Pediatrics 2004 Practice Questions: Set 1 (Solved)

Key Takeaway
Your ultimate guide to Pediatrics 2004 Practice Questions: Set 1 (Solved) starts here. Access high-yield Pediatrics questions for the 2004 board exam. This module (Set 1) covers critical topics including surgical techniques, pathology, and treatment protocols with verified answers.
Pediatrics 2004 Practice Questions: Set 1 (Solved)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
An 8-year-old boy sustains nondisplaced midshaft fractures of the tibia and fibula after being struck by a car while he was riding his bicycle. No other injuries are noted, but the patient reports pain with passive motion of his toes. His neurovascular examination is otherwise normal. What is the best course of action?

Explanation
Question 2
A 6-year-old girl has the bilateral foot deformity shown in Figure 1. There is no family history of disease. Examination reveals fixed hindfoot equinus, and muscle function testing shows strong posterior tibial function, fair plus anterior tibial function, poor peroneal function, and strong gastrocnemius function. A Coleman block test shows a correctable hindfoot. Nerve conduction velocity studies show diminished function in the peroneal and ulnar nerves on both sides. Pathologic changes found in a sural nerve biopsy include "onion bulb" formation, and DNA testing confirms the presence of a mutation in the MPZ gene, consistent with hereditary motor sensory neuropathy type III (HMSN-III). What is the best course of action?

Explanation
Question 3
An obese 4-year-old boy has infantile Blount's disease. Radiographs reveal a metaphyseal-diaphyseal angle of 18 degrees and a depression of the medial proximal tibial physis. Management should consist of

Explanation
Question 4
A 10-year-old boy has activity-related knee pain that is poorly localized. He denies locking, swelling, or giving way. Examination shows mild tenderness at the medial femoral condyle and painless full range of motion without ligamentous instability. Radiographs are shown in Figures 2a through 2c. What is the best course of action?

Explanation
Question 5
Figure 3a shows the preoperative radiograph of a 5-year-old girl who achieved complete correction with valgus osteotomies. Figure 3b shows a radiograph obtained 2 years later. What is the cause of the recurrent deformity on the right side?

Explanation
Question 6
An 8-year-old boy reports ankle pain after striking the ground with the medial aspect of his foot while attempting to kick a soccer ball. Radiographs reveal slight distal tibial physeal widening but no other abnormalities. In treating this injury, which of the following associated conditions is most likely present but may be missed without careful evaluation?

Explanation
Question 7
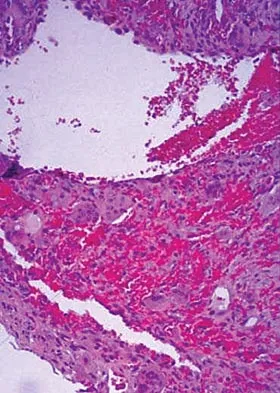
An 11-year-old girl has wrist pain. Figure 4a shows the radiograph, and Figures 4b and 4c show the low- and medium-power photomicrographs of a lesion in the distal radius. What is the most likely diagnosis?
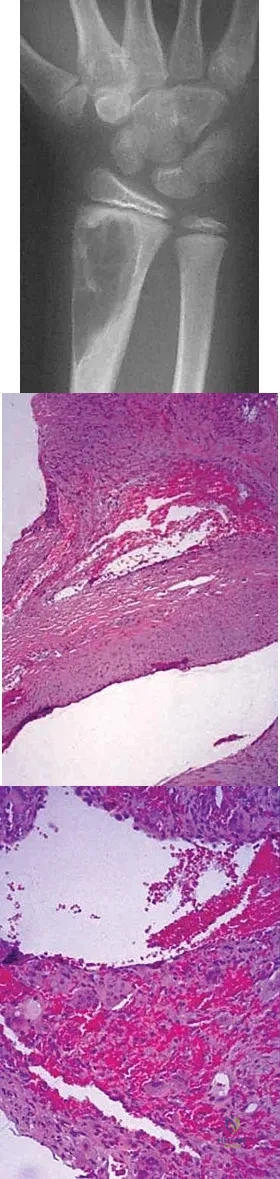
Explanation
Question 8
In a patient with vertebral tuberculosis, which of the following characteristics is most predictive of progression of the kyphosis?

