Dupuytren Contracture: Prognosis, Indications, and Surgical Techniques

Key Takeaway
Dupuytren contracture management requires a nuanced understanding of disease histopathology, prognostic factors, and precise surgical execution. Operative intervention is typically indicated for metacarpophalangeal joint contractures exceeding 30 degrees or any proximal interphalangeal joint contracture causing functional impairment. Surgical options range from percutaneous needle aponeurotomy to partial fasciectomy and dermatofasciectomy. Meticulous dissection, particularly regarding neurovascular bundle displacement by spiral cords, is paramount to minimizing complications and optimizing postoperative functional recovery.
Comprehensive Introduction and Patho-Epidemiology
Dupuytren disease is a complex, benign, fibroproliferative disorder of the palmar fascia characterized by the progressive formation of pathological nodules and cords, ultimately leading to debilitating, irreversible flexion contractures of the digits. The fundamental histopathology involves the aberrant transformation of normal fascial fibroblasts into myofibroblasts. These specialized cells exhibit aggressive contractile properties driven by the intracellular expression of alpha-smooth muscle actin ($/alpha$-SMA) and are heavily regulated by profibrotic cytokines, most notably transforming growth factor-beta 1 (TGF-$/beta$1), basic fibroblast growth factor (bFGF), and platelet-derived growth factor (PDGF). The disease progresses through three distinct histological stages: the proliferative phase (highly cellular, rich in myofibroblasts and Type III collagen), the involutional phase (alignment of myofibroblasts along lines of tension), and the residual phase (acellular, dense, avascular cords composed primarily of Type I collagen).
Successful management of Dupuytren contracture requires the orthopedic surgeon to possess a profound, three-dimensional understanding of palmar fascial anatomy, the biomechanical behavior of pathological cords, and the patient-specific prognostic factors that dictate the timing, modality, and extent of surgical intervention. Operating during the active, highly cellular proliferative stage is fraught with complications, often resulting in ill-defined surgical planes, massive postoperative flare reactions, and paradoxical stiffening.
The prognosis in Dupuytren contracture is highly variable and intimately linked to the patient's biological predisposition. The concept of "Dupuytren's diathesis," originally popularized by Hueston, refers to a constellation of constitutional risk factors that predispose a patient to aggressive disease, early onset, rapid progression, and a notoriously high rate of postoperative recurrence. The extent of any surgical operation must be meticulously tailored to these prognostic indicators.
- Heredity and Genetics: A strong family history, particularly with an autosomal dominant inheritance pattern exhibiting variable penetrance, indicates that the lesion is likely to progress rapidly. Early age of onset (typically before the fifth decade) in these patients is a hallmark of an aggressive diathesis. Recent genome-wide association studies (GWAS) have identified multiple susceptibility loci, predominantly involving the Wnt signaling pathway, which is critical in fibromatosis pathogenesis.
- Sex: The lesion typically begins later in life and progresses more slowly in women, who often accommodate better to the resulting deformity. However, landmark studies by Zemel et al. demonstrated that long-term surgical outcomes are paradoxically worse in women than in men. Postoperative flare reactions, including devastating complex regional pain syndrome (CRPS), are twice as likely in the female demographic, necessitating highly cautious preoperative counseling.
- Epilepsy: Historically, earlier literature positively associated Dupuytren contracture with epilepsy and the long-term use of barbiturates (e.g., phenobarbital). However, contemporary, highly powered epidemiological studies by Geoghegan et al. have conclusively debunked this myth, demonstrating that neither epilepsy nor antiepileptic medications are independently associated with the disease when confounding variables are controlled.
- Diabetes Mellitus: Diabetes is a well-established, independent risk factor. The severity of the fibroproliferative response correlates directly with the medical management required; patients requiring exogenous insulin therapy are significantly more likely to develop Dupuytren disease compared to those managed with diet modification, metformin, or sulfonylureas. Diabetic patients often present with a milder, more diffuse form of the disease but are at a higher risk for microvascular complications postoperatively.
