Dupuytren Contracture: Pathogenesis, Pathoanatomy, and Surgical Management

Key Takeaway
Dupuytren contracture is a benign fibroproliferative disorder of the palmar fascia characterized by fibroblast proliferation and abnormal type III collagen deposition. This leads to progressive flexion contractures of the metacarpophalangeal and proximal interphalangeal joints. Surgical management, primarily regional fasciectomy, requires meticulous dissection of diseased fascial cords—particularly the spiral cord, which predictably displaces the neurovascular bundle—to restore digital extension and optimize hand function.
INTRODUCTION AND EPIDEMIOLOGY
Dupuytren disease is a progressive, benign fibroproliferative disorder of the palmar fascia. While the exact etiology remains elusive, extensive research has elucidated the cellular and connective tissue alterations that drive the disease process. The condition exhibits an autosomal dominant inheritance pattern with variable penetrance, predominantly affecting individuals of Northern European descent (frequently termed the "Viking disease").
Although Dupuytren disease shares some histological similarities with malignant fibromatoses—such as uncontrolled cellular proliferation—it is strictly a benign process. The clinical hallmark is the development of palmar nodules that progress to palpable cords, ultimately resulting in irreversible flexion contractures of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints.
PATHOGENESIS AND CELLULAR BIOLOGY
The pathogenesis of Dupuytren contracture is fundamentally a disorder of abnormal fibroblast proliferation and dysregulated collagen deposition. The disease process has been closely compared to an exaggerated wound healing response.
The Role of the Myofibroblast
The primary effector cell in Dupuytren disease is the myofibroblast. In normal fascia, type I collagen predominates. However, in Dupuytren tissue, an initial surge in fibroblast proliferation is followed by a massive deposition of type III collagen.
Growth factors and their specific receptors exhibit markedly increased expression in diseased palmar fascia. The most critical mediators include:
* Transforming Growth Factor-Beta (TGF-β): The primary catalyst that induces the differentiation of standard fibroblasts into contractile myofibroblasts.
* Basic Fibroblast Growth Factor (bFGF): Stimulates endothelial cell and fibroblast proliferation.
Clinical Pearl: The myofibroblast is the dominant cell type in both active granulation tissue (wound healing) and the involutional stage of Dupuytren disease. It contains alpha-smooth muscle actin (α-SMA), which provides the cellular contractile force that physically shortens the fascial cords.
Additional Pathogenic Factors
Several other biochemical and environmental factors have been theorized to play a role in the development of Dupuytren contracture:
* Increased glycosaminoglycan concentration.
* Altered matrix metalloproteinase (MMP) activity, leading to an imbalance between collagen synthesis and degradation.
* The presence of fibrofatty tissue between the skin and fascia.
* Microvascular ischemia and localized trauma generating free radicals.
* Genetic predisposition (ongoing DNA studies are actively investigating specific gene loci, particularly within the Wnt signaling pathway).
Stages of Disease Progression
Luck classically described the progression of Dupuytren disease through three distinct histological and clinical stages:
- Proliferative Stage: Characterized by the development of highly cellular nodules composed of fibroblasts and type III collagen. These nodules typically appear at the distal palmar crease over the MCP joints and distally over the PIP joints. They expand, displace subcutaneous fat, and fuse to the overlying skin, causing skin pitting.
- Involutional Stage: The nodules cease expanding and begin to contract. Fibroblasts align along lines of tension, and myofibroblasts become the predominant cell type. The contraction of these nodules places tension on the normal proximal fascia, inducing fascial hypertrophy and the formation of distinct "nodule-cord units."
- Residual Stage: The cellularity decreases significantly. The nodules shrink, leaving behind dense, acellular, type III collagen-rich fibrous cords responsible for the fixed joint contractures.
CLINICAL PRESENTATION AND ECTOPIC MANIFESTATIONS
Dupuytren disease most commonly affects the ulnar digits (ring and small fingers) and frequently presents asymmetrically.
Clinical presentation demonstrating mild, asymmetrical bilateral ulnar hand disease.