Explanation
Question 9
When planning scoliosis surgery for a patient with a 50-degree thoracolumbar curve and spinal muscular atrophy, it is most important to include

Explanation
Question 10
An 8-year-old boy sustains injuries to his head, abdomen, and left lower extremity after being struck by a truck. In the emergency department, his mental status deteriorates and he is intubated after assessment reveals a Glasgow Coma Scale score of 3; the score subsequently improves to 10. A CT scan reveals a right parietal intracranial hemorrhage, and an abdominal ultrasound reveals free fluid. Prior to an emergency laparotomy, the swollen left thigh is evaluated. Radiographs reveal a transverse fracture of the mid-diaphysis. Management of the fracture should consist of

Explanation
Question 11
A 3-year-old boy has a rigid 40-degree lumbar scoliosis that is the result of a fully segmented L5 hemivertebra. All other examination findings are normal. Management should consist of

Explanation
Question 12
A newborn with bilateral talipes equinovarus undergoes serial manipulation and casting. What is the primary goal of manipulation?

Explanation
Question 13
Figure 5 shows the radiograph of a 10-year-old girl who reports chronic shoulder pain after her gymnastics classes. Examination reveals pain on internal and external rotation but no instability. What is the most likely diagnosis?

Explanation
Question 14
Figure 6 shows the clinical photographs of a newborn who underwent a colostomy for an imperforate anus. Examination shows extended knees, flexed hips, and equinovarus feet. Dimpling is noted over the buttocks. Patients with these findings differ from patients with myelodysplasia in that they

Explanation
Question 15
Which of the following patients is considered the most appropriate candidate for selective dorsal rhizotomy?

Explanation
Question 16
A 2-day-old infant has the hyperextended knee deformity shown in Figure 7. No other deformities are found on examination. A radiograph shows that the ossified portion of the proximal tibia is slightly anterior to that of the distal femur. Management should consist of

Explanation
Question 17
Figures 8a and 8b show the current radiographs of a 10-year-old boy with a hip disorder who was treated with an abduction orthosis 3 years ago. If no further remodeling occurs, what is the most likely prognosis?

Explanation
Question 18
In girls with idiopathic scoliosis, peak height velocity (PHV) typically occurs at what point?

Explanation
Question 19
Examination of a 6-year-old boy who sustained a displaced Salter-Harris type II fracture of the distal radius reveals 35 degrees of volar angulation. A satisfactory reduction is obtained with the aid of a hematoma block. At the 10-day follow-up examination, radiographs show loss of reduction and 35 degrees of volar angulation. Management should now consist of

Explanation
Question 20
Figures 9a and 9b show the radiographs of a 12-year-old girl who has had right hip pain for the past 4 months. She reports that the pain is so severe that she is unable to walk and is now using a wheelchair. Examination reveals pain with any attempted range of motion. Management should include
Explanation
Question 21
An 18-month-old boy has 45 degrees of kyphosis in the thoracolumbar spine secondary to type I congenital kyphosis. Examination reveals that he is neurologically intact, and an MRI scan shows no evidence of intraspinal pathology. Management should consist of

Explanation
Question 22
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Explanation
Question 23
Which of the following findings can cause a dorsal bunion in a patient with neuromuscular disease?

Explanation
Question 24
Which of the following studies is considered most sensitive in monitoring a therapeutic response in acute hematogenous osteomyelitis?

