Comprehensive Introduction and Patho-Epidemiology
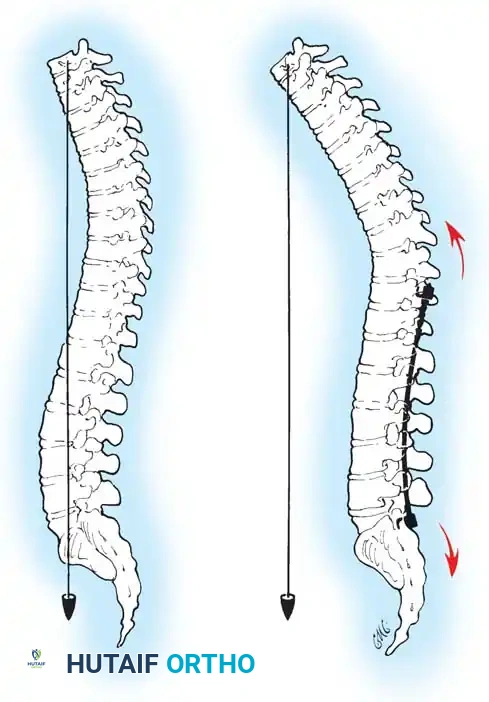
Adolescent Idiopathic Scoliosis (AIS) represents a complex, three-dimensional structural deformity of the spine characterized by coronal curvature, sagittal plane alteration, and axial vertebral rotation. The posterior approach to the spinal column remains the most universally utilized, versatile, and biomechanically sound corridor for the surgical management of this formidable pathology. Familiar to all fellowship-trained orthopaedic spine surgeons, this extensile approach offers safe, comprehensive exposure of the entire vertebral column from the upper thoracic spine to the sacropelvic junction. It facilitates the application of modern multi-segmental pedicle screw constructs, allows for aggressive posterior column osteotomies (such as Ponte or Smith-Petersen osteotomies), and provides a massive surface area for robust, lifelong arthrodesis.
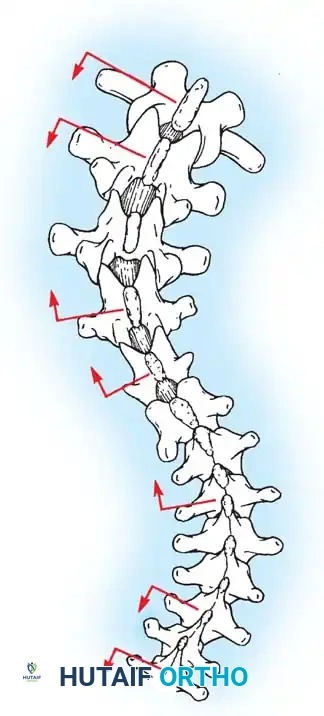
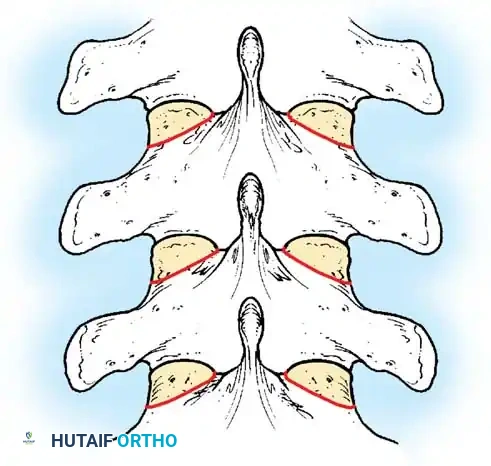
The patho-epidemiology of AIS is fundamentally rooted in the Hueter-Volkmann principle, wherein asymmetric mechanical loading across the vertebral endplates exacerbates asymmetric longitudinal growth. While the exact etiology remains elusive—spanning genetic, neurohormonal, and biomechanical theories—the clinical manifestation is predictably progressive during periods of rapid skeletal acceleration, particularly the adolescent growth spurt. The prevalence of AIS in the general at-risk population is approximately 2% to 3%, though curves progressing to a magnitude necessitating surgical intervention (typically >45 to 50 degrees) occur in only about 0.1% to 0.3% of adolescents. Understanding this epidemiological framework is critical for the spine surgeon, as it dictates the timing of surgical intervention relative to the patient's skeletal maturity, typically assessed via the Risser sign or Sanders maturity scale.
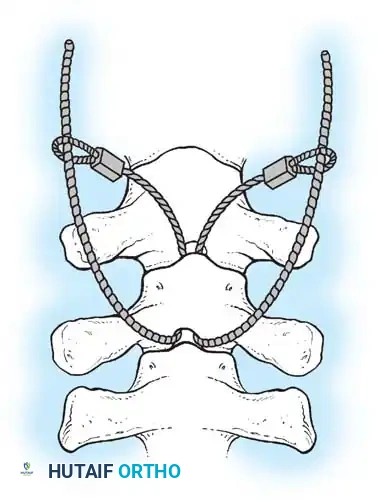
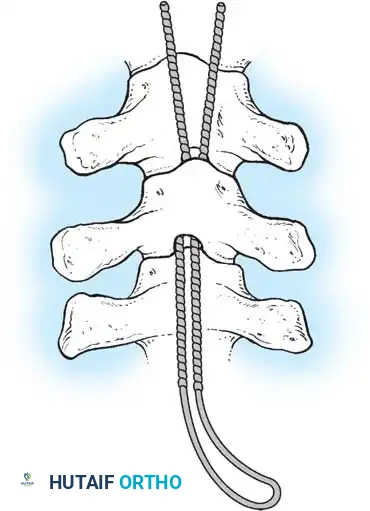
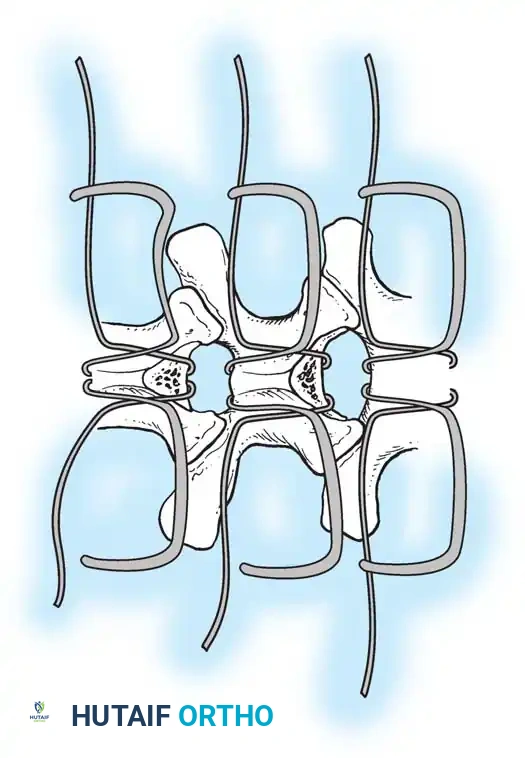
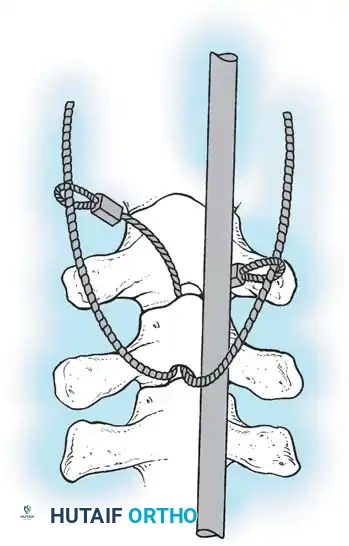
The long-term success of any operative procedure for idiopathic scoliosis is fundamentally predicated on achieving a solid, mature arthrodesis. While modern instrumentation provides immediate biomechanical stability and dramatic intraoperative deformity correction, it is the biological fusion that ensures lifelong maintenance of alignment and prevents hardware failure. Historically, the evolution of posterior scoliosis surgery transitioned from non-instrumented cast corrections to Harrington rod distraction, then to segmental hook-and-wire constructs (Cotrel-Dubousset), and finally to the current gold standard: all-pedicle screw constructs. This evolution has dramatically improved our ability to control the spine in all three planes, particularly enhancing axial derotation and sagittal profile restoration.
Despite these technological advancements, the biological imperative remains unchanged. The surgeon must meticulously balance the biomechanical forces of correction with the biological requirements of bone healing. This requires a profound understanding of spinal vascularity, osteogenesis, and the local mechanical environment. A beautifully instrumented spine that fails to fuse will inevitably result in pseudarthrosis, hardware breakage, loss of correction, and profound clinical morbidity requiring complex revision surgery. Therefore, the masterclass in posterior scoliosis surgery is not merely in the placement of titanium, but in the meticulous preparation of the host bed to ensure a definitive biological union.
Detailed Surgical Anatomy and Biomechanics
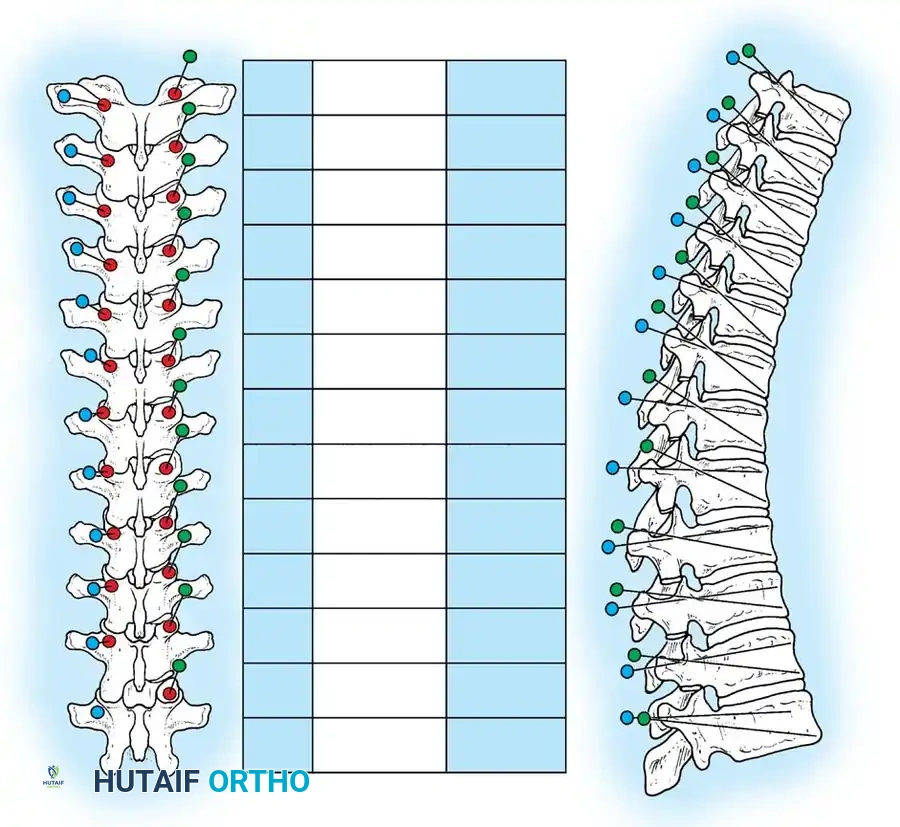
A profound, three-dimensional spatial awareness of spinal osteology, ligamentous structures, and neurovascular anatomy is the sine qua non of safe posterior spinal surgery. The thoracic spine presents unique anatomical challenges due to its kyphotic alignment, the presence of the rib cage, and the narrow morphometry of the thoracic pedicles. The thoracic facets are oriented primarily in the coronal plane, which permits lateral bending and rotation but restricts flexion and extension. In contrast, the lumbar facets are oriented in the sagittal plane, facilitating flexion and extension while restricting axial rotation. Recognizing these transitional changes at the thoracolumbar junction is critical when performing facetectomies, osteotomies, and determining pedicle screw trajectories.
The muscular anatomy encountered during the posterior approach consists of superficial, intermediate, and deep layers. The deep paraspinal musculature, primarily the erector spinae (spinalis, longissimus, iliocostalis) and the transversospinales group (multifidus, rotatores), must be meticulously elevated subperiosteally to minimize hemorrhagic morbidity and muscle denervation. The vascular supply to these muscles and the posterior elements is derived from the dorsal branches of the posterior intercostal and lumbar arteries. These segmental vessels course laterally and send branches medially, passing just lateral to the pars interarticularis and facet joints. Inadvertent transection of these vessels during lateral dissection can lead to brisk, insidious bleeding that obscures the surgical field and increases overall blood loss.