More diffuse bilateral disease with a severe, fixed flexion contracture of the proximal interphalangeal (PIP) joint of the right small finger.

Advanced palmar fascial disease with prominent pretendinous cords and skin tethering.
Dupuytren Diathesis
Patients with a strong genetic predisposition may exhibit "Dupuytren diathesis," characterized by an early age of onset, aggressive disease progression, high recurrence rates post-surgery, and the presence of ectopic fibromatosis outside the palmar fascia.
Ectopic deposits include:
* Ledderhose Disease (Plantar Fibromatosis): Nodules and cords within the plantar fascia.
* Garrod Nodules (Knuckle Pads): Fibrous deposits over the dorsal aspect of the PIP joints.
* Peyronie Disease: Fibromatosis of the tunica albuginea of the penis.

Bilateral medial plantar and medial great toe involvement characteristic of Ledderhose disease.

Dorsal proximal interphalangeal joint nodules, clinically known as Garrod nodules.
PATHOANATOMY OF THE PALMAR FASCIA
A profound understanding of the normal palmar fascial anatomy and its pathological transformation is mandatory for safe surgical intervention. The nomenclature established by McFarlane dictates that normal fascial structures are termed bands, while their diseased, contracted counterparts are termed cords.
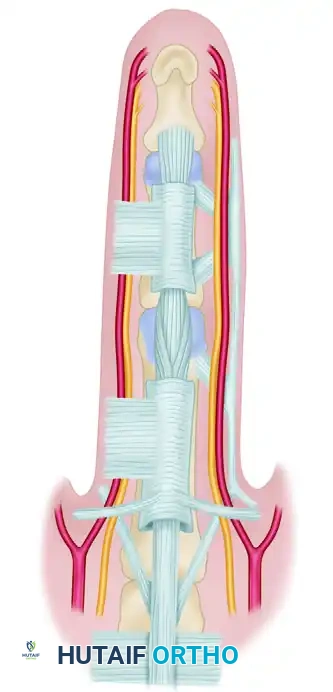
Diagrammatic representation of normal palmar and digital fascia.
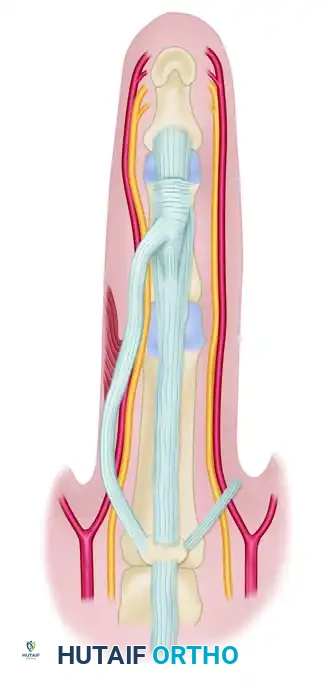
Diseased fascia demonstrating continuity with the pretendinous cord.
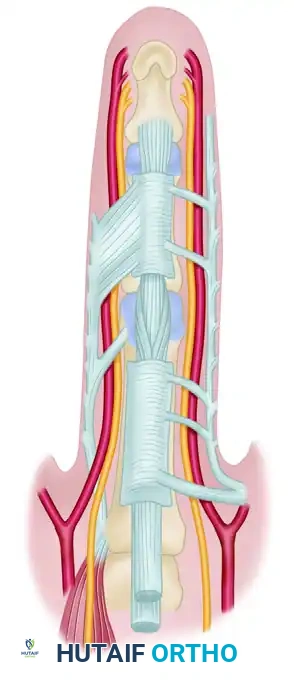
Other common fascial disease patterns illustrating the complex network of cords.
The Pretendinous Cord
The normal pretendinous band transforms into the pretendinous cord. This structure is nearly always responsible for the primary flexion contracture of the metacarpophalangeal (MCP) joint. It may attach to the skin of the distal palmar crease, the base of the proximal phalanx, or the flexor tendon sheath.