Explanation
Question 25
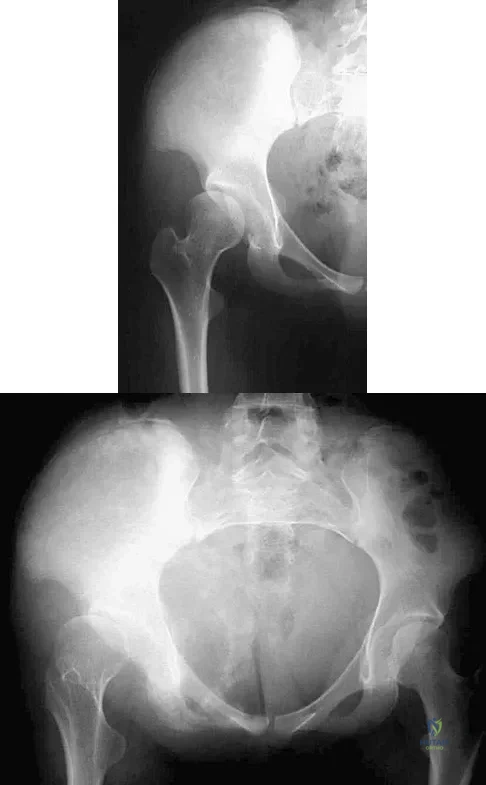
Figure 10 shows the radiograph of a 7-year-old patient who has a bilateral Trendelenburg limp and limited range of hip motion but no pain. His work-up should include