- Alcoholism and Smoking: Microvascular ischemia and free radical damage play a central role in the pathogenesis of fascial fibrosis. Godtfredsen et al. found a strict, dose-dependent relationship between alcohol intake, tobacco smoking, and disease severity. The combination of these two factors conveys a remarkably high risk for rapid progression and postoperative recurrence, likely due to chronic hypoxia stimulating fibroblast proliferation.
- Location and Extent of Disease: Bilateral hand involvement, especially when associated with ectopic fibroproliferative deposits such as knuckle pads (Garrod's nodes), plantar fibromatosis (Ledderhose disease), or penile fibromatosis (Peyronie's disease), signifies a severe, systemic diathesis. Progression is characteristically more rapid on the ulnar side of the hand, preferentially affecting the ring and small fingers.
- Behavior of Disease: The historical biological behavior of the disease in a given patient—whether previously treated or observed longitudinally—remains the most reliable predictor of its future clinical course.

Detailed Surgical Anatomy and Biomechanics
A masterful command of the normal and pathological anatomy of the palmar fascia is the absolute prerequisite for safe surgical intervention. The normal palmar fascia is a complex, three-dimensional aponeurotic framework designed to stabilize the palmar skin during gripping while protecting the underlying neurovascular structures. It is composed of longitudinal, transverse, and vertical fibers.
Normal Fascial Structures
- Pretendinous Bands: Longitudinal fibers originating from the palmaris longus tendon (or palmar fascia apex) that insert into the skin, the deep transverse metacarpal ligament, and the base of the proximal phalanx.
- Superficial Transverse Palmar Ligament: Transverse fibers lying deep to the pretendinous bands in the mid-palm. Crucially, this structure is rarely involved in Dupuytren disease.
- Natatory Ligaments: Transverse fibers in the web spaces that resist digital abduction.
- Spiral Bands: Fibers that originate from the pretendinous band, pass deep to the neurovascular bundle, and insert into the lateral digital sheet.
- Lateral Digital Sheet: Fascia running along the lateral aspect of the digit, receiving contributions from the natatory and spiral bands.
- Grayson's and Cleland's Ligaments: Grayson's ligaments are volar to the neurovascular bundle and are frequently involved in Dupuytren disease. Cleland's ligaments are dorsal to the neurovascular bundle and are strictly spared from the disease.
Pathological Cords and Biomechanics
In Dupuytren disease, normal fascial bands hypertrophy and contract to become pathological cords. The biomechanical consequences of these cords dictate the clinical deformity.
- Pretendinous Cord: Arises from the pretendinous band. Contraction causes isolated metacarpophalangeal (MCP) joint flexion contractures.
- Natatory Cord: Arises from the natatory ligament. Contraction causes web space contractures, severely limiting digital abduction.
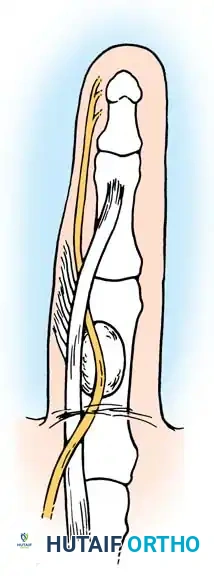
- Spiral Cord: This is the most surgically treacherous structure. It is formed by the confluence of four structures: the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament. As the spiral cord contracts, it causes proximal interphalangeal (PIP) joint flexion. More importantly, its biomechanical contraction uniquely displaces the digital neurovascular bundle centrally, superficially, and proximally. The nerve is brought perilously close to the skin at the level of the proximal phalanx, placing it at extreme risk of iatrogenic transection during surgical exposure.
- Retrovascular Cord (of Thomine): A longitudinal cord running dorsal to the neurovascular bundle. It contributes to recalcitrant PIP joint contractures and must be excised to achieve full extension.
Exhaustive Indications and Contraindications
The decision to proceed with treatment, whether nonoperative or operative, hinges on the degree of functional impairment, the specific joints involved, and the biological phase of the disease. In the absence of contractures, surgical treatment is strictly not indicated. Painless palmar nodules alone do not warrant surgery unless they cause severe discomfort, skin pitting, or maceration.