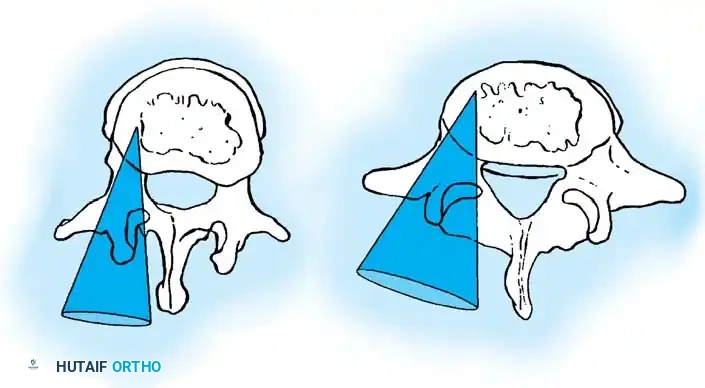
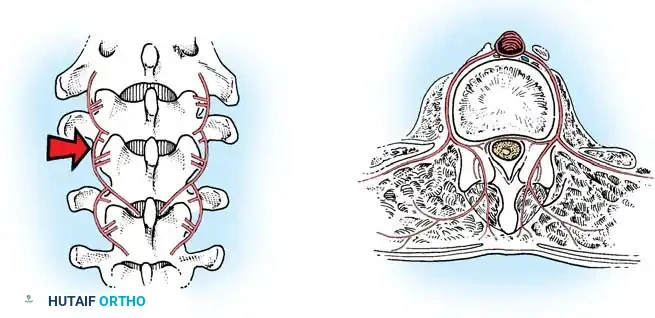
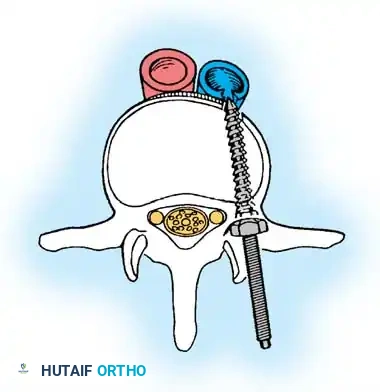
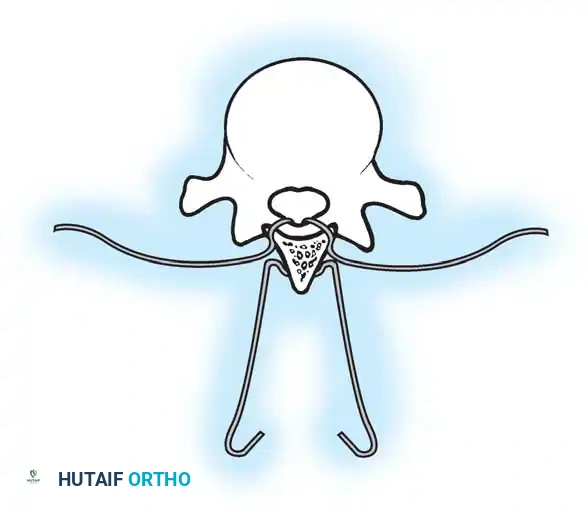
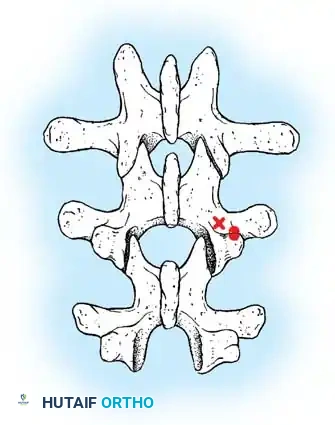
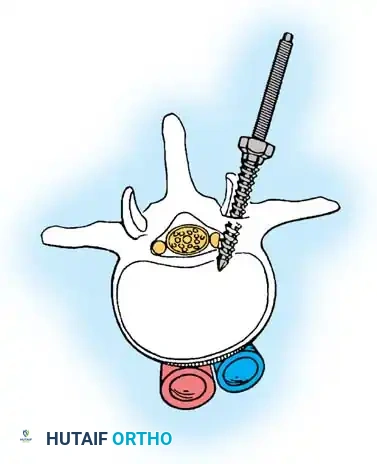
Neurologically, the proximity of the spinal cord in the thoracic region leaves virtually no margin for error during instrumentation. The thoracic spinal canal is relatively narrow, and the cord occupies a significant portion of the available space. Furthermore, the vascular watershed zone of the thoracic spinal cord (typically T4-T9) makes it exquisitely sensitive to hypoperfusion or mechanical compression. In the scoliotic spine, the spinal cord migrates toward the concavity of the curve, altering its typical anatomic relationship to the pedicles. Medial cortical breaches during pedicle screw preparation on the concave side carry a catastrophic risk of direct spinal cord injury, while lateral breaches risk injury to the pleura, lungs, or great vessels (particularly the aorta on the left side).
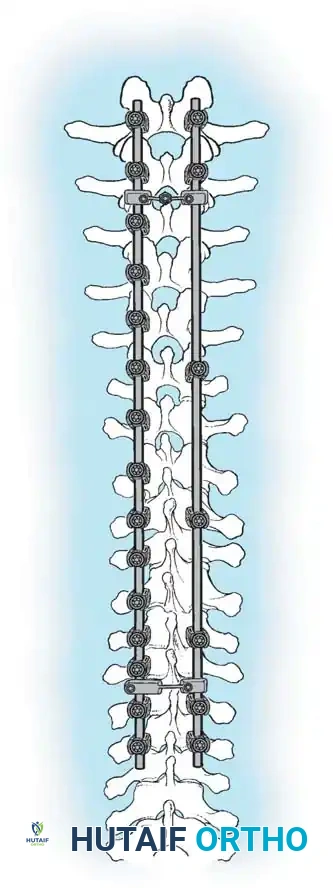
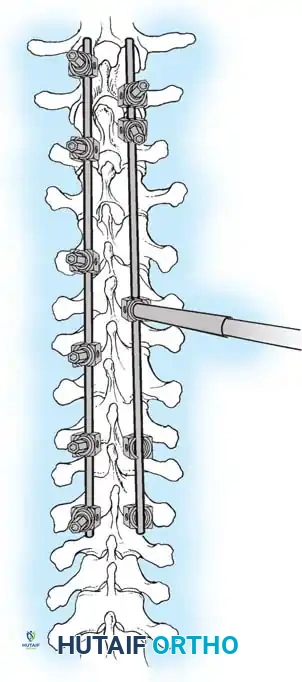
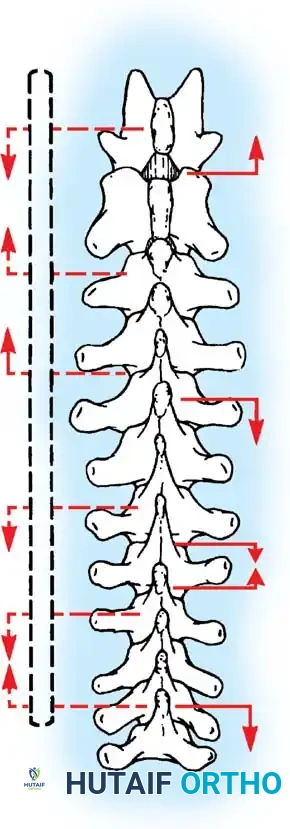
Biomechanically, modern all-pedicle screw constructs provide rigid three-column fixation, allowing for powerful deformity correction through multiple mechanisms: rod derotation, direct vertebral translation, compression, distraction, and cantilever forces. Pedicle screws bypass the posterior elements and anchor directly into the vertebral body, providing superior pull-out strength compared to hooks or sublaminar wires. This rigid fixation neutralizes micromotion across the instrumented segments, creating an optimal mechanical environment for bone graft incorporation. However, the immense stiffness of these constructs alters the biomechanics of the adjacent uninstrumented segments, necessitating meticulous pre-operative planning to select the appropriate upper and lower instrumented vertebrae (UIV and LIV) to prevent proximal junctional kyphosis (PJK) or distal adding-on.
Exhaustive Indications and Contraindications
The decision to proceed with posterior spinal fusion in an adolescent with idiopathic scoliosis is a highly nuanced process that synthesizes curve magnitude, skeletal maturity, curve progression, and the patient's psychosocial context. The primary indication for surgical intervention is a coronal Cobb angle exceeding 45 to 50 degrees in a growing child, or a curve exceeding 50 degrees in a skeletally mature adolescent. Curves of this magnitude have a high natural history of continued progression into adulthood (typically 1 to 2 degrees per year), which can lead to severe cosmetic deformity, truncal shift, coronal decompensation, and eventually, restrictive pulmonary disease and cor pulmonale in severe thoracic curves (>90 degrees).
Beyond simple coronal magnitude, the sagittal profile plays a crucial role in surgical decision-making. AIS is classically associated with thoracic hypokyphosis or true lordosis. Restoring normal thoracic kyphosis is a primary goal of modern instrumentation to optimize pulmonary mechanics and prevent secondary cervical kyphosis. Furthermore, the curve pattern dictates the surgical approach. While the vast majority of Lenke 1 through 6 curves are amenable to an isolated posterior approach, extremely rigid, large magnitude curves (>75-80 degrees) may occasionally require an anterior release or aggressive posterior column osteotomies (Ponte/Smith-Petersen) to achieve adequate flexibility for correction.
Contraindications to posterior spinal fusion for AIS are generally relative and center around severe medical comorbidities that preclude safe anesthesia, or active local/systemic infections. However, a critical diagnostic contraindication to proceeding with a standard AIS protocol is the presence of an atypical curve pattern (e.g., left thoracic curve, short angular curve, absence of apical lordosis, or rapid progression). These features strongly suggest an underlying neurogenic or syndromic etiology (such as a syrinx, Chiari malformation, or tethered cord). In such cases, an MRI of the entire neural axis is mandatory, and the underlying neurosurgical pathology must be addressed prior to any structural deformity correction.
| Category | Indications for Posterior Spinal Fusion in AIS | Absolute & Relative Contraindications |
|---|---|---|
| Curve Magnitude | Coronal Cobb angle > 45°-50° in immature patients. | Mild to moderate curves (< 40°) effectively managed with bracing. |
| Progression | Documented progression despite compliant orthotic management. | Skeletally mature patients with stable curves < 45°. |
| Sagittal Profile | Severe thoracic hypokyphosis/lordosis requiring structural restoration. | Severe, rigid hyperkyphosis requiring combined anterior/posterior approach (relative). |
| Neurological | Normal neural axis confirmed on clinical exam or MRI. | Untreated intraspinal anomalies (syrinx, tethered cord, Chiari malformation). |
| Medical/Host | Medically optimized for major reconstructive surgery and blood loss. | Active systemic infection, severe malnutrition, or uncorrectable coagulopathy. |
Pre-Operative Planning, Templating, and Patient Positioning
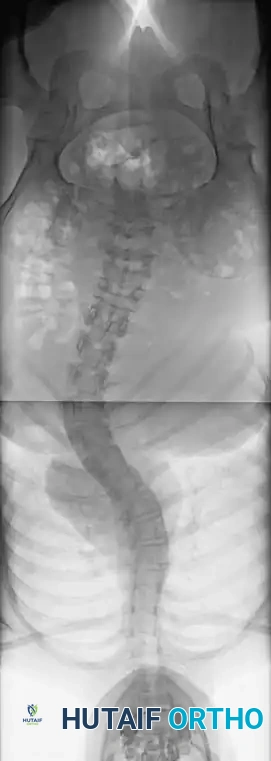
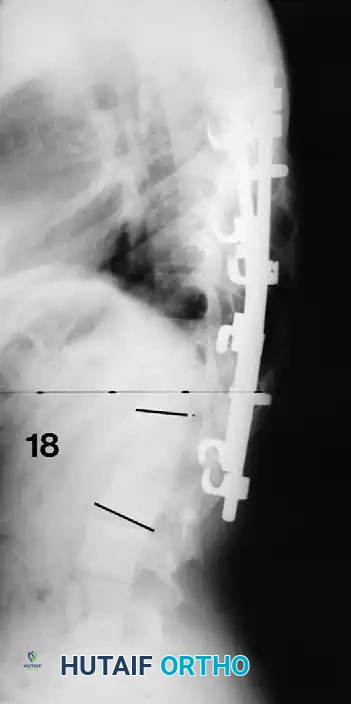
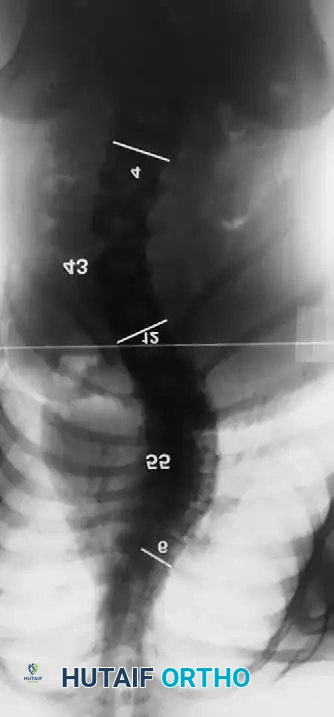
Meticulous pre-operative planning is the foundation of a successful scoliosis correction. This process begins with high-quality, standing full-length posteroanterior (PA) and lateral radiographs (preferably utilizing low-dose EOS imaging to minimize radiation exposure). Flexibility films, including supine side-bending, fulcrum bending, or traction radiographs, are essential to assess curve rigidity, differentiate structural from non-structural curves, and determine the anticipated flexibility of the spine. The Lenke Classification system is rigorously applied to define the curve type (1-6), lumbar spine modifier (A, B, C), and sagittal thoracic modifier (-, N, +), which systematically guides the selection of fusion levels.