Explanation
Question 26
A 3-month-old girl with Developmental Dysplasia of the Hip (DDH) is treated with a Pavlik harness. At her two-week follow-up, the mother reports that the infant is no longer kicking her right leg as much. On examination, the infant demonstrates decreased active knee extension on the right side. What is the most likely cause of this finding?
Explanation
Question 27
A 7-year-old boy with spastic quadriplegic cerebral palsy has progressive lateral subluxation of the right hip. Radiographs reveal a migration percentage of 50%, a neck-shaft angle of 155 degrees, and an acetabular index of 35 degrees. What is the most appropriate definitive management?
Explanation
Question 28
A 13-year-old obese boy undergoes in situ single screw fixation for a stable mild slipped capital femoral epiphysis (SCFE) of the left hip. Nine months later, he returns complaining of progressive left hip pain, severe stiffness, and an inability to participate in sports. Radiographs reveal diffuse joint space narrowing of the left hip and subchondral irregularities, with the screw threads completely within the femoral head. What is the most likely diagnosis?
Explanation
Question 29
A 5-year-old boy presents with a lateral condyle fracture of the distal humerus that was treated with a long-arm cast at an outside facility 4 weeks ago. Radiographs now demonstrate 4 mm of displacement of the fracture fragment and no evidence of callus formation. What is the most appropriate next step in management?
Explanation
Question 30
A 12-year-old premenarcheal girl presents for evaluation of a spinal deformity. She is Risser 0. Standing posteroanterior and lateral radiographs of the spine reveal a right thoracic curve of 36 degrees and normal sagittal alignment. Which of the following is the most appropriate treatment recommendation?
Explanation
Question 31
A 4-week-old infant is undergoing treatment for an idiopathic right clubfoot using the Ponseti method. After four sequential casts, the forefoot is abducted to 60 degrees, and the heel is in valgus. However, the ankle can only be dorsiflexed to neutral. What is the most appropriate next step in management?
Explanation
Question 32
A 6-year-old boy sustains a supracondylar fracture of the humerus. Radiographs demonstrate a Gartland Type III fracture with posteromedial displacement of the distal fragment. Which of the following neurologic deficits is most likely to be present?
Explanation
Question 33
A 4-year-old boy with blue sclerae and a history of four extremity fractures after minimal trauma is diagnosed with severe Osteogenesis Imperfecta (OI). Which of the following pharmacological therapies is currently the standard of care to decrease fracture incidence and increase bone mineral density in this patient?
Explanation
Question 34
An 11-year-old boy presents with a 6-month history of bilateral foot pain and recurrent ankle sprains. Examination reveals rigid flatfeet with absent subtalar motion and peroneal spasticity. Computed tomography (CT) confirms bilateral talocalcaneal coalitions involving approximately 25% of the posterior facet, with no degenerative changes. Nonoperative management with casting and orthotics has failed to relieve his symptoms. What is the most appropriate surgical intervention?
Explanation
Question 35
A 13-year-old boy presents to the emergency department with severe left hip pain after tripping over a curb. He is completely unable to bear weight on the left leg, even with the assistance of crutches. Radiographs demonstrate a severe slipped capital femoral epiphysis (SCFE). Which of the following factors is the most significant predictor for the development of avascular necrosis in this patient?
Explanation
Question 36
A 13-year-old boy weighing 95 kg presents with left groin pain and an obligatory external rotation of the hip with flexion. Radiographs confirm a left slipped capital femoral epiphysis (SCFE). Which of the following factors is the strongest indication for prophylactic in situ pinning of the contralateral asymptomatic hip?
Explanation
Question 37
A 4-month-old infant is being treated with a Pavlik harness for developmental dysplasia of the hip (DDH). During a routine follow-up, the parents report that the child has stopped kicking the affected leg. On examination, there is decreased active extension of the knee, but the child moves the foot and toes spontaneously. What is the most likely cause, and what is the appropriate initial management?
Explanation
Question 38
A 6-year-old boy sustains a completely displaced, extension-type supracondylar fracture of the humerus. During the neurologic examination, he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. Which nerve is most likely injured?
Explanation
Question 39
An 8-year-old boy with spastic quadriplegic cerebral palsy is found to have a migration percentage of 45% on his anteroposterior pelvis radiograph. He has pain with diaper changes and limited hip abduction. What is the most appropriate management?
Explanation
Question 40
A 9-year-old boy presents with a painless limp and restricted hip internal rotation. Radiographs demonstrate fragmentation of the capital femoral epiphysis consistent with Legg-Calvé-Perthes disease. Which of the following factors carries the worst prognosis for this patient?
Explanation
Question 41
When treating a rigid idiopathic clubfoot using the Ponseti method of serial casting, what is the correct order of deformity correction?
Explanation
Question 42
A 10-year-old boy presents to the emergency department after sustaining a minor twisting injury to his right arm while throwing a baseball. Radiographs reveal a minimally displaced pathologic fracture through a centrally located, completely radiolucent lesion in the proximal humerus metaphysis. The lesion demonstrates a 'fallen leaf' sign. What is the most appropriate initial management?