The Spiral Cord (Surgical Danger Zone)
The spiral cord is the most critical structure for the operating surgeon to understand, as it is responsible for the displacement of the digital neurovascular bundle.
The spiral cord is formed by the pathological amalgamation and contraction of four normally existing structures:
1. Pretendinous band
2. Spiral band
3. Lateral digital sheet
4. Grayson ligament
Surgical Warning: The normal spiral band runs dorsal to the neurovascular bundle proximally and volar to it distally. When these structures become diseased and contract into a spiral cord, the neurovascular bundle is drawn centrally (toward the midline of the finger) and superficially. This displacement is most common on the ulnar aspect of the little and ring fingers. Tedious, microscopic dissection is required to prevent catastrophic digital nerve transection.

Normal components of the fascia that eventually produce the spiral cord: pretendinous band, spiral band, lateral digital sheet, and Grayson ligament.
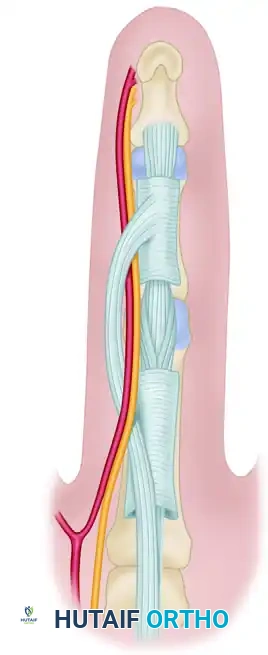
The diseased spiral cord demonstrating the dangerous medial and superficial displacement of the neurovascular bundle.
The Lateral Cord
The lateral digital cord may extend distally and contribute to flexion contractures of the distal interphalangeal (DIP) joint. The tissue plane between this cord and the overlying skin is exceptionally thin and must be developed sharply to avoid skin necrosis.
The Central Cord
Originating from the periosteum of the proximal phalanx and the fascia overlying the intrinsic muscles, the central cord courses distally (dorsal to the neurovascular bundles) and inserts into the middle phalanx or flexor tendon sheath. It is a primary driver of isolated PIP joint contractures.
The Retrovascular Cord
Described by Thomine, this longitudinally oriented fascia is located dorsal to the neurovascular bundle. While it is not believed to be the primary contributor to PIP joint flexion contractures, failure to excise a diseased retrovascular cord is a frequent cause of residual contracture or postoperative recurrence.
Spared Structures
It is a widely accepted anatomical rule that Cleland's ligaments (located dorsal to the neurovascular bundle) are spared from the fibroproliferative process of Dupuytren disease. Conversely, Grayson's ligaments (located volar to the bundle) are frequently involved.
While Skoog historically suggested that the superficial transverse palmar ligaments are always spared, modern consensus aligns with McFarlane: the superficial transverse ligaments, along with the natatory cords, are frequently involved and require excision, particularly in symptomatic thumb web space contractures.
SURGICAL MANAGEMENT: REGIONAL FASCIECTOMY
Indications for Surgery
Observation is appropriate for painless nodules without contracture. Surgical intervention is indicated when the contracture impairs hand function. Standard indications include:
* MCP joint contracture > 30 degrees.
* Any degree of PIP joint contracture that is progressive or functionally limiting (PIP contractures are notoriously difficult to correct fully and should be addressed earlier than MCP contractures).
* A positive Hueston's Table Top Test (inability to place the palm flat on a hard surface).
Preoperative Preparation and Positioning
- Anesthesia: Regional block (axillary or supraclavicular) or general anesthesia. Local anesthesia with epinephrine (WALANT) is increasingly utilized for select cases.
- Positioning: Supine with the operative arm extended on a hand table.
- Tourniquet: A well-padded upper arm tourniquet is essential for a bloodless field, typically inflated to 250 mm Hg.
- Magnification: Surgical loupes (minimum 2.5x to 3.5x) are mandatory for safe identification of displaced neurovascular bundles.
Step-by-Step Surgical Approach
1. Incision Design
The incision must allow wide exposure while preventing postoperative scar contracture.
