neuromuscular injury is multifactorial. Biochemical, biomechanical, microvascular, and cellular mechanisms combine to produce significant tissue damage, even when tourniquets are used at clinically allowable pressures and durations.
- Biomechanical Injury: Direct mechanical compression causes edge-effect shear forces on the myelin sheaths of peripheral nerves, leading to invagination of the nodes of Ranvier and subsequent conduction block.
- Biochemical Ischemia: Prolonged arterial occlusion leads to cellular hypoxia, depletion of adenosine triphosphate (ATP), intracellular acidosis, and the accumulation of toxic metabolic byproducts.
- Reperfusion Injury: Upon tourniquet deflation, the sudden influx of oxygenated blood triggers the release of oxygen free radicals, exacerbating microvascular permeability and leading to profound interstitial edema.
Tourniquet Selection and Sizing
Improvements in biomedical engineering have resulted in the development of highly sophisticated "automatic" pneumatic tourniquets. These microprocessor-controlled devices allow the surgeon to set precise pressures within a safe therapeutic range and for specific, monitored periods of time. Integrated audiovisual alarms notify the surgeon and anesthesiologist when the preset ischemic time limit has elapsed.
Pneumatic tourniquets are available in a variety of widths and lengths, typically secured with heavy-duty Velcro strap fasteners. The selection of the cuff size is critical.
Clinical Pearl: The tourniquet cuff should be as wide as possible without interfering with the surgical field. Wider cuffs distribute the compressive force over a larger surface area, thereby requiring lower inflation pressures to achieve arterial occlusion and minimizing focal mechanical compression of the underlying nerves. Smaller, narrower cuffs are strictly reserved for pediatric patients.
STEP-BY-STEP TOURNIQUET APPLICATION AND EXSANGUINATION
The standard protocol for tourniquet application begins prior to skin preparation. Several layers of soft cast padding (e.g., Webril) are wrapped smoothly and circumferentially around the middle of the upper arm, proximal to the operative site and near the axilla.
Surgical Warning: The padding must be applied with absolute smoothness. Any wrinkles, folds, or overlaps in the padding can cause severe focal pressure points, leading to friction blisters, skin pinching, and full-thickness dermal necrosis once the cuff is inflated.
The pneumatic tourniquet is then applied tightly over the padding by the surgeon, an experienced surgical assistant, or the anesthesiologist. The tourniquet remains uninflated until all surgical preparations, draping, and incision markings have been completed.
The Exsanguination Process
For procedures performed under general anesthesia or regional block, the extremity must be thoroughly exsanguinated prior to tourniquet inflation to ensure a truly bloodless field.
Exsanguination is achieved via two primary methods:
1. Gravity Elevation: The limb is elevated at a 60-degree angle for 2 to 5 minutes. This allows venous drainage but is less effective at emptying the capillary beds.
2. Elastic Compression (Martin/Esmarch Bandage): A Martin elastic bandage (approximately 10 cm wide) is wrapped tightly around the limb, beginning distally at the fingertips and proceeding proximally in an overlapping fashion to a point just distal to the tourniquet edge.
Once the limb is exsanguinated, the pneumatic tourniquet is rapidly inflated. With modern automatic tourniquets, inflation is swift enough to instantly occlude arterial inflow, preventing the trapping of excessive venous blood in the arm during the inflation phase.
Pitfall: Wrapping the limb with an elastic bandage for exsanguination is strictly contraindicated in patients with active infections (e.g., purulent tenosynovitis, necrotizing fasciitis) or in whom malignant tumors are suspected. Mechanical compression can cause systemic dissemination of bacteria or malignant cells. In these scenarios, the limb should be exsanguinated solely by gravity elevation for 5 to 10 minutes prior to inflation.
Inflation Pressures and Time Limits
The determination of tourniquet inflation pressure must be individualized based on the patient's systolic blood pressure, limb circumference, and age.
* Adults: The inflation pressure generally should not exceed 250 to 300 mm Hg. A common evidence-based formula is to set the tourniquet pressure at 50 to 70 mm Hg above the patient's resting systolic blood pressure.
* Children: Pressures should be maintained at 250 mm Hg or lower, often calculated at 50 mm Hg above systolic pressure.
There is no absolute, universally agreed-upon rule regarding the maximum safe duration a tourniquet can remain inflated. However, extensive literature, particularly the reports of Wilgis, suggests that the required "recovery time" or revascularization interval between periods of tourniquet inflation is directly proportional to the length of the preceding ischemic period.
In standard orthopedic practice, the universally accepted safe limit for continuous tourniquet inflation is 1 to 1.5 hours (60 to 90 minutes). Exceeding this limit exponentially increases the risk of irreversible nerve paralysis and severe muscle contracture.
Management of Prolonged Procedures (The "Breathe" Protocol)
If a complex reconstructive operation is anticipated to last longer than 1.5 hours, a strict reperfusion protocol must be initiated.
1. The tourniquet is deflated and released.
2. The limb is allowed to reperfuse ("breathe") for a minimum of 15 to 20 minutes.
3. During this time, the limb is elevated, and minimal, gentle compression is applied to the open incisions using sterile dressings to control hemorrhage.
4. Following the reperfusion interval, the limb is once again exsanguinated with an elastic wrap, and the tourniquet is reinflated for the next phase of the procedure.