Nonoperative Management
Nonoperative treatment regimens focus on altering the fundamental histopathology of the myofibroblast or enzymatically degrading the established collagen matrix. Bisson et al. demonstrated that nodule-derived fibroblasts possess significantly greater contractile properties and force generation than cord-derived or normal carpal tunnel ligament fibroblasts, making the nodule the biological epicenter of the disease.
- Corticosteroid Injections: Ketchum and Donahue studied the modification of Dupuytren nodules via intralesional injection of triamcinolone acetonide. After an average of 3.2 injections per nodule, 97% of hands exhibited softening or flattening. While complete resolution is rare, nodule reactivation was delayed by up to 3 years in 50% of patients. This is highly effective for painful, rapidly growing nodules in the proliferative phase.
- Clostridial Collagenase Injections: Enzymatic fasciotomy using Clostridium histolyticum collagenase (CCH) has revolutionized nonoperative care. Badalamente et al. established the safety and efficacy of this enzymatic degradation. CCH specifically targets and cleaves Type I and Type III collagen. It provides prompt MCP and PIP joint contracture release when followed by a controlled manipulation 24 to 48 hours post-injection. It is particularly indicated for palpable, distinct cords in patients who are poor surgical candidates.

Operative Indications and Timing
The classic "Hueston's tabletop test" is utilized to screen patients; an inability to place the hand flat on a table indicates a functional contracture. Timing is critical. Surgery should ideally be delayed until the disease matures into the "residual phase" (dense, avascular cords).
| Parameter | Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| MCP Joint | Contracture $/ge$ 30 degrees | Painless palmar nodules without contracture | Severe medical comorbidities precluding anesthesia |
| PIP Joint | Contracture $/ge$ 15 to 20 degrees | Active, highly cellular "proliferative stage" (high flare risk) | Slowly progressing disease in elderly, low-demand patients |
| Web Space | Severe adduction contracture limiting span | Prophylactic surgery to prevent future contracture | Patient non-compliance with postoperative splinting |
| Skin/Soft Tissue | Severe skin pitting, maceration, or recurrent infection | Active complex regional pain syndrome (CRPS) | Heavy smoking/alcohol abuse (high risk of flap necrosis) |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential to minimize morbidity. The surgeon must meticulously assess the nutritional status of the palmar skin, the presence of fixed joint subluxations, and the patient’s overall diathesis score.
Anesthesia and Positioning
Historically, Dupuytren surgery was performed under general anesthesia or regional brachial plexus block with a pneumatic tourniquet. Contemporary practice increasingly utilizes WALANT (Wide Awake Local Anesthesia No Tourniquet). Using a mixture of 1% lidocaine with 1:100,000 epinephrine (buffered with sodium bicarbonate), the surgeon achieves excellent hemostasis without the ischemic pain of a tourniquet. This allows intraoperative active movement by the patient, enabling the surgeon to immediately assess the adequacy of the contracture release and verify flexor tendon integrity. If a tourniquet is used, the limb is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mmHg. The patient is positioned supine with the arm extended on a radiolucent hand table.