* Bruner Zig-Zag Incision: The most common approach. Apices of the flaps must end at the mid-axial lines at the level of the flexion creases to prevent vascular compromise of the skin flaps.
* Longitudinal Incision with Z-Plasty: A straight longitudinal incision is made over the cord, and multiple Z-plasties are designed at the joint creases to lengthen the skin upon closure.
2. Skin Flap Elevation
The skin flaps are elevated off the underlying diseased fascia. This must be done with sharp dissection (using a #15 blade or tenotomy scissors). The subdermal plexus must be preserved. In areas of severe skin tethering (skin pits), the skin may be buttonholed; if the skin is non-viable, it should be excised.
3. Identification of the Neurovascular Bundle
Surgical Pearl: Never search for the neurovascular bundle in the zone of maximal disease. Always identify the digital nerve and artery proximally in the normal palmar fat, or distally in the normal finger, and trace them into the diseased tissue.
Once identified, the neurovascular bundle must be meticulously dissected free from the surrounding spiral and lateral cords. The surgeon must physically visualize the nerve being pulled medially and superficially by the spiral cord.
4. Excision of the Fascial Cords (Fasciectomy)
- Pretendinous Cord: Excised from its proximal origin in the palm to its distal insertion.
- Spiral Cord: Carefully divided and excised only after the neurovascular bundle is fully protected.
- Natatory Cords: Excised to restore digital abduction and web space compliance.
- Retrovascular Cords: Must be sought out dorsal to the neurovascular bundle and excised to maximize PIP joint extension.
5. Joint Release (If Necessary)
If PIP joint extension is not achieved after complete fasciectomy, a sequential joint release may be required:
1. Release of the flexor tendon sheath.
2. Release of the accessory collateral ligaments.
3. Release of the volar plate (rarely required and carries a risk of joint instability).
6. Hemostasis and Closure
The tourniquet is deflated prior to closure to achieve meticulous hemostasis, minimizing the risk of postoperative hematoma.
* Primary Closure: Performed if the skin reaches without tension.
* McCash Open Palm Technique: Transverse palmar incisions are left open to heal by secondary intention. This allows for hematoma drainage and prevents skin tension, though it requires prolonged wound care.
* Skin Grafting (Dermofasciectomy): Full-thickness skin grafts are utilized if the overlying skin is heavily diseased or excised. This technique significantly lowers the local recurrence rate and is highly recommended for recurrent disease or severe Dupuytren diathesis.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Optimal surgical outcomes rely heavily on rigorous postoperative hand therapy.
* Immediate Post-Op: The hand is placed in a bulky, non-compressive dressing with a volar plaster splint holding the MCP and PIP joints in maximal safe extension.
* Days 3-5: The bulky dressing is removed. A custom thermoplastic extension splint is fabricated.
* Active Therapy: Early active range of motion (ROM) exercises are initiated to prevent tendon adhesions and joint stiffness.
* Splinting Regimen: The extension splint is typically worn continuously (except during exercises) for the first 3 weeks, and then transitioned to nighttime wear for 3 to 6 months to prevent recurrent contracture.
COMPLICATIONS AND PITFALLS
- Digital Nerve Injury: The most devastating intraoperative complication, occurring in 1-3% of primary cases and up to 10% of revisions. Immediate microsurgical epineural repair is required if transected.
- Digital Artery Injury: May lead to digital ischemia, especially if bilateral digital arteries are compromised.
- Hematoma: The most common postoperative complication. It can lead to skin flap necrosis, infection, and severe scarring. Meticulous hemostasis and the use of drains or the McCash technique mitigate this risk.
- Complex Regional Pain Syndrome (CRPS) / Flare Reaction: Characterized by disproportionate pain, swelling, and stiffness. Treated with aggressive therapy, sympathetic blocks, and short-course corticosteroids.
- Recurrence: Highly common, particularly in patients with Dupuytren diathesis. Patients must be counseled preoperatively that surgery is a treatment for the contracture, not a cure for the underlying genetic disease.
You Might Also Like