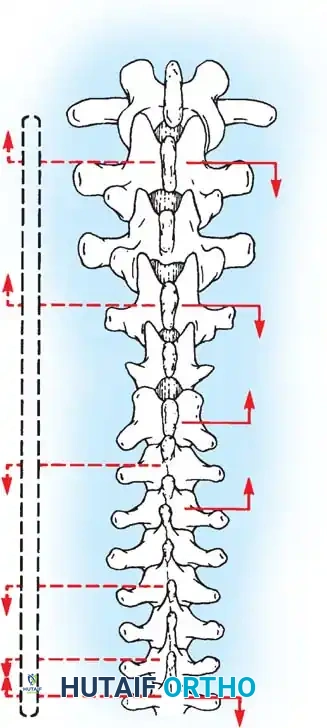
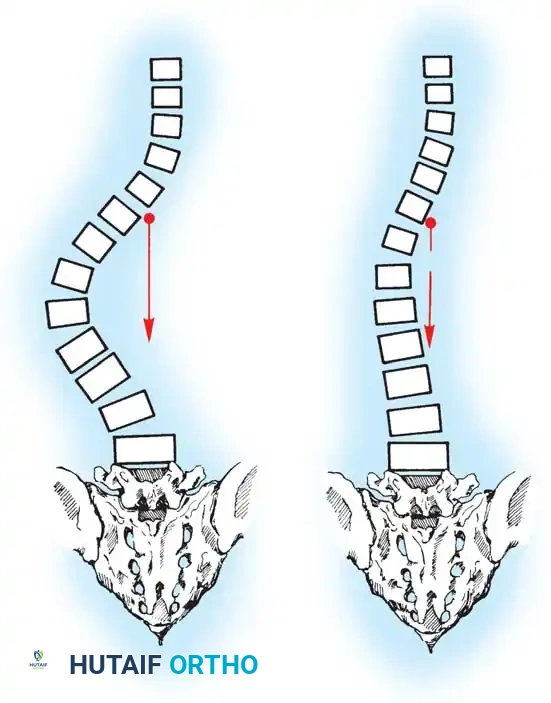
Selecting the Upper Instrumented Vertebra (UIV) and Lower Instrumented Vertebra (LIV) is arguably the most intellectually demanding aspect of the procedure. The UIV must be chosen to ensure the shoulders remain level postoperatively, often extending to T2 or T3 for double thoracic curves, or T4/T5 for main thoracic curves. The LIV must be selected to stabilize the spine over the center of the sacrum, typically stopping at the "stable vertebra" or the "touched vertebra" on the bending films. Stopping short of the stable vertebra risks distal adding-on, while fusing unnecessarily low (into the lower lumbar spine) sacrifices critical lumbar motion segments, predisposing the patient to premature adjacent segment degeneration and flatback syndrome.
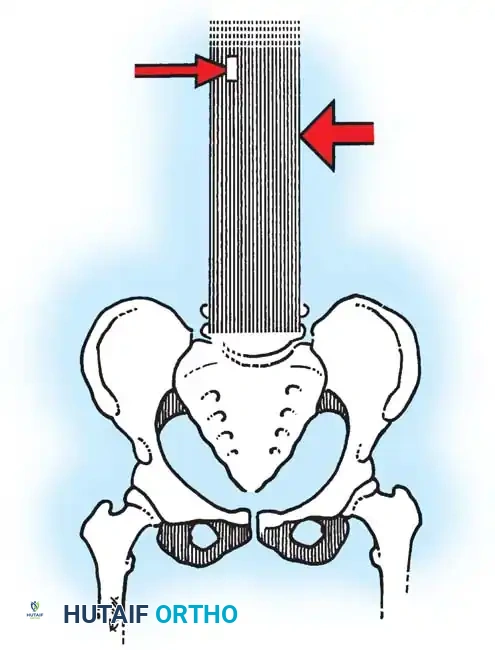
Patient positioning is the first, and often most critical, physical step in the operating room. The patient is carefully rolled prone onto an open-frame Jackson table (e.g., Mizuho OSI). The open frame is paramount as it allows the abdomen to hang completely free. Eliminating intra-abdominal pressure prevents compression of the inferior vena cava. This directly reduces venous engorgement within Batson’s epidural venous plexus, drastically minimizing intraoperative blood loss during subperiosteal exposure, facetectomies, and pedicle cannulation. The arms must be meticulously supported on arm boards with all bony prominences (especially the elbows and ulnar nerves) heavily padded, ensuring shoulder abduction does not exceed 90 degrees to prevent brachial plexus neuropraxia.
Sagittal Profile Optimization during Positioning
When a patient is positioned prone with the hips flexed, physiological lumbar lordosis is artificially obliterated. If the planned fusion extends into the lower lumbar spine (L3, L4, or L5), it is imperative to elevate the knees and thighs so the hip joints are fully extended. This maneuver restores and mechanically locks in normal lumbar lordosis on the operating table. Fusing the lumbar spine in a hypolordotic or flatback position is a catastrophic biomechanical error that forces the patient into a positive sagittal balance, leading to chronic, debilitating back pain, compensatory hip/knee flexion, and the eventual need for massive revision osteotomies (e.g., Pedicle Subtraction Osteotomies).
Step-by-Step Surgical Approach and Fixation Technique
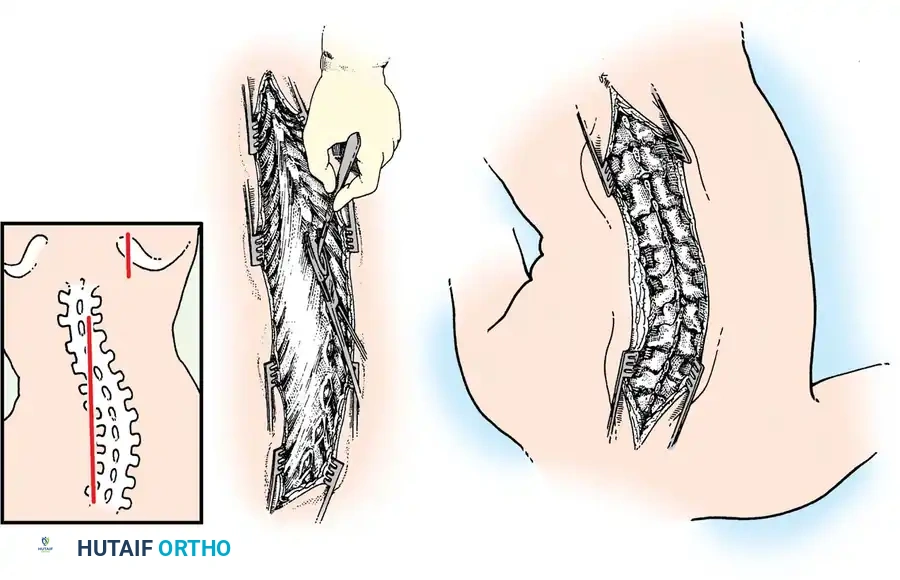
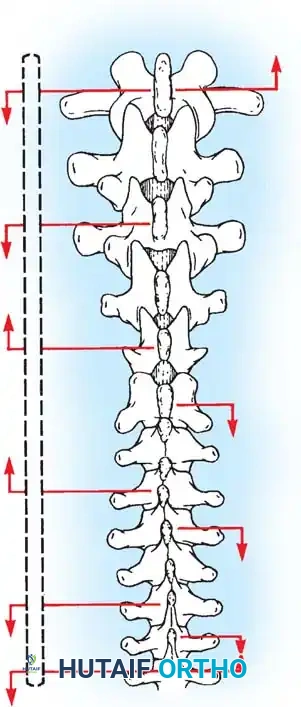
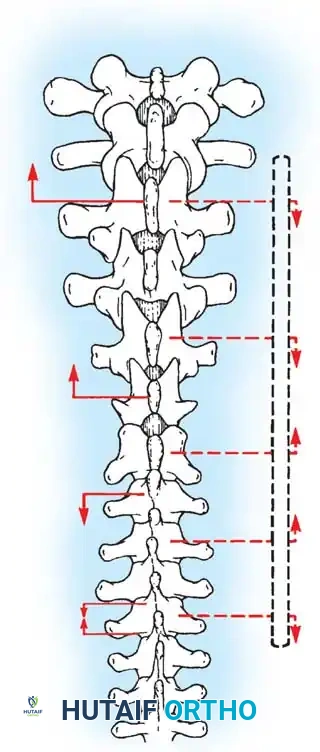
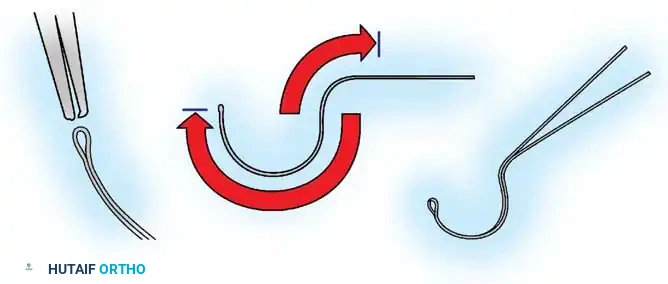
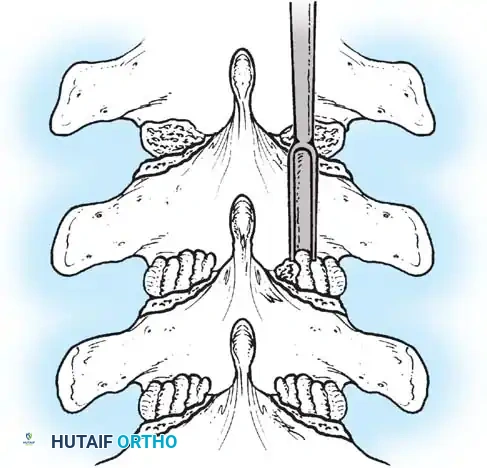
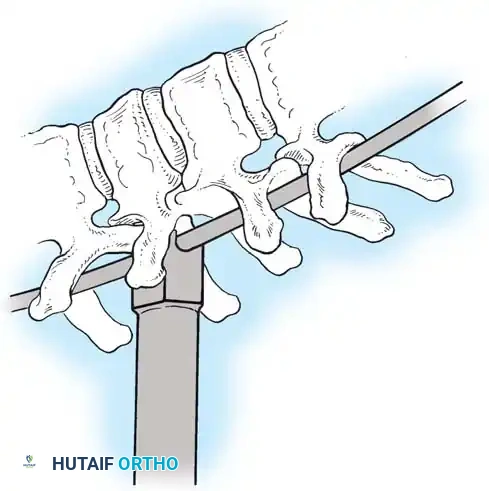
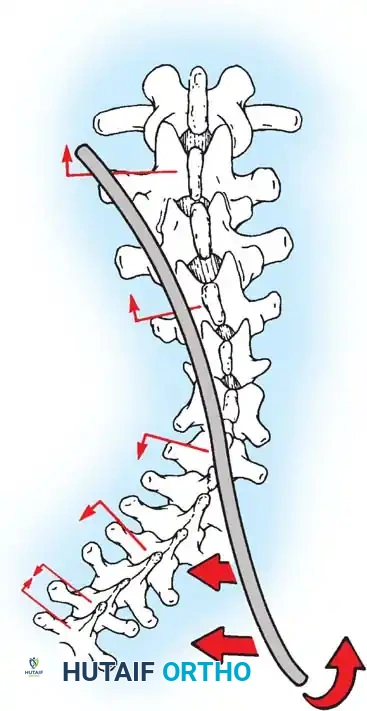
A bloodless, efficient exposure sets the tone for the entire reconstructive procedure. The skin is incised in a perfectly straight midline trajectory from one vertebra above the UIV to one below the LIV. The superficial dissection is carried down through the subcutaneous fat to the avascular midline raphe. Utilizing a Cobb elevator combined with precise electrocautery, the spinous processes are exposed subperiosteally. The direction of dissection is critical: the surgeon must dissect from caudad to cephalad. The short rotator muscles (multifidus and rotatores) and ligaments of the spine attach obliquely, pointing superomedially. Sweeping upward works with the grain of these fibers, allowing for a cleaner, faster subperiosteal release while minimizing muscle tearing and bleeding.