Explanation
Question 43
A 3-year-old girl is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. Before proceeding with any surgical intervention, which of the following screening evaluations is most critical to perform?
Explanation
Question 44
A 4-year-old boy sustains a minimally displaced (<2 mm) lateral condyle fracture of the humerus that is treated in a long-arm cast. He is lost to follow-up and returns 15 years later. Radiographs demonstrate an established nonunion of the lateral condyle. Which of the following clinical findings is most likely to be present on physical examination?
Explanation
Question 45
An 11-year-old girl falls off her bicycle and injures her left knee. Radiographs reveal a Type III tibial eminence fracture (completely displaced). This injury is considered the pediatric equivalent of which of the following adult sports injuries?
Explanation
Question 46
A 4-month-old infant presents with a persistently dislocated left hip after a failed 6-week trial of Pavlik harness treatment. Ultrasound confirms the femoral head is dislocated but reducible with moderate force. The acetabulum appears dysplastic. What is the most appropriate next step in management?
Explanation
Question 47
A 12-year-old obese boy presents with acute on chronic left knee pain and an antalgic gait. Physical examination reveals obligate external rotation of the thigh during passive hip flexion. He is diagnosed with a stable slipped capital femoral epiphysis (SCFE) and undergoes in situ pinning with a single cannulated screw. Which of the following is the most significant risk factor for the development of chondrolysis in this patient?
Explanation
Question 48
A 6-year-old girl sustains a severely displaced extension-type supracondylar fracture of the humerus. On examination, the hand is pink but the radial pulse is absent. Neurologic examination reveals an inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured?
Explanation
Question 49
A 13-year-old boy presents with a painful, rigid flatfoot and a history of recurrent ankle sprains. Examination shows a lack of subtalar motion and peroneal muscle spasm. Radiographs show a continuous C-shaped radiodense line formed by the medial outline of the talar dome and the posteroinferior aspect of the sustentaculum tali. Which of the following is the most likely diagnosis?
Explanation
Question 50
An 8-year-old boy presents with a painless limp. Radiographs demonstrate fragmentation of the capital femoral epiphysis. The treating orthopedic surgeon notes multiple 'head-at-risk' signs on the radiograph. According to Catterall, which of the following is considered a 'head-at-risk' sign in Legg-Calve-Perthes disease?
Explanation
Question 51
A 6-year-old nonambulatory child with spastic quadriplegic cerebral palsy presents for routine evaluation. An anteroposterior pelvis radiograph demonstrates a right hip migration percentage of 55%. The child is currently asymptomatic. What is the most appropriate management?
Explanation
Question 52
A 14-year-old boy sustains a Salter-Harris type II fracture of the distal femur during a football game. He undergoes an anatomic closed reduction and casting. Which of the following complications is most commonly associated with this specific injury?
Explanation
Question 53
A 2-year-old boy presents with an anterolateral bowing of the tibia and a pseudoarthrosis. Physical examination reveals multiple café-au-lait spots on his trunk and axillary freckling. Which of the following conditions is most strongly associated with this orthopedic presentation?
Explanation
Question 54
During the Ponseti casting technique for the treatment of idiopathic clubfoot, the foot is sequentially manipulated to correct the complex deformity. Which of the following describes the correct sequential order of deformity correction?
Explanation
Question 55
A 14-year-old female gymnast presents with progressive low back pain. Radiographs demonstrate a grade II isthmic spondylolisthesis at L5-S1. She has failed 6 months of conservative management (rest, bracing, physical therapy), and her pain significantly limits her activities of daily living. Neurologic examination is entirely normal. What is the most appropriate surgical treatment?
Explanation
Question 56
A 3-year-old boy presents to the emergency department after falling off a slide. He has a closed, isolated midshaft femur fracture with 1.5 cm of shortening. He is normally developing and has no other injuries. What is the most appropriate definitive management for this patient?
Explanation
Question 57
A 7-year-old girl with spastic quadriplegic cerebral palsy presents for routine surveillance. She is non-ambulatory (GMFCS Level V). Radiographs of the pelvis demonstrate a right hip migration percentage of 55%, coxa valga, and an intact Shenton's line on the left. She has mild pain with hip abduction. What is the most appropriate management?
Explanation
Question 58
A 9-month-old girl presents for an initial orthopedic evaluation. She has asymmetric thigh folds and limited abduction of the left hip. Ultrasound at 6 weeks of age was reportedly abnormal but the parents did not follow up. Current radiographs demonstrate a dislocated left hip with a dysplastic acetabulum. What is the most appropriate next step in management?
Explanation
Question 59
A 13-year-old girl sustains a twisting injury to her right ankle. Radiographs reveal a Salter-Harris III fracture of the anterolateral distal tibia.
This specific fracture pattern (Juvenile Tillaux fracture) occurs as a direct result of the asymmetrical closure of the distal tibial physis. Which of the following describes the LAST portion of the distal tibial physis to close?