Incision Design and Exposure Strategy
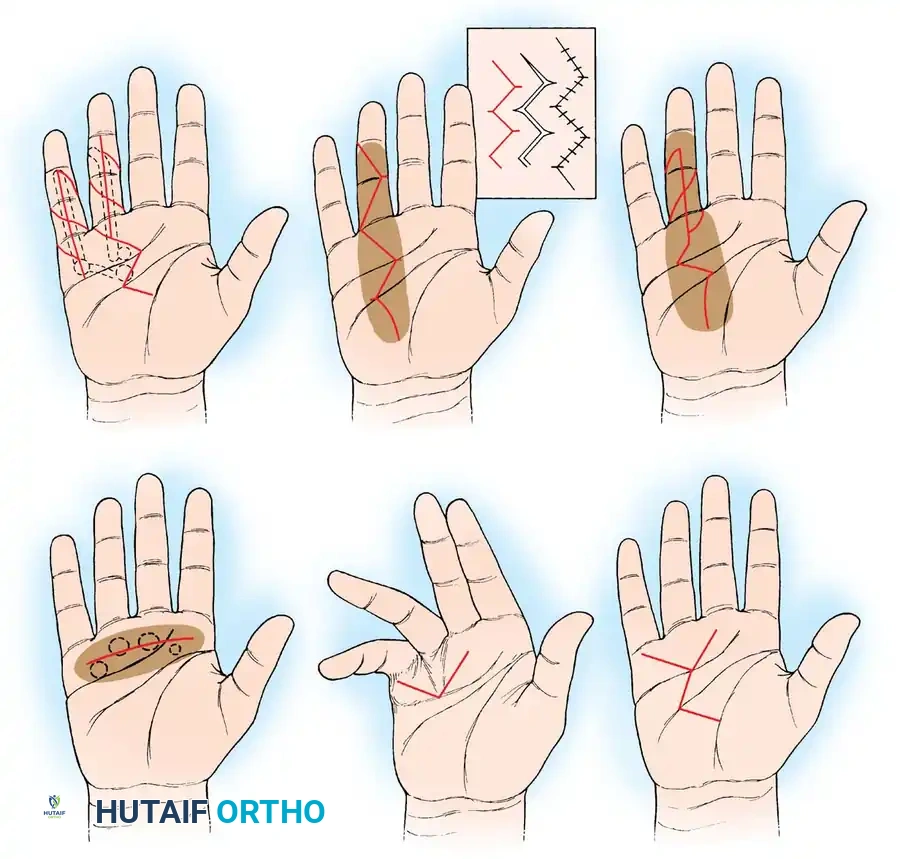
Exposure is paramount. The incision must allow full visualization of the neurovascular bundles from proximal to distal while preventing postoperative linear scar contracture.
- Zigzag (Bruner) Incisions: The preferred choice for longitudinal digital exposure. They prevent linear scar contracture but must be meticulously designed so the apices of the flaps do not cross the transverse digital flexion creases at right angles. The flaps must have broad bases to ensure adequate dermal perfusion.
- Z-Plasties: Used to lengthen contracted palmar skin. A midline longitudinal incision over the cord can be converted into multiple Z-plasties during closure. The angles of the Z-plasty limbs are typically designed at 60 degrees to maximize length gain (up to 73%).
- Transverse Incisions (McCash Technique): Useful in the distal palm when the disease is well-defined. The transverse incision is left open to heal by secondary intention, which allows for hematoma drainage, eliminates skin tension, and paradoxically results in rapid, pain-free healing with excellent functional outcomes.
Step-by-Step Surgical Approach and Fixation Technique
The appropriate procedure depends entirely on the degree of contracture, skin viability, and the patient's diathesis. The surgical armamentarium ranges from minimally invasive fasciotomies to complex salvage arthrodeses requiring rigid fixation.
1. Subcutaneous Fasciotomy (Luck Technique)
This minimally invasive procedure is primarily indicated for elderly patients, those with severe medical comorbidities, or as a preliminary staging procedure for severe, unyielding contractures prior to definitive fasciectomy. It is most effective for isolated, mature pretendinous cords causing MCP joint flexion.
Surgical Warning: Subcutaneous fasciotomy is strictly contraindicated for laterally placed digital cords or spiral cords due to the extreme risk of digital nerve transection. It must only be performed for centrally located, palpable palmar cords.