For exceptionally lengthy procedures, Neimkin and Smith described the use of a double tourniquet technique. This involves placing two adjacent tourniquet cuffs on the upper arm. By alternating the sites of pressure at hourly intervals, the focal mechanical compression on the underlying nerve is relieved, permitting the safe use of tourniquet ischemia for cumulative periods of up to 3.5 hours in select patients.
ANESTHESIA CONSIDERATIONS IN HAND SURGERY
While major upper extremity reconstructions are often performed under general anesthesia or brachial plexus blockade (e.g., supraclavicular or axillary blocks), many distal hand procedures can be executed flawlessly under local infiltration or specific regional nerve blocks.
Digital Nerve Blocks
For procedures isolated to the digits (e.g., trigger finger release, distal phalanx fracture pinning, nail bed repair), digital nerve blocks provide excellent, localized anesthesia without the systemic risks of general anesthesia.
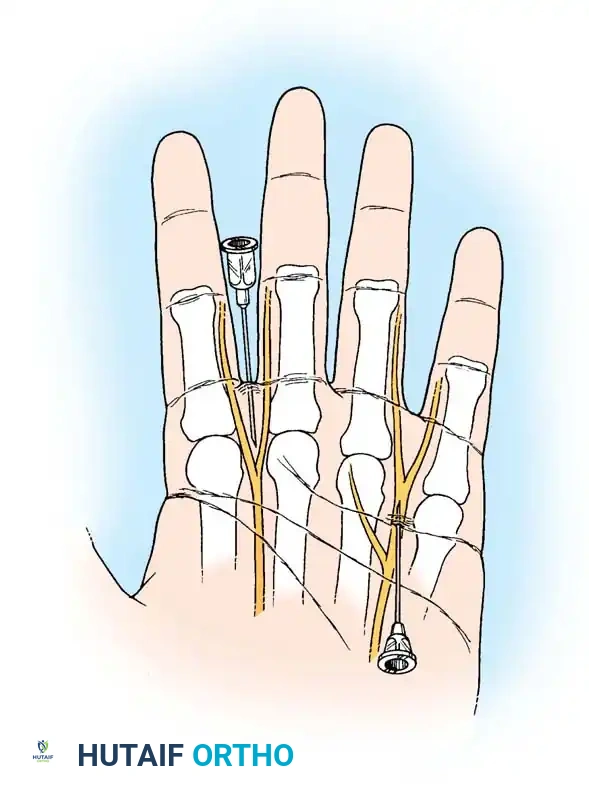
The digital block targets the proper palmar digital nerves. Using a small-gauge needle (25G or 27G), local anesthetic (typically 1% or 2% lidocaine without epinephrine, though the absolute contraindication of epinephrine in digits is currently debated in WALANT surgery) is injected into the web spaces at the base of the proximal phalanx, ensuring circumferential anesthesia of the digit.
Tourniquet Tolerance Under Local Anesthesia
When operations are performed with the patient under local anesthesia and are anticipated to last less than 30 minutes, an elastic (Martin) bandage can serve a dual purpose: exsanguination and hemostasis.
Application of the Elastic Wrap Tourniquet:
1. Wrapping begins at the fingertips and proceeds proximally up the forearm.
2. The bandage is applied in smooth layers that overlap by less than 5 to 6 mm.
3. When the mid-forearm is reached, four or five layers of the elastic bandage are overlapped directly on top of one another. Wrinkles must be strictly avoided.
4. The pressure is incrementally increased with each layer so that only moderate stretching of the bandage is required.
5. The bandage is then unwrapped, beginning distally at the hand and proceeding up to the mid-forearm. The overlapped layers in the mid-forearm are left in place to act as the tourniquet until the operation is finished.
For procedures performed with local infiltration or wrist block anesthesia, a standard pneumatic tourniquet can also be utilized. The tourniquet can be applied either above the elbow or just below the elbow (forearm tourniquet). An awake patient can typically tolerate an inflated pneumatic tourniquet for up to 30 minutes before experiencing extreme ischemic discomfort (tourniquet pain).
Ogufere, Giddins, and Thom assessed the perception of arm tourniquet pain in 100 patients undergoing procedures under local anesthesia. Their findings demonstrated that for procedures lasting 20 minutes or less, 99% of patients tolerated the tourniquet exceptionally well without the need for supplemental intravenous sedation.
COMPLICATIONS AND POSTOPERATIVE PROTOCOLS
The responsibility of the surgeon does not end with the deflation of the tourniquet. Immediate postoperative management of the limb is critical to preventing delayed complications.
When the operation is complete and the tourniquet has been released, both the pneumatic cuff and the underlying cotton wrapping (Webril) must be removed immediately. Leaving a deflated, tight cuff or blood-soaked padding around the arm acts as a venous tourniquet, causing severe venous congestion, exacerbating postoperative edema, and increasing the risk of hematoma formation at the surgical site.
Furthermore, Flatt emphasized the critical need for routine maintenance of surgical equipment. The calibration of the pressure indicator gauges on older-design pneumatic tourniquets must be checked regularly against a standard mercury manometer. Extreme, unrecorded pressures caused by a faulty, uncalibrated gauge—even over a short operative period—can cause devastating crush injuries to the peripheral nerves, resulting in profound paralysis that may require months of intensive rehabilitation for recovery, or may result in permanent deficit.
By adhering to these rigorous, evidence-based protocols for preparation, draping, and tourniquet management, the orthopedic surgeon ensures an optimal operative environment while safeguarding the functional integrity of the patient's upper extremity.
You Might Also Like