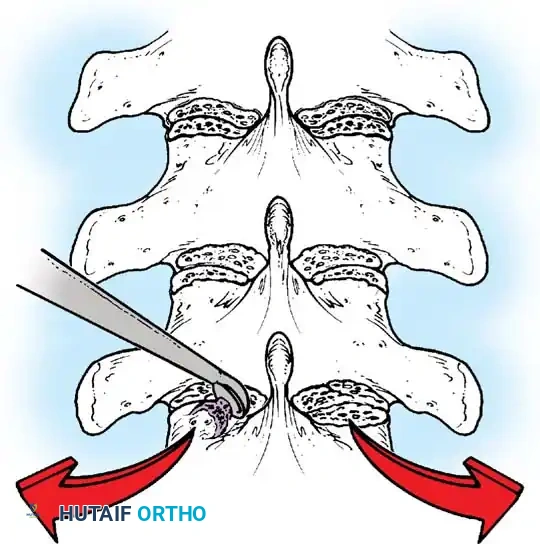
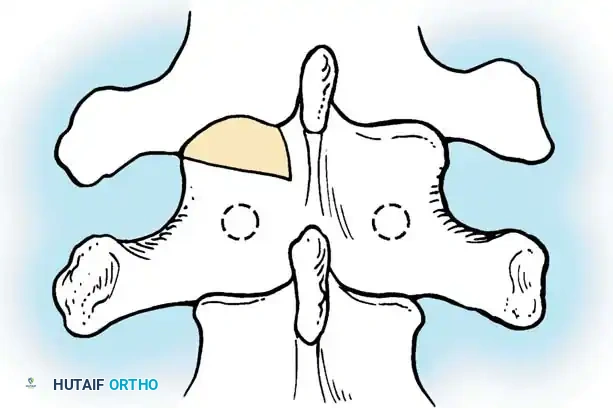
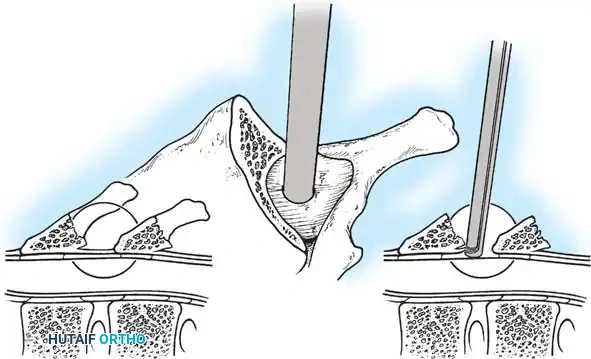
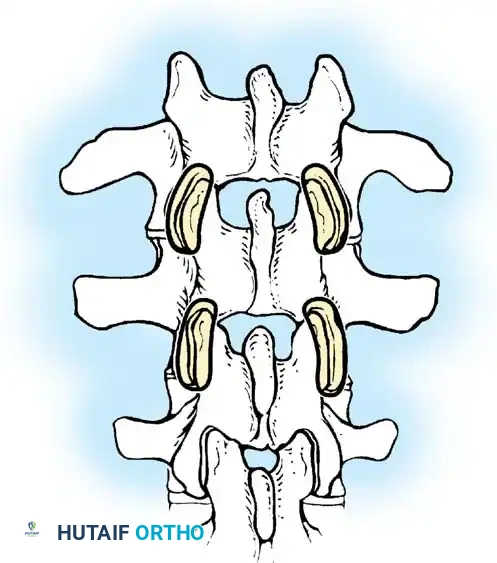
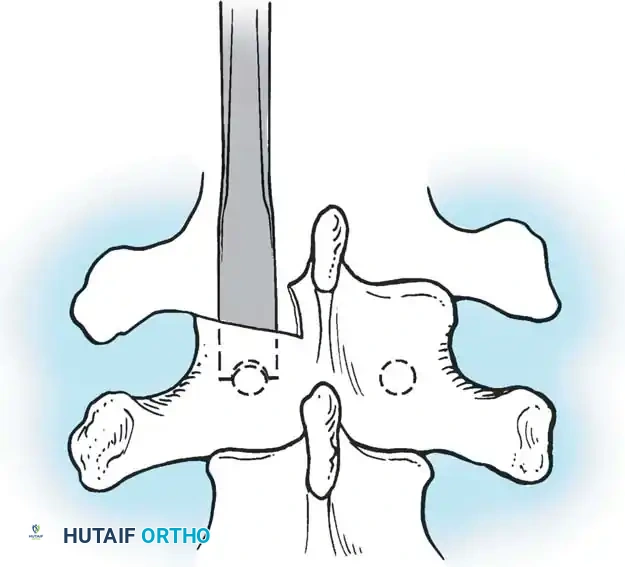
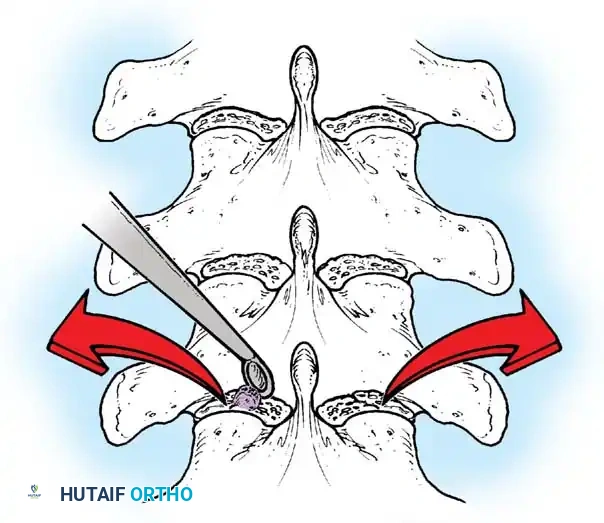
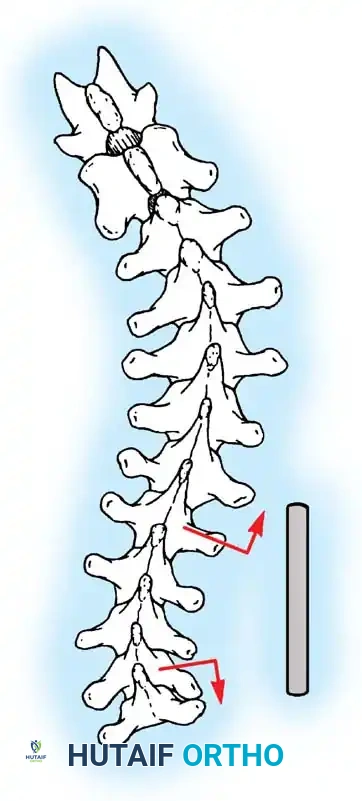
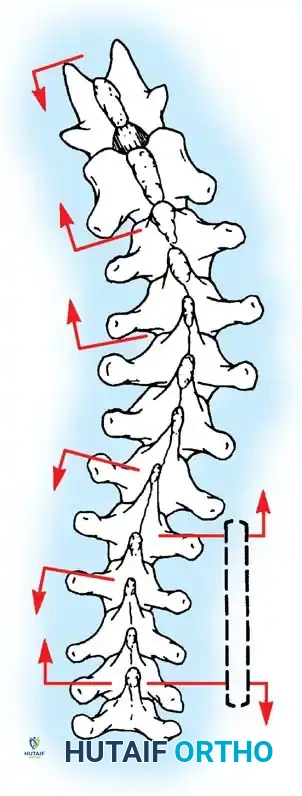
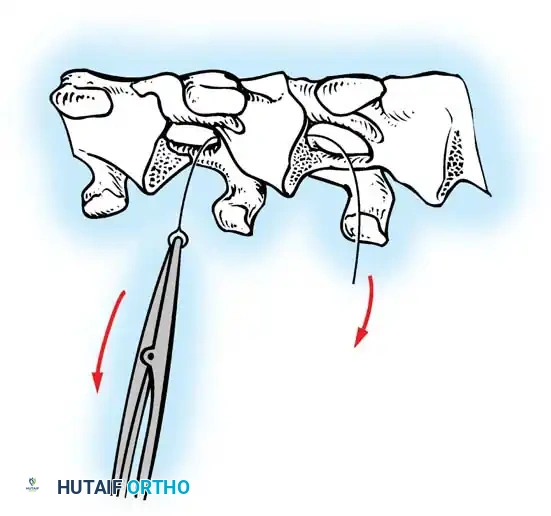
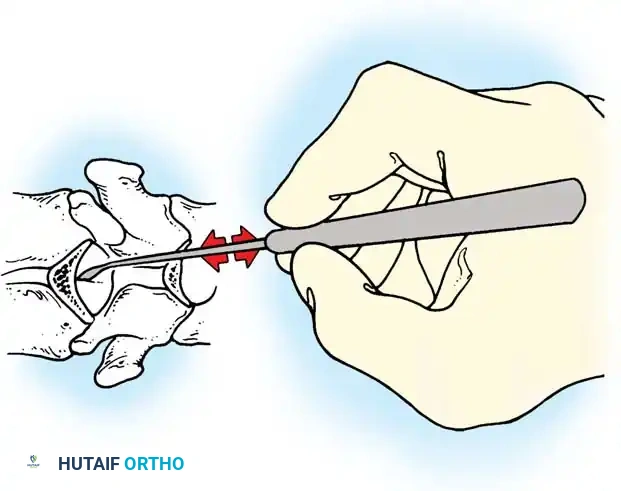
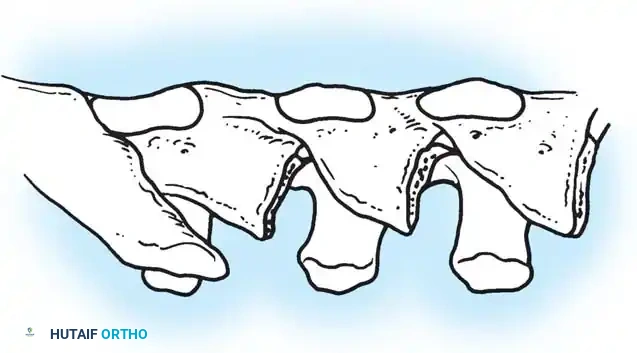
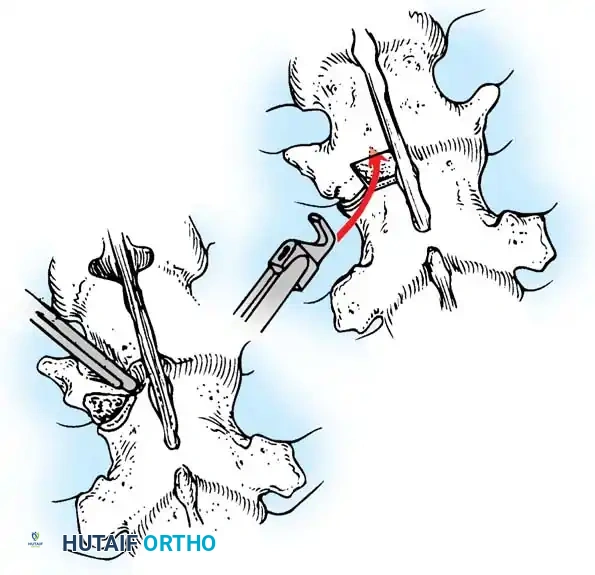
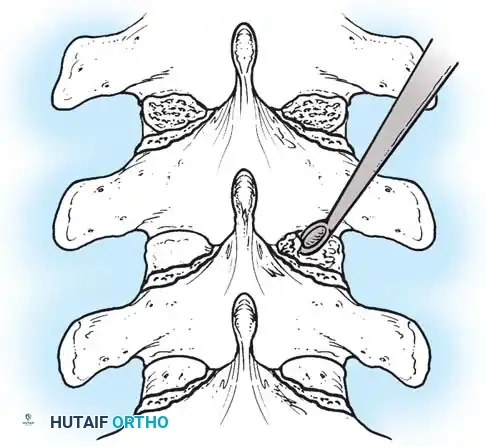
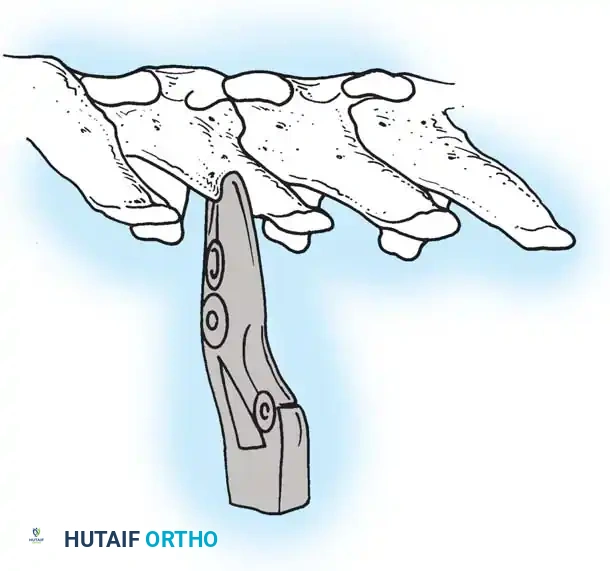
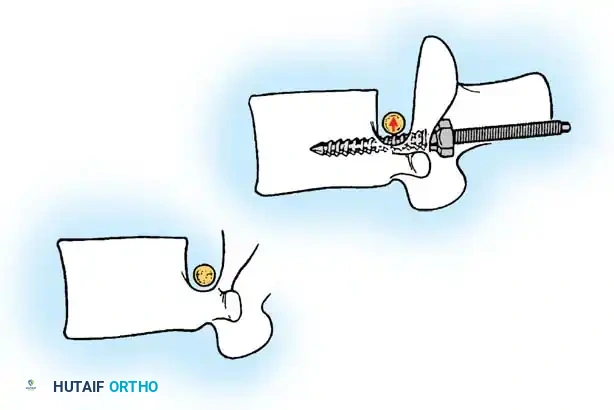
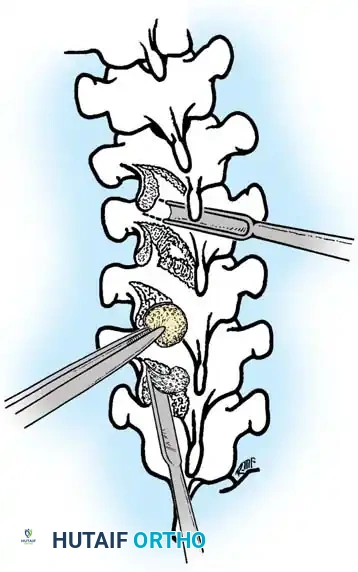
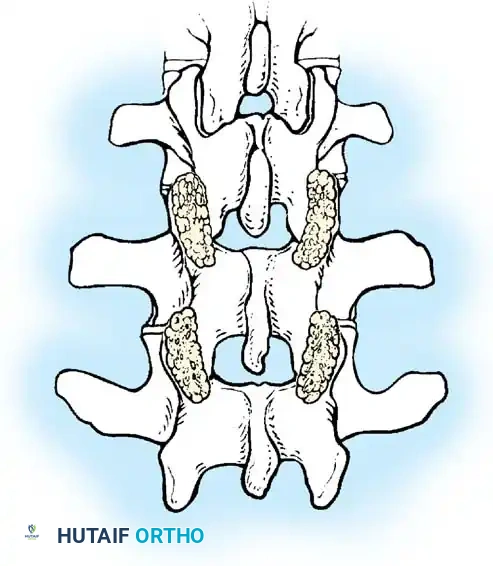
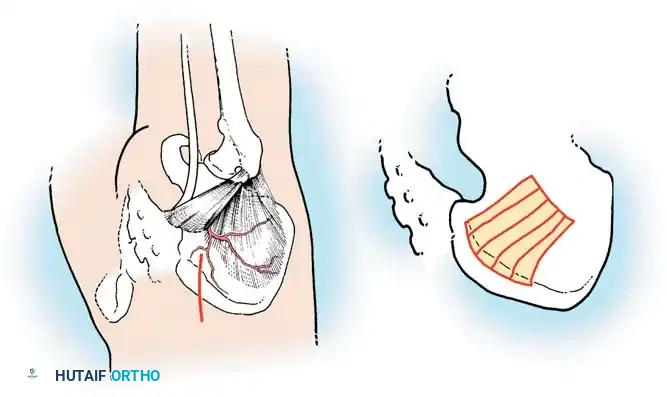
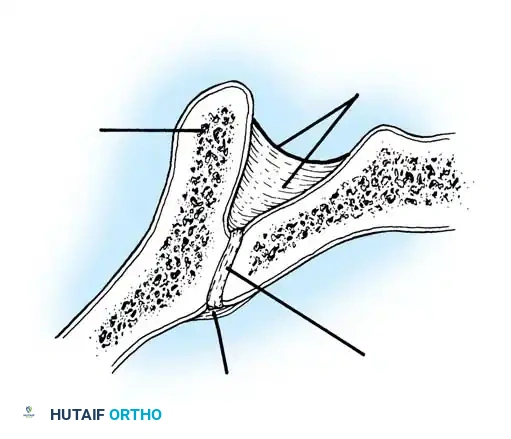
Once the spine is exposed to the tips of the transverse processes bilaterally, meticulous facetectomies are performed. This serves a dual purpose: it significantly increases the flexibility of the spine for subsequent deformity correction, and it provides a highly vascularized bed for intra-articular arthrodesis. The Moe technique or the Hall technique can be utilized depending on surgeon preference and regional anatomy. In the thoracic