Technique:
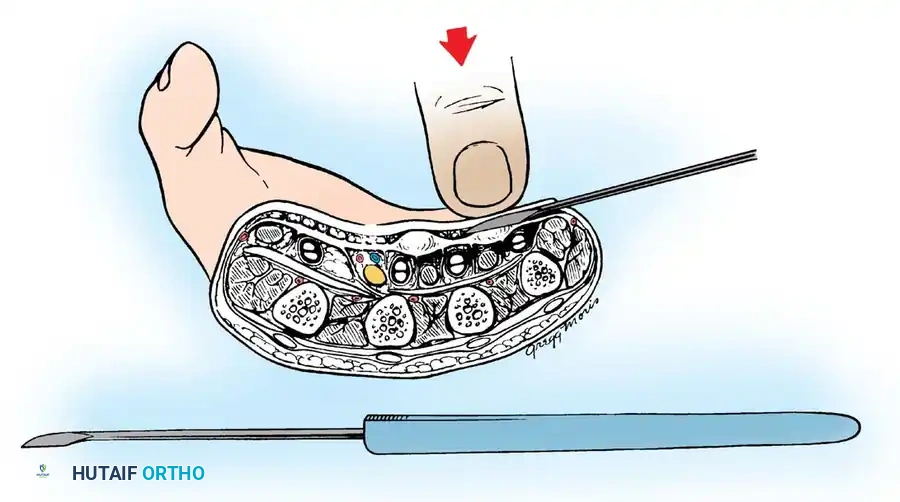
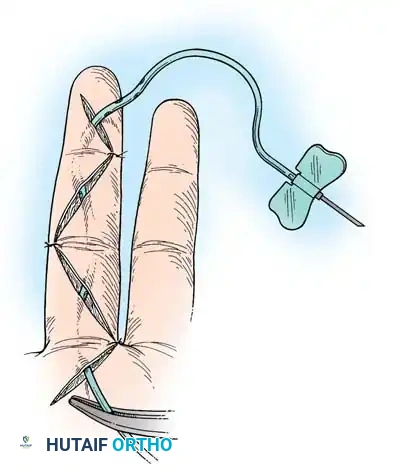
1. Using a pointed scalpel (e.g., #11 blade), make small puncture wounds on the ulnar side of the diseased palmar fascia at three distinct levels: distal to the palmar fascia apex, near the proximal palmar crease, and at the distal palmar crease.
2. Insert a small tenotomy knife or a specialized Luck fasciotome (resembling a myringotome) through the puncture wounds. The blade must remain perfectly parallel to the palm, passing immediately beneath the dermis but superficial to the fascial cord.
3. Extend the fingers to place the fascial cord under maximal biomechanical tension.
4. Turn the blade edge 90 degrees toward the palmar fascia and divide the cord using gentle pressure or a controlled rocking motion. Never use a sawing motion, as this risks erratic transection of deeper structures.
5. A sudden, palpable loss of gritty resistance indicates complete division of the cord.
6. Undermine the corrugated skin using the blade parallel to the dermis to release dermal tethering and skin pits.
2. Partial (Selective) Fasciectomy
This remains the gold standard and most frequently performed operation worldwide. It excises only the macroscopically diseased fascia, balancing adequate contracture release with minimized surgical morbidity.
Technique:
1. Preparation: Exsanguinate the limb and inflate the pneumatic tourniquet (if WALANT is not utilized). Loupe magnification (minimum 2.5x to 3.5x) is absolutely mandatory for neurovascular dissection.
2. Incision: Outline a Bruner zigzag incision over the digit, extending proximally into the palm. Incorporate severe skin pits into the flap design so they can be sharply excised or carefully released from the underlying cord.
3. Flap Elevation: Elevate full-thickness skin flaps using sharp dissection. The dissection plane is immediately deep to the dermis. Great care must be taken to preserve the delicate subdermal vascular plexus; violating this plane leads to devastating full-thickness flap necrosis.
4. Neurovascular Identification: This is the most critical and perilous step of the operation. The normal anatomy is grossly distorted by the pathological cords.

- Dissection: Identify the neurovascular bundle in the proximal palm where the anatomy remains normal and undisturbed by the disease process. Trace it systematically distally into the diseased tissue.
- Excision: Carefully dissect the diseased cord away from the nerve and artery. Retract the neurovascular bundle safely using vessel loops and excise the cord in its entirety from proximal to distal.
- Skoog's Modification: Skoog emphasized that a definitive cleavage plane exists between the longitudinal pretendinous fibers and the transverse palmar ligament. The superficial transverse palmar ligament is rarely involved in Dupuytren's and must be preserved to protect the underlying neurovascular structures and flexor tendons.