Explanation
Question 60
A 6-year-old boy falls onto an outstretched hand and sustains a widely displaced, extension-type supracondylar fracture of the humerus. On physical examination in the emergency department, his hand is pink and well-perfused with a palpable radial pulse. However, he is unable to flex the interphalangeal joint of his thumb and the distal interphalangeal joint of his index finger. Which nerve is most likely injured?
Explanation
Question 61
An 11-year-old boy with a BMI in the 99th percentile presents with left knee pain and a limp for 4 weeks. Radiographs show a mild, stable slipped capital femoral epiphysis (SCFE) of the left hip. The parents ask about the risk to the other hip. Which of the following is the strongest indication for prophylactic pinning of the contralateral, asymptomatic right hip?
Explanation
Question 62
An 8-year-old boy presents with a 2-month history of a painless limp. Radiographs demonstrate sclerosis and fragmentation of the proximal femoral epiphysis consistent with Legg-Calve-Perthes disease. Which of the following is considered the most important radiographic prognostic factor for determining the final outcome of the hip?
Explanation
Question 63
A 14-year-old boy complains of recurrent right ankle sprains and deep midfoot pain that worsens with activity. Examination reveals a rigid flat foot, prominent peroneal tendons, and limited subtalar inversion and eversion. Lateral radiographs show an elongated anterior process of the calcaneus (the 'anteater nose' sign). What is the most likely diagnosis?
Explanation
Question 64
A 12-year-old girl presents with a destructive diaphyseal lesion of the femur with a permeative pattern and an 'onion skin' periosteal reaction.
A core needle biopsy is performed, revealing sheets of uniform small, round, blue cells. Immunohistochemistry is strongly positive for CD99. Which of the following chromosomal translocations is most characteristic of this tumor?
Explanation
Question 65
A newborn male is evaluated for bilateral idiopathic clubfeet (talipes equinovarus). The treating orthopedic surgeon initiates the Ponseti method of serial casting. What is the correct physiological sequence in which the components of the deformity are systematically corrected?
Explanation
Question 66
A 12-year-old boy with a BMI of 35 presents with an acute on chronic slipped capital femoral epiphysis (SCFE) of the left hip. He undergoes uneventful in situ pinning. When considering prophylactic pinning of the contralateral right hip, which of the following is the most important risk factor for developing a subsequent SCFE?
Explanation
Question 67
A 6-year-old boy presents with a completely displaced posteromedial supracondylar humerus fracture. Based on the direction of displacement, which nerve is at highest risk of injury?
Explanation
Question 68
An infant is placed in a Pavlik harness for treatment of developmental dysplasia of the hip (DDH). During a follow-up visit, the parents report that the child has stopped kicking the leg. Examination reveals an absence of active knee extension on the affected side, but intact ankle dorsiflexion and plantar flexion. What is the most appropriate next step in management?
Explanation
Question 69
When treating idiopathic clubfoot using the Ponseti method, what is the proper sequence of deformity correction?
Explanation
Question 70
Which of the following is the most important prognostic factor for long-term outcome in a child with Legg-Calvé-Perthes disease?
Explanation
Question 71
A 14-year-old boy presents with knee pain. Radiographs reveal a mixed sclerotic and lytic lesion in the distal femoral metaphysis with a sunburst periosteal reaction and a Codman triangle. A biopsy shows malignant spindle cells producing osteoid. What is the most significant prognostic factor for survival in this patient?
Explanation
Question 72
A 5-year-old child with spastic quadriplegic cerebral palsy is evaluated in the clinic. The patient has a Gross Motor Function Classification System (GMFCS) level of V. What is the most appropriate radiographic screening protocol for hip displacement in this patient?
Explanation
Question 73
A 12-year-old boy presents with a history of recurrent ankle sprains and rigid flatfeet. On examination, he has decreased subtalar motion and peroneal spasticity. Radiographs demonstrate a C-sign on the lateral view of the foot. Which of the following is the most appropriate initial management?
Explanation
Question 74
A 3-year-old child sustains a closed, isolated midshaft femur fracture with 2 cm of shortening after falling from a playground slide. Which of the following is the most appropriate definitive management?
Explanation
Question 75
A 14-year-old female gymnast complains of lower back pain that worsens with extension activities. Neurological exam is normal. AP and lateral radiographs of the lumbar spine are normal. What is the most appropriate next step in imaging to diagnose an acute pars interarticularis stress reaction?
Explanation
Question 76
An 11-year-old girl with a history of renal osteodystrophy presents with a 3-week history of left groin and knee pain. She is diagnosed with a moderate slipped capital femoral epiphysis (SCFE) on the left side. Her right hip is completely asymptomatic, and radiographs of the right hip are normal. What is the most appropriate management regarding the contralateral right hip?
Explanation
Question 77
A 6-year-old boy falls from the monkey bars and sustains a displaced extension-type supracondylar humerus fracture. Radiographs demonstrate posterolateral displacement of the distal fragment.
Based on the direction of displacement, which nerve is most at risk for injury, and what is its characteristic motor deficit?
Explanation
Question 78
A 3-month-old infant with developmental dysplasia of the hip is being treated with a Pavlik harness. At a routine 2-week follow-up, the mother reports that the child is no longer kicking her right leg. On examination, there is an absence of active knee extension on the right side, but foot and ankle motion are preserved. What is the most likely cause of this finding?
Explanation
Question 79
A 7-year-old child with spastic quadriplegic cerebral palsy is evaluated for progressive left hip dysplasia. Current anteroposterior pelvis radiographs show a migration percentage of 65%, a neck-shaft angle of 155 degrees, and an intact triradiate cartilage. The articular cartilage appears well-preserved on MRI. What is the most appropriate surgical intervention?
Explanation
Question 80
A 7-year-old boy is diagnosed with Legg-Calvé-Perthes disease. According to the Herring classification system, which of the following radiographic parameters evaluated during the fragmentation stage is the most reliable predictor of long-term outcome?
Explanation
Question 81
When correcting an infant's idiopathic clubfoot deformity using the Ponseti casting technique, the deformities must be sequentially addressed. What is the correct chronological order of correction?
Explanation
Question 82
A 9-year-old boy presents to the emergency department after a minor fall with right arm pain. Radiographs reveal a centrally located, lucent metaphyseal lesion in the proximal humerus with a nondisplaced pathologic fracture. A 'fallen leaf' sign is noted within the lesion.
What is the most appropriate initial management?
Explanation
Question 83
A 5-year-old girl falls onto an outstretched hand and complains of elbow pain. Radiographs demonstrate a lateral condyle fracture of the distal humerus.
The fracture fragment is displaced by 4 millimeters. What is the most appropriate definitive management?
Explanation
Question 84
A 13-year-old boy sustains a twisting injury to his ankle while playing soccer. Radiographs demonstrate a Salter-Harris type III fracture of the anterolateral aspect of the distal tibia (Tillaux fracture).
This specific fracture pattern is governed by the normal physiological closure pattern of the distal tibial physis. In what order does the distal tibial physis close?