spine, the coronal orientation of the facets allows for the creation of hinged bone flaps. The cartilage is completely denuded using sharp curets and pituitary rongeurs, and the resulting defect is packed tightly with cancellous bone graft.
Pedicle Screw Insertion
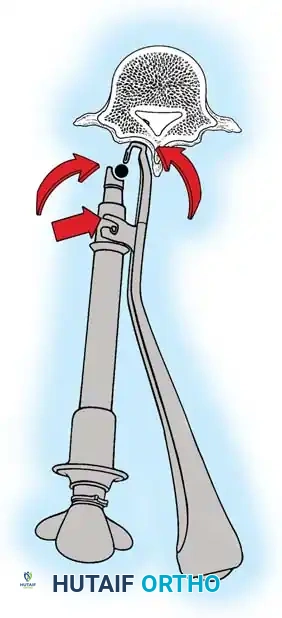
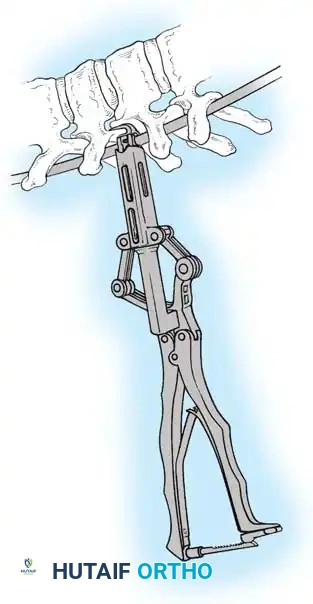
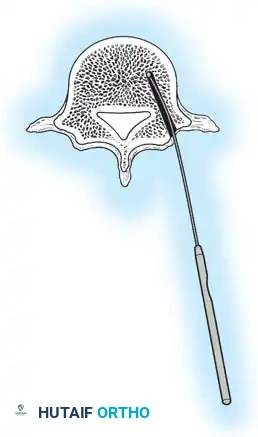
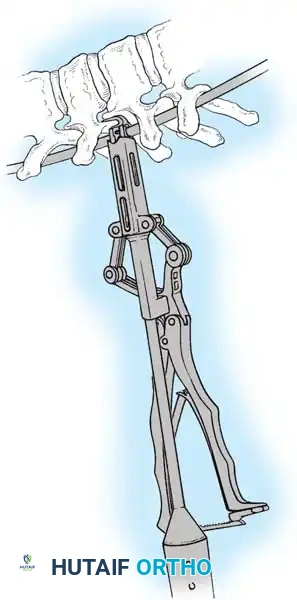
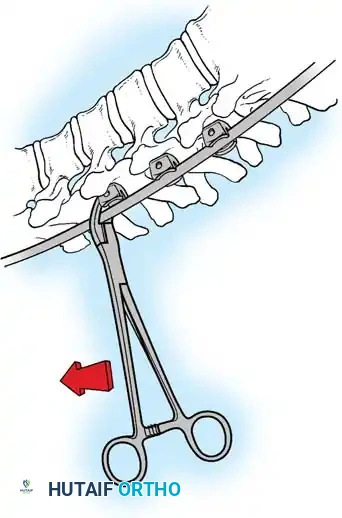
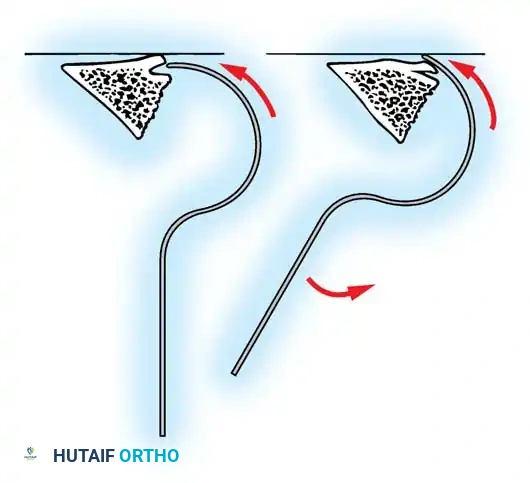
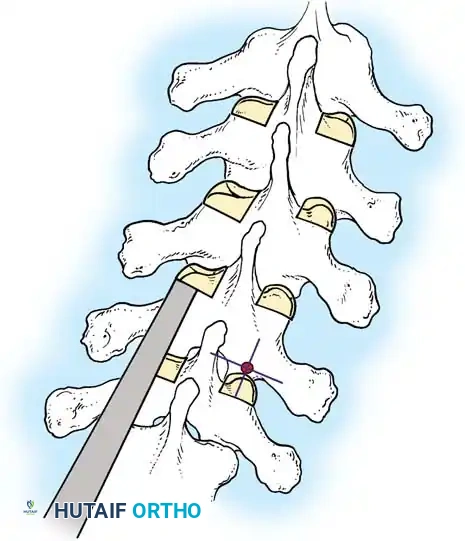
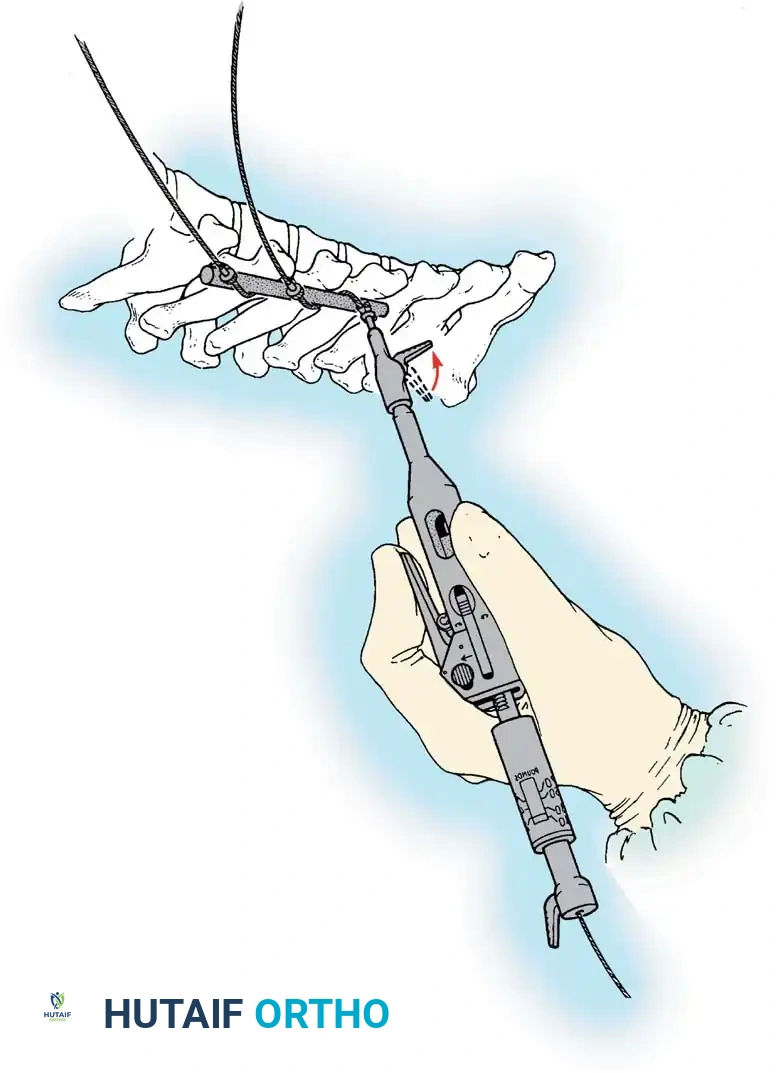
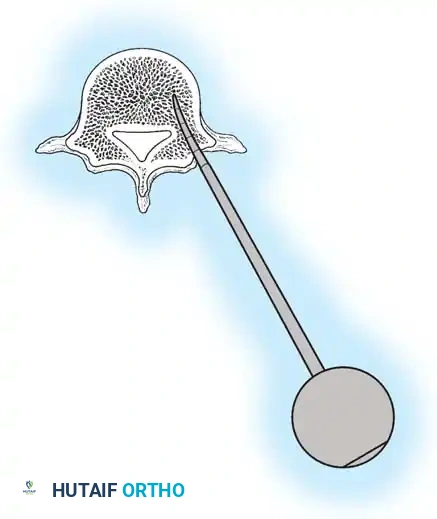
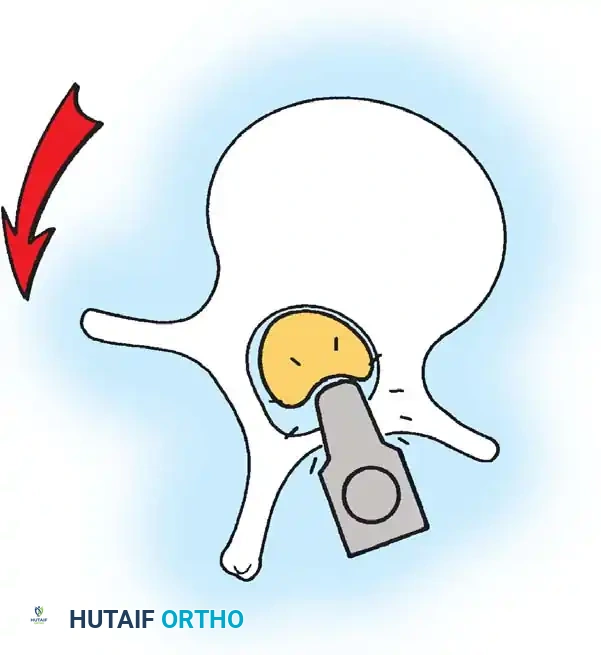
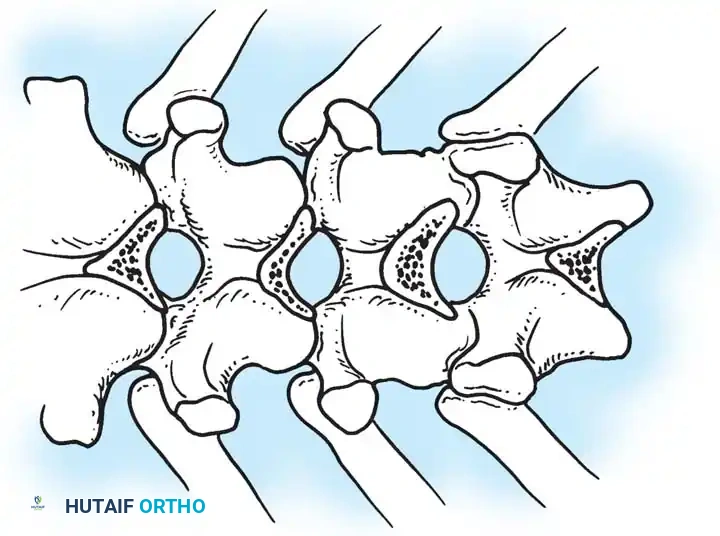
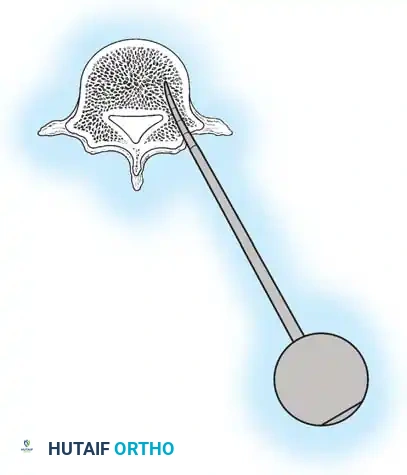
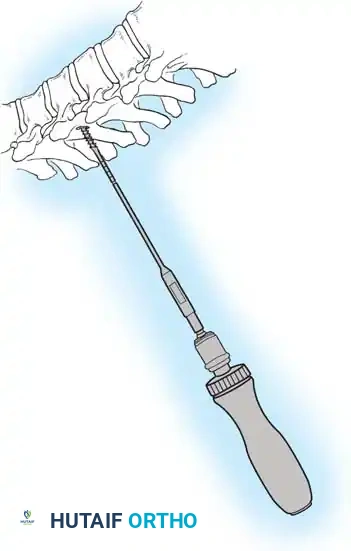
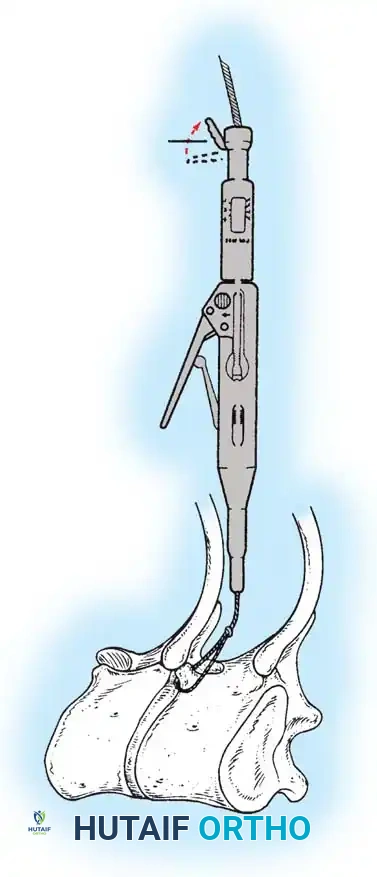
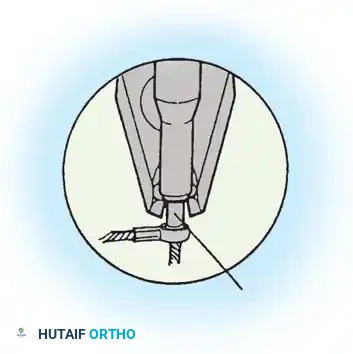
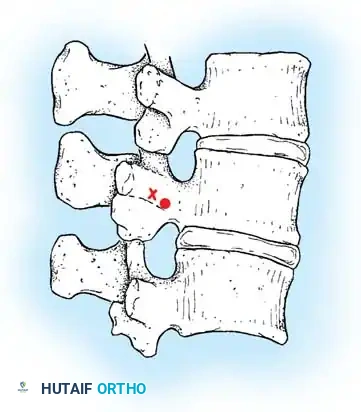
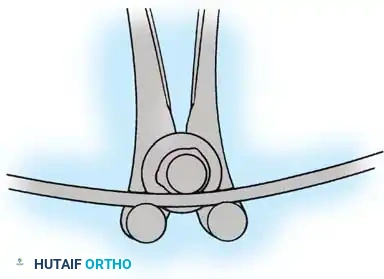
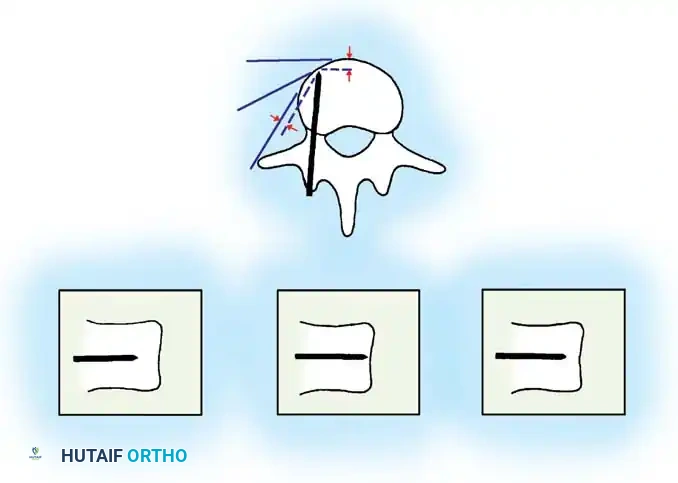
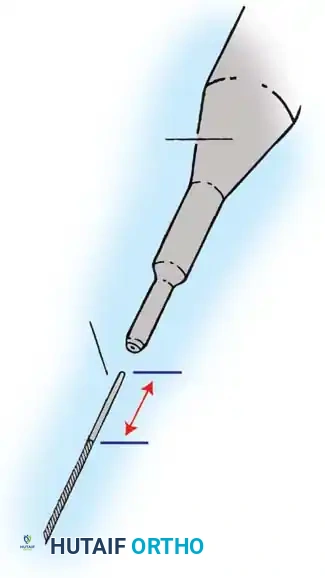
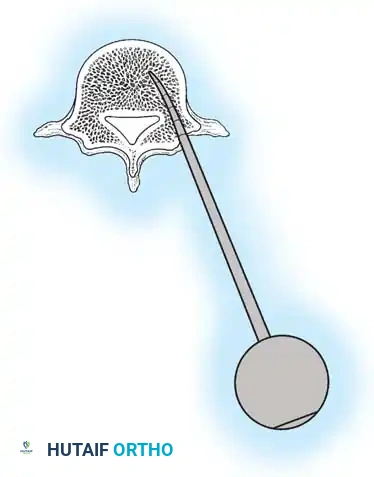