Management of the Stiff PIP Joint
Following thorough fasciectomy, residual PIP joint flexion deformity is common. This is often due to isolated cords passing volar to the rotation axis of the PIP joint, inserting onto the flexor tendon sheath or the base of the middle phalanx. If excision of all fascial cords (including the retrovascular cords of Thomine) fails to correct the contracture, a volar joint capsulotomy and release of the checkrein ligaments may be required. However, Weinzweig et al. demonstrated that PIP contractures >60 degrees are typically only correctable to about 50% of the existing deformity, regardless of extensive capsulotomy. Furthermore, capsulotomy patients lose an average of 16 degrees of terminal flexion.
3. Dermatofasciectomy with Skin Grafting (Hueston's Procedure)
Advocated by Hueston, this aggressive procedure is indicated for young patients with a severe Dupuytren's diathesis, highly recurrent disease, or when the palmar skin is so intimately involved with the fascia (severe dermal infiltration) that it cannot be salvaged without compromising viability.
Technique and Fixation:
The diseased fascia and the overlying involved skin are excised en bloc. The resulting defect is covered with a full-thickness skin graft (FTSG) typically harvested from the hypothenar eminence, groin, or inner arm. Recurrence beneath a skin graft is exceptionally rare, as the graft appears to act as a biological "firebreak" against myofibroblast proliferation. Fixation of the graft is critical: the graft is sutured into the defect using 5-0 chromic gut or nylon, and a tie-over bolster dressing (using Xeroform and fluffed gauze) is firmly secured over the graft to prevent shearing forces and hematoma accumulation, ensuring optimal inosculation and neovascularization.
4. Salvage Procedures: Amputation and Arthrodesis
In cases of severe, neglected PIP joint contractures (e.g., >90 degrees in the small finger) where the digit is non-functional, interferes with daily activities, or where the neurovascular bundles are hopelessly encased in scar tissue, salvage procedures are indicated.
- Amputation: A ray amputation or amputation through the PIP joint may be necessary. The skin from the filleted finger can be preserved as a vascularized pedicle flap to cover large palmar skin defects, turning a liability into a reconstructive asset.
- Arthrodesis: Resection of the severely contracted PIP joint and arthrodesis in a functional position (typically 30-40 degrees of flexion for the index/long fingers, and 40-50 degrees for the ring/small fingers) shortens the finger, relieving tension on the neurovascular bundles, and permanently eliminates the risk of recurrent contracture. Fixation Technique: The joint surfaces are prepared with flat cuts or cup-and-cone reamers. Rigid fixation is achieved using crossed 0.045-inch Kirschner wires (K-wires), a tension band construct, or modern headless compression screws to ensure bony union.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for Dupuytren disease carries a significant complication profile, demanding meticulous technique and vigilant postoperative care. Hematoma formation is the most common complication and serves as a potent stimulus for excessive scarring, flap necrosis, and severe flare reactions.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management & Prevention |
|---|---|---|---|
| Hematoma | 2% - 15% | Rebound vasodilation post-tourniquet, inadequate hemostasis. | Prevention: Deflate tourniquet prior to closure, bipolar cautery. Management: Immediate evacuation to prevent flap necrosis. |
| Digital Nerve Injury | 1% - 3% | Transection due to central/superficial displacement by the spiral cord. | Prevention: Proximal-to-distal dissection. Management: Immediate microsurgical primary epineurial repair. |
| Digital Artery Injury | 2% - 5% | Iatrogenic transection during deep retrovascular cord excision. | If unilateral, observe capillary refill. If bilateral or ischemic, immediate microsurgical vein grafting or primary repair. |
| Skin Flap Necrosis | 3% - 10% | Dissection too superficial (violating subdermal plexus), tension on closure. | Allow to heal by secondary intention; avoid aggressive debridement early. Use McCash open palm technique prophylactically. |
| Flare Reaction / CRPS | 5% - 10% | Exaggerated inflammatory response, higher in females and severe diathesis. | Aggressive hand therapy, systemic corticosteroids (Medrol dose pack), sympathetic nerve blocks, Gabapentin. |
| Recurrence | 20% - 50% (at 5 yrs) | Incomplete excision, aggressive diathesis, presence of ectopic disease. | Dermatofasciectomy with FTSG (firebreak effect), or salvage arthrodesis/amputation for severe multi-recurrent digits. |
Phased Post-Operative Rehabilitation Protocols