Posterior Hip Dislocation: Comprehensive Orthopedic Diagnosis & Management
Key Takeaway
Posterior hip dislocation is a high-energy traumatic injury where the femoral head displaces posteriorly from the acetabulum. It's emergent because delayed reduction, beyond 6 hours, significantly increases risks of avascular necrosis (AVN) of the femoral head and sciatic nerve injury. Prompt diagnosis and reduction are paramount to mitigate severe long-term sequelae.
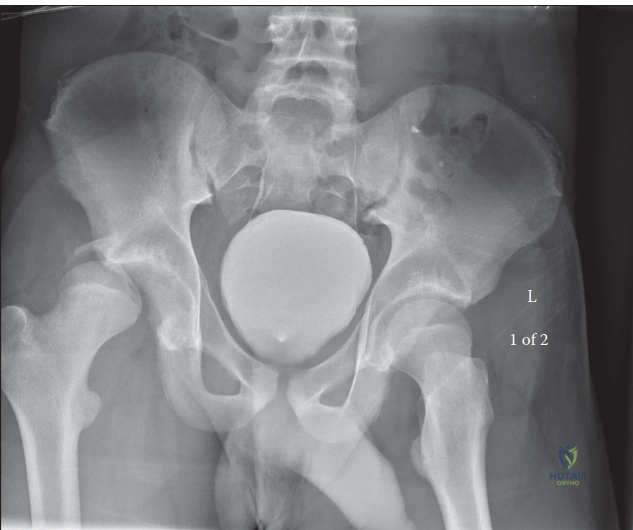
A 28-year-old male presents to the Emergency Department following a high-speed motorcycle collision. He is hemodynamically stable. On clinical examination, his right hip is held in flexion, adduction, and internal rotation. AP Pelvis radiograph is shown below. What are your immediate management priorities?
Candidate: I would perform an ATLS primary survey to rule out other life-threatening injuries. Then, I would conduct a thorough neurovascular assessment, specifically checking for a sciatic nerve palsy. I would order an urgent hip radiograph and then proceed to closed reduction under sedation, ideally within 6 hours. Post-reduction, I would obtain a CT scan to check for concentricity and any incarcerated fragments.
Failure to explicitly mention the absolute contraindication of a femoral neck fracture. Candidates often jump to "reduction" without emphasizing that they have reviewed the radiographs to rule out a concurrent femoral neck fracture, which would necessitate open reduction rather than closed manipulation.
Structure your answer: 1. Resuscitation: ATLS protocol. 2. Assessment: Documented pre-reduction neurovascular status (sciatic nerve is priority). 3. Exclusion: Rule out ipsilateral femoral neck fracture on high-quality imaging (X-ray/CT) as this is a contraindication to closed reduction. 4. Urgency: Aim for reduction <6 hours to minimize AVN risk. 5. Post-procedure: Mandatory CT scan to confirm concentric reduction and evaluate for osteochondral fragments or posterior wall fractures.
You have successfully performed a closed reduction. The patient is now pain-free. How do you assess the stability of the hip, and in what clinical scenario would you opt for an open reduction instead?
Candidate: I assess stability by checking range of motion, specifically looking for re-dislocation during abduction or internal rotation. If the hip is unstable, I would consider surgery. Open reduction is indicated if the reduction is not concentric, if there are incarcerated fragments, or if there is a significant posterior wall fracture.
Failing to mention the Pipkin classification for femoral head fractures or failing to define what "non-concentric" means on a CT scan (e.g., widened joint space, intra-articular debris).
Categorize the indications for ORIF: 1. Irreducibility: Mechanical block (capsule, labrum, or bone). 2. Incongruity: Post-reduction CT showing incarcerated fragments or subluxation. 3. Fracture management: Unstable posterior acetabular wall fractures or significant Pipkin Type II-IV femoral head fractures. 4. Neurological: Progressive sciatic nerve deficit suggestive of entrapment. 5. Technique: Use the Kocher-Langenbeck approach, protecting the sciatic nerve and repairing the capsule/short rotators at closure.