Pedicle screw insertion in the deformed scoliotic spine demands profound anatomical knowledge and tactile feedback. The freehand technique remains the gold standard, though fluoroscopic, navigated, and robotic assistance are increasingly utilized. The starting point for a thoracic pedicle screw is typically at the intersection of the bisected transverse process and the lateral border of the superior articular facet. A burr or awl breaches the cortical bone. A curved pedicle probe (gearshift) is then advanced through the cancellous core of the pedicle, initially pointing laterally to avoid medial cortical breach into the spinal canal, and then rotated medially to enter the vertebral body.
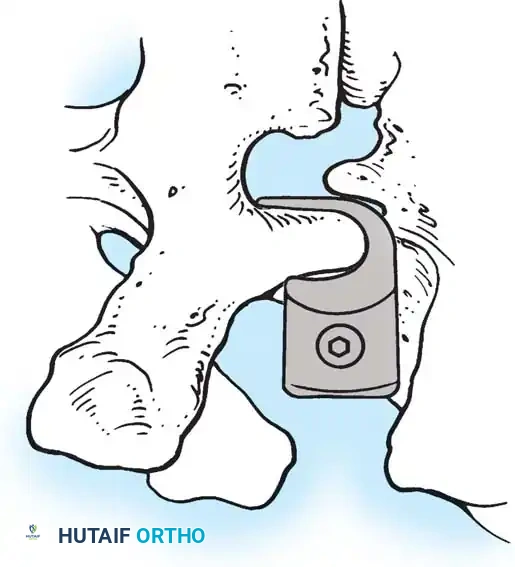
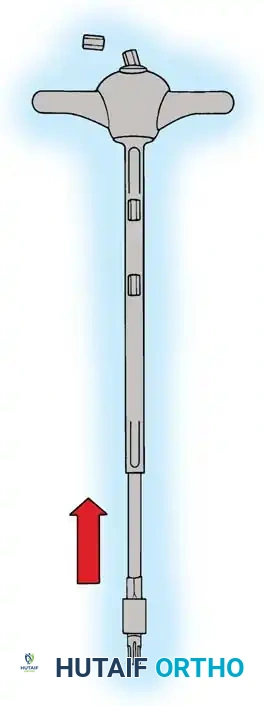
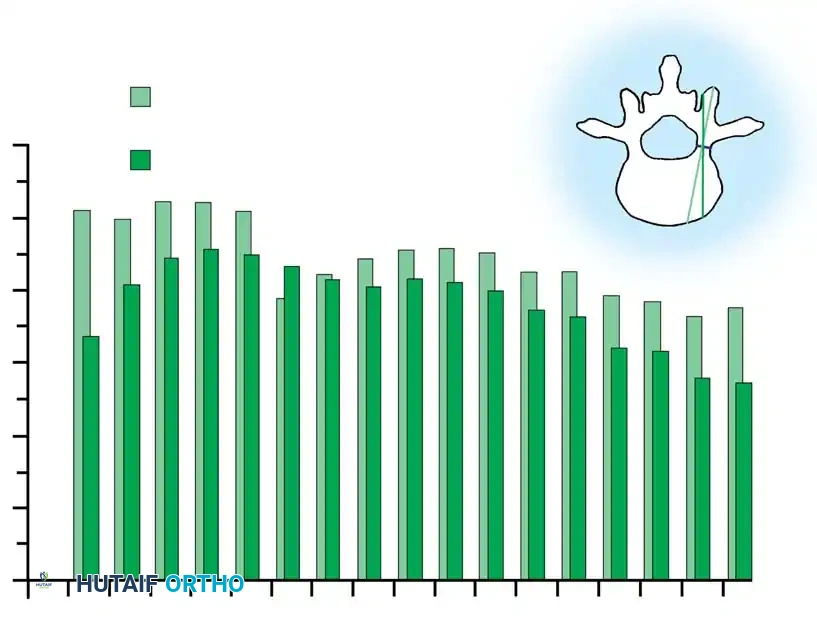
The trajectory is continuously verified using a flexible ball-tip probe to palpate the five bony walls of the pedicle tract (medial, lateral, superior, inferior, and anterior). The tract is then tapped, palpated again, and the appropriate length and diameter titanium or cobalt-chrome screw is inserted. In severe deformities, apical vertebral rotation severely distorts normal landmarks. The concave pedicles at the apex are often sclerotic, dysmorphic, and extremely narrow, requiring meticulous preparation to avoid catastrophic medial breaches.