Explanation
Question 85
A 4-year-old child with a history of recurrent fractures, blue sclerae, and dentinogenesis imperfecta is diagnosed with osteogenesis imperfecta (OI) type III. In order to decrease the fracture burden and correct progressive long-bone deformities, what is the current gold standard combined medical and surgical management strategy?
Explanation
Question 86
An obese 12-year-old boy presents with acute-on-chronic left thigh pain and is unable to bear weight on the left leg, even with crutches. Radiographs demonstrate a posterior and medial displacement of the proximal femoral epiphysis. According to the Loder classification, what is the most significant complication directly associated with his specific presentation type?
Explanation
Question 87
A 13-year-old boy complains of frequent ankle sprains and lateral foot pain. Examination reveals a rigid flatfoot with peroneal spasticity. Oblique radiographs of the foot demonstrate an 'anteater sign.'
If a 6-month trial of short leg casting and orthotics fails to relieve his symptoms, and no degenerative changes are noted on CT scan, what is the most appropriate definitive surgical management?
Explanation
Question 88
A 6-year-old boy falls from monkey bars and sustains a completely displaced, extension-type supracondylar humerus fracture. On arrival at the emergency department, his hand is pink and warm with brisk capillary refill, but no radial pulse is palpable. What is the next best step in management?
Explanation
Question 89
A 6-year-old child with spastic quadriplegic cerebral palsy is evaluated during routine hip surveillance. Radiographs demonstrate a Reimer's migration percentage of 45% in the right hip. There are no advanced degenerative changes. What is the most appropriate management?
Explanation
Question 90
A 4-month-old infant with developmental dysplasia of the hip (DDH) has been managed with a Pavlik harness for 4 weeks. Repeat dynamic ultrasound demonstrates that the affected hip remains completely dislocated and cannot be reduced in the harness. What is the most appropriate next step in management?
Explanation
Question 91
An 8-year-old boy presents with a painless limp. Radiographs demonstrate fragmentation of the capital femoral epiphysis consistent with Legg-Calvé-Perthes disease.
The lateral pillar maintains 60% of its normal height. According to the prospective multicenter study by Herring et al., what is the most appropriate management for this specific presentation?