Deformity Correction Maneuvers
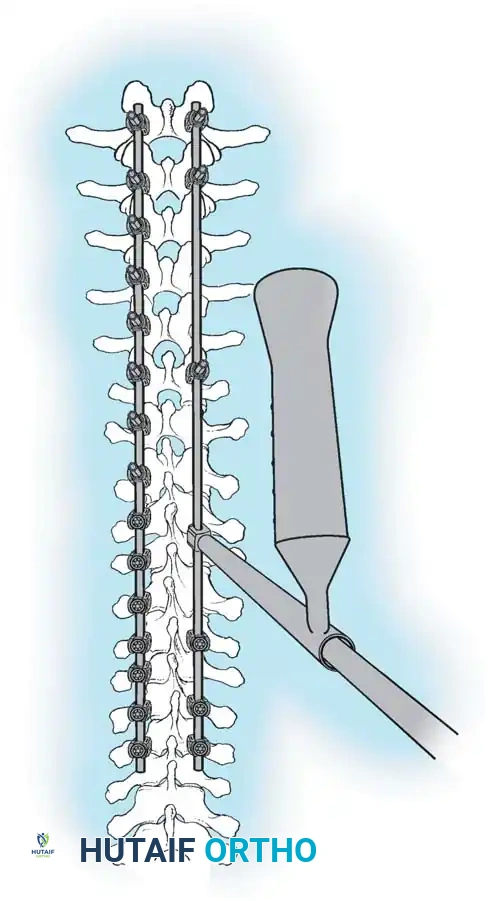
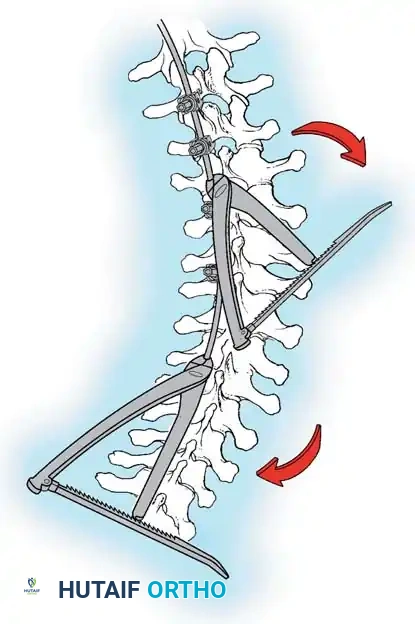
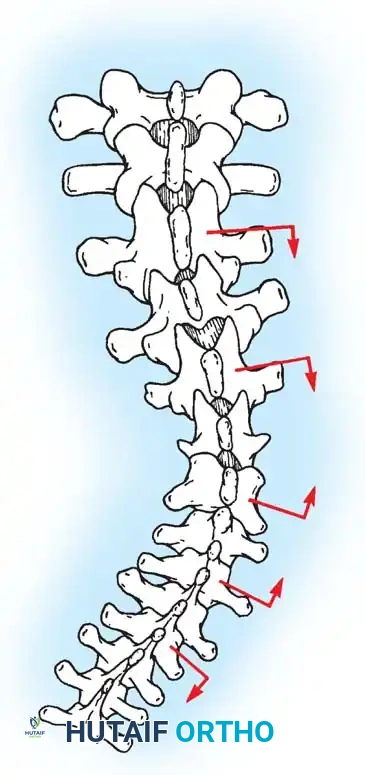
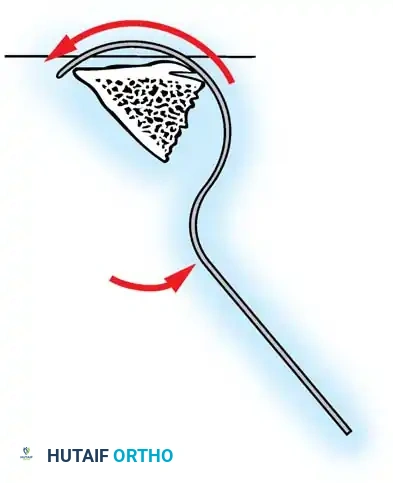
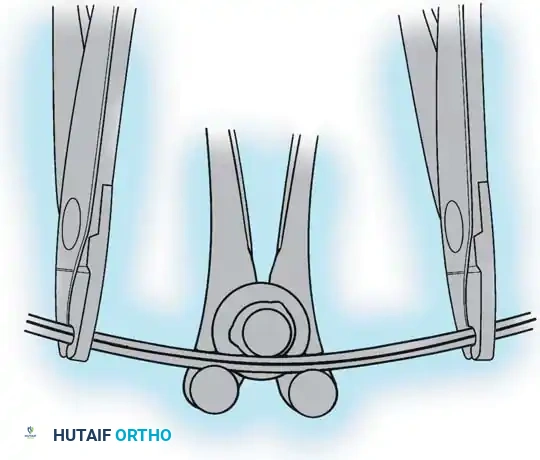
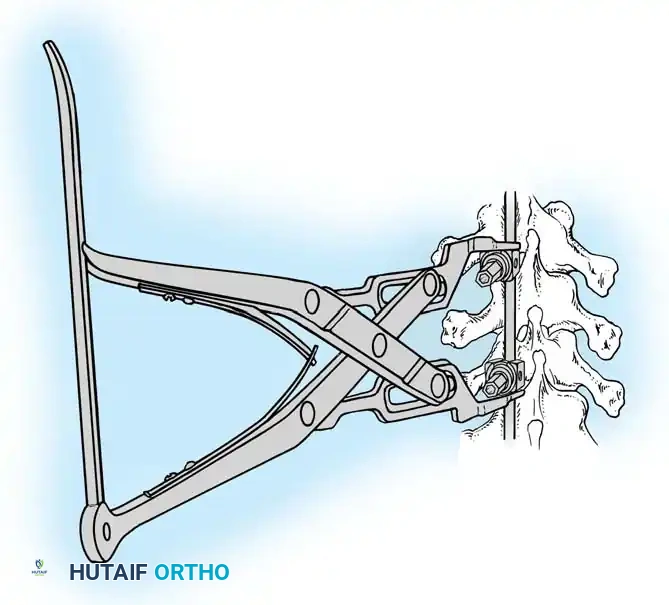
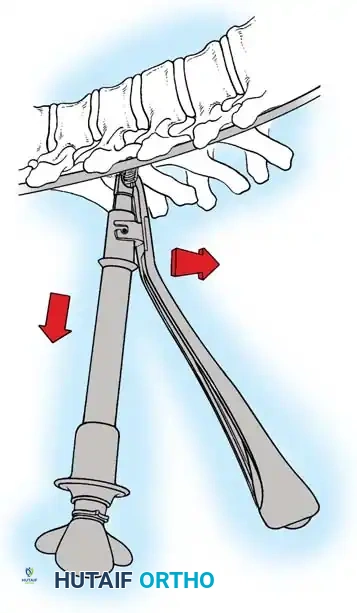
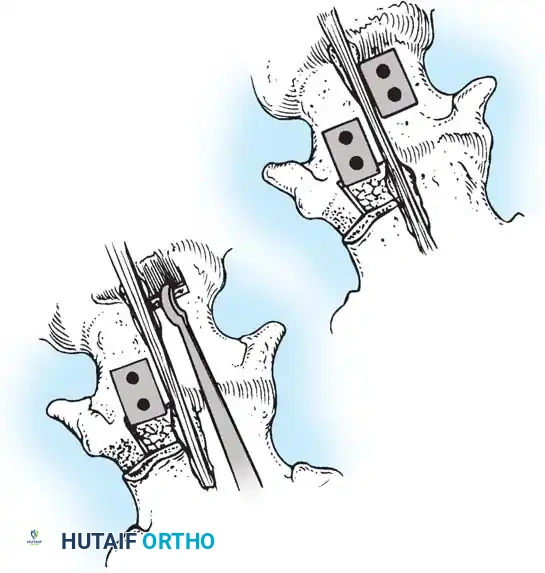
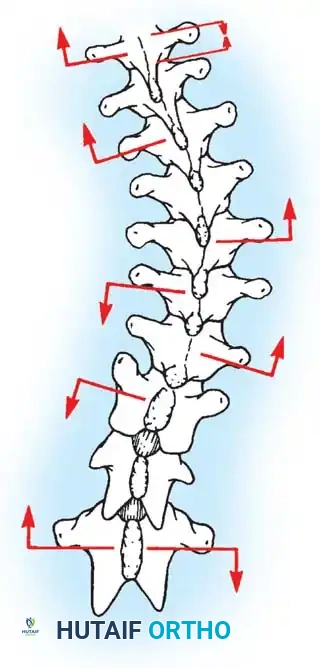
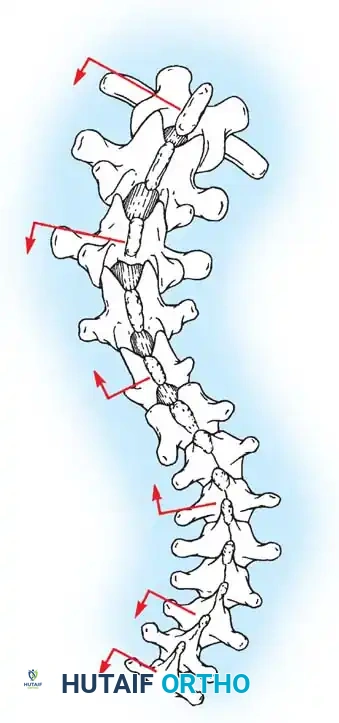
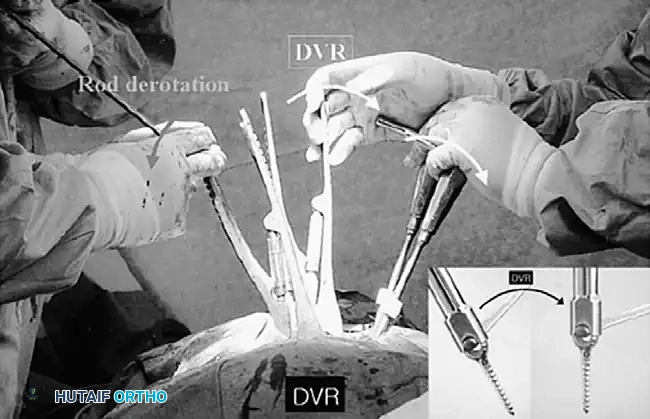
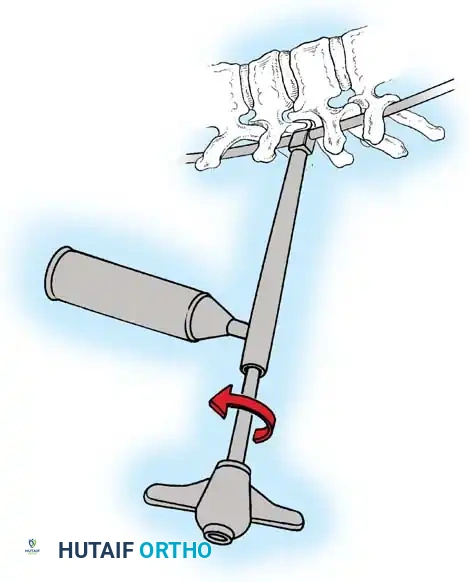
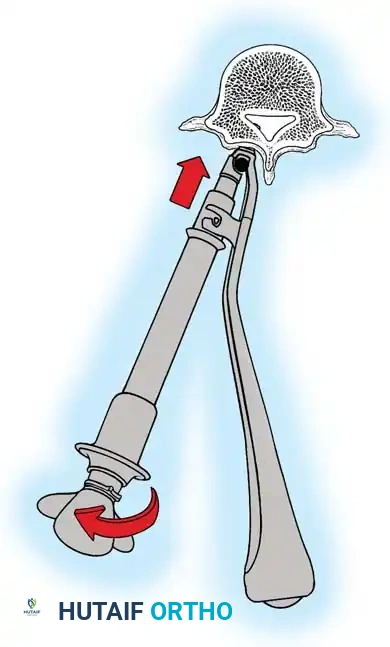
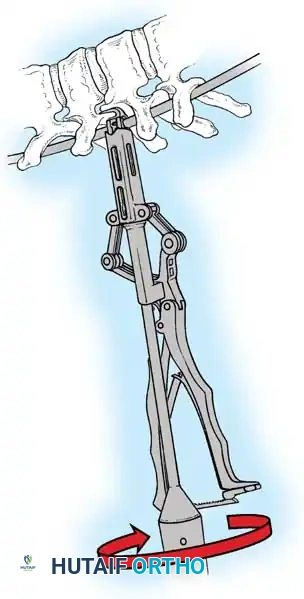
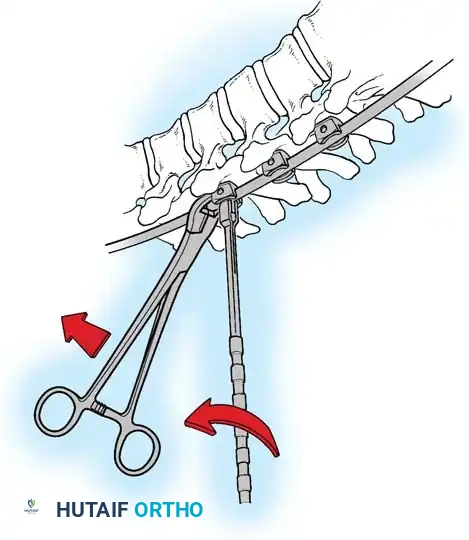
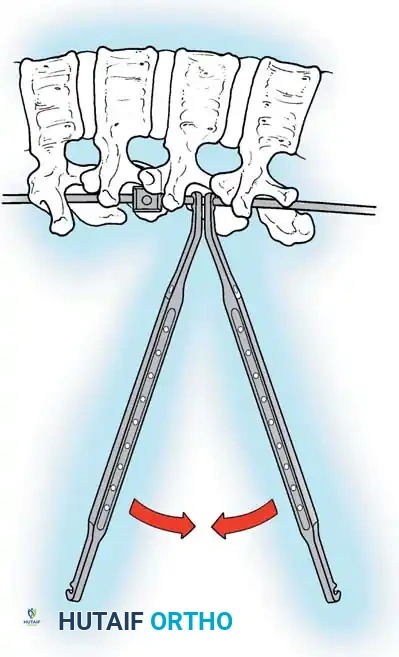
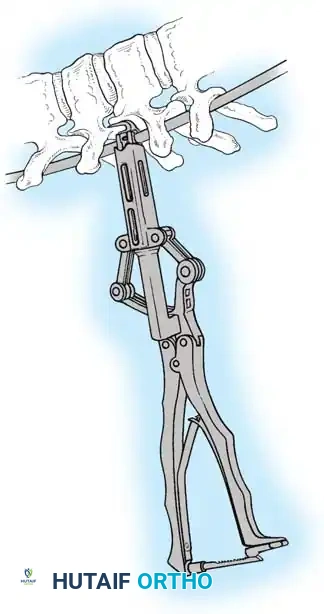
Once the foundation of pedicle screws is established, deformity correction is executed. Modern techniques utilize a combination of rod derotation, direct vertebral translation, and segmental compression/distraction. A pre-contoured rod (often cobalt-chrome for its high yield strength and ability to maintain sagittal contour) is seated into the concave screw heads. As the rod is seated, the spine is translated to the rod. Subsequently, global rod derotation maneuvers are performed to convert coronal deformity into sagittal kyphosis, effectively addressing the 3D nature of AIS. Direct apical vertebral derotation (DVR) using specialized reduction tubes provides powerful axial correction, significantly improving the clinical rib hump.
Decortication and Bone Grafting
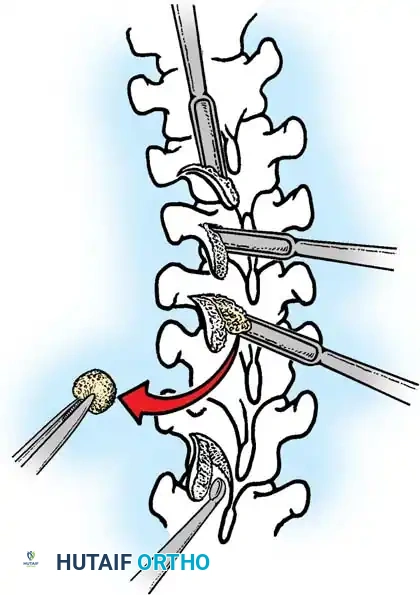
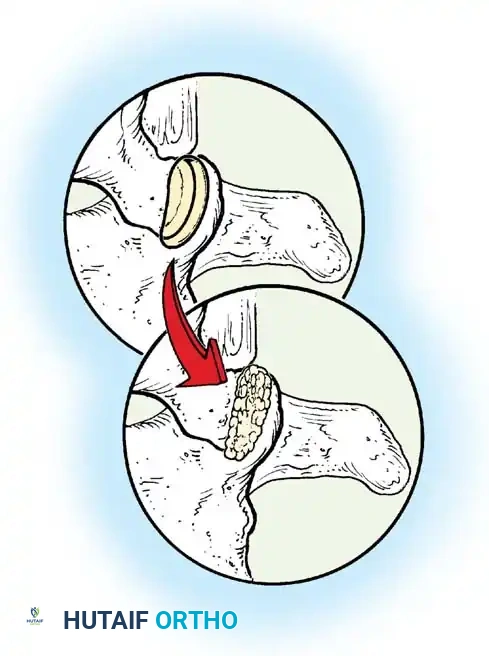
Following final tightening of all set screws, the crucial step of biological preparation begins. The entire exposed posterior elements—laminae, transverse processes, and facet joints—are aggressively decorticated using high-speed burrs or sharp gouges until bleeding cancellous bone is exposed. Local autograft harvested from the spinous processes and facetectomies is milled and mixed with allograft (cancellous chips or demineralized bone matrix) to create a voluminous graft mass. This graft is packed tightly across the decorticated surfaces, particularly on the concave side of the curve, which is under compressive forces conducive to osteogenesis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, posterior spinal fusion for AIS carries inherent risks. Neurological injury is the most devastating complication, occurring in approximately 0.1% to 0.5% of cases. To mitigate this, continuous intraoperative neurophysiological monitoring (IONM), including Somatosensory Evoked Potentials (SSEPs) and Transcranial Motor Evoked Potentials (TcMEPs), is mandatory. A significant loss of MEP signals during correction maneuvers demands immediate action: increasing mean arterial pressure, ensuring adequate oxygenation, removing correction forces (releasing the rod), and checking for misplaced hardware. If signals do not return, a wake-up test may be necessary, and the hardware may need to be permanently removed or adjusted.
Vascular injuries, while rare, can be life-threatening. Lateral pedicle breaches on the left thoracic spine risk injury to the aorta. Massive intraoperative hemorrhage is typically managed proactively with the use of intravenous Tranexamic Acid (TXA), meticulous bipolar electrocautery, and intraoperative cell salvage systems. Postoperative complications include surgical site infections (SSI), which occur in 1% to 2% of idiopathic cases. Deep SSIs require aggressive operative debridement, copious irrigation, and prolonged culture-directed intravenous antibiotics. Hardware is generally retained unless the infection cannot be cleared or the fusion mass is already completely solid.
Long-term mechanical complications include pseudarthrosis, hardware failure, and Proximal Junctional Kyphosis (PJK). Pseudarthrosis presents as loss of correction, pain, and eventual rod fracture, necessitating revision surgery with robust bone grafting and potentially anterior column support. PJK, defined as abnormal kyphosis at the upper instrumented segment, is a growing concern, particularly as constructs become stiffer. Prevention involves meticulous preservation of the supraspinous ligaments at the UIV, avoiding excessive soft tissue dissection cephalad to the fusion, and utilizing transition rods or tethers to gradually dissipate mechanical forces.
| Complication | Estimated Incidence | Prevention & Salvage Management Strategy |
|---|---|---|