Explanation
Question 92
A 2-week-old infant is diagnosed with congenital idiopathic clubfoot and is scheduled to begin serial casting using the Ponseti method. What is the correct chronological sequence of deformity correction in this technique?
Explanation
Question 93
An 8-year-old boy weighing 35 kg sustains a closed, length-stable, transverse midshaft fracture of the femur. His neurovascular examination is intact. What is the most appropriate definitive management?
Explanation
Question 94
A 12-year-old boy sustains a Salter-Harris type II fracture of the distal femur. The fracture is managed with a closed reduction and percutaneous pinning. Post-operative radiographs show perfect anatomical alignment. Despite an optimal reduction, the parents should be thoroughly counseled that the child remains at significant risk for which of the following complications?
Explanation
Question 95
A 3-year-old girl with blue sclerae and dentinogenesis imperfecta presents with her third low-energy long bone fracture. Genetic testing confirms a mutation affecting type I collagen. Which of the following systemic pharmacological treatments is most commonly indicated to decrease fracture incidence and improve bone mass in this condition?
Explanation
Question 96
A 2-week-old infant is brought to the clinic for evaluation of a bilateral congenital foot deformity. Examination reveals rigid equinus, varus of the hindfoot, adductus of the forefoot, and a cavus midfoot. The decision is made to initiate the Ponseti method of serial casting. According to the principles of this technique, what is the correct sequence of deformity correction?
Explanation
Question 97
A 6-year-old boy falls from the monkey bars and sustains a completely displaced, extension-type supracondylar fracture of the humerus. On presentation to the emergency department, his hand is pink and well-perfused. However, neurologic examination reveals that he is unable to flex the interphalangeal joint of his thumb or the distal interphalangeal joint of his index finger. Which of the following nerve structures is most likely injured?
Explanation
Question 98
A 7-month-old girl presents for evaluation of a persistent limp and asymmetric thigh folds. She has had no prior orthopedic treatment. Ultrasound and plain radiographs confirm a completely dislocated left hip consistent with developmental dysplasia of the hip (DDH). Clinical examination demonstrates limited abduction of the left hip and a positive Galeazzi sign. What is the most appropriate initial management for this patient?
Explanation
Question 99
A 12-year-old obese boy with a history of end-stage renal disease presents with a 3-week history of left thigh pain and a noticeable limp. He denies trauma. Examination reveals obligate external rotation of the left hip upon passive flexion. Radiographs demonstrate a mild left slipped capital femoral epiphysis (SCFE). Radiographs of the right hip appear normal. What is the most appropriate definitive management?
Explanation
Question 100
A 5-year-old girl with spastic quadriplegic cerebral palsy is evaluated in the clinic. She is non-ambulatory (GMFCS Level V) and requires full assistance for transfers. Pelvic radiographs reveal an anteroposterior view with a bilateral migration percentage (Reimers' index) of 45%. Clinical examination shows bilateral hip abduction is limited to 20 degrees with the hips in extension. She has an established coxa valga deformity. What is the most appropriate management to prevent painful hip dislocation?
Explanation
None