| Spinal Cord Injury | 0.1% - 0.5% | Prevention: Continuous SSEP/TcMEP monitoring, meticulous freehand technique. Salvage: Immediate removal of corrective forces, MAP > 85 mmHg, hardware extraction, wake-up test. |
| Surgical Site Infection | 1.0% - 2.0% | Prevention: Pre-op chlorhexidine, IV cefazolin, copious irrigation, intrawound vancomycin powder. Salvage: Urgent operative I&D, retain hardware if not loose, 6 weeks IV antibiotics. |
| Pseudarthrosis / Rod Breakage | 1.0% - 3.0% | Prevention: Aggressive facetectomies, thorough decortication, adequate graft volume, smoking cessation. Salvage: Revision posterior fusion, hardware exchange, massive autograft/BMP application, consider anterior support. |
| Proximal Junctional Kyphosis | 5.0% - 15.0% | Prevention: Preserve UIV supraspinous ligament, avoid over-correction of thoracic kyphosis, use transition rods. Salvage: If symptomatic or progressive, revision extension of fusion proximally. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management of AIS patients has undergone a paradigm shift over the last decade, transitioning from prolonged bed rest and rigid bracing to Enhanced Recovery After Surgery (ERAS) protocols. The immediate postoperative phase (Days 0-3) focuses on aggressive multimodal pain management, early mobilization, and return of bowel function. A combination of gabapentin, acetaminophen, muscle relaxants (e.g., methocarbamol or diazepam), and judicious use of short-acting opioids has largely replaced continuous PCA (Patient-Controlled Analgesia) pumps. Patients are typically mobilized out of bed with physical therapy on postoperative day 1, and Foley catheters are removed within 24 hours to prevent urinary tract infections and encourage ambulation.
During the intermediate phase (Weeks 2-6), the primary focus is on wound healing and biological incorporation of the bone graft. Because modern high-density pedicle screw constructs provide immense immediate biomechanical stability, postoperative bracing (TLSO) is virtually obsolete in the treatment of idiopathic scoliosis, reserved only for patients with poor bone quality or syndromic conditions. Patients are instructed to avoid the "BLTs" (Bending, Lifting > 10 lbs, and Twisting). Return to school is highly variable but generally achieved within 3 to 4 weeks, depending on the patient's stamina and analgesic requirements.

The late rehabilitation phase (Months 3-12) involves serial radiographic monitoring to assess the progression of the fusion mass and maintenance of correction. At 3 months, low-impact aerobic activities (swimming, stationary cycling) are initiated. By 6 months, assuming radiographic evidence of trabecular bridging and absence of pain, patients are cleared for most non-contact sports. Full clearance for high-impact and contact sports is typically granted at 1 year postoperatively, once the arthrodesis is deemed fully mature. Hardware removal is rarely indicated unless the patient develops late-onset operative site pain directly attributable to prominent hardware in asthenic individuals, and is never performed before 2 years post-op to ensure absolute biological union.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of AIS is deeply rooted in a rich history of landmark orthopaedic literature that has continuously refined our techniques and clinical guidelines. The modern era of scoliosis surgery was birthed by Paul Harrington in the 1960s, who introduced the concept of posterior distraction instrumentation. While revolutionary, Harrington rods frequently resulted in flatback syndrome due to their inability to control the sagittal plane. This limitation was addressed by Cotrel and Dubousset in the 1980s, who introduced segmental hook fixation and the concept of three-dimensional rod derotation, fundamentally changing the spatial understanding of the deformity.
The most significant paradigm shift in recent decades was spearheaded by Suk et al. in the mid-1990s, who popularized the use of thoracic pedicle screws. Suk's landmark papers demonstrated that all-pedicle screw constructs provided superior deformity correction, lower pseudarthrosis rates, and shorter fusion lengths compared to hook or hybrid constructs. This was further validated by multi-center prospective studies, notably by Betz, Lenke, and the Harms Study Group, which definitively established pedicle screws as the gold standard for AIS, despite early concerns regarding the neurological safety of thoracic screw placement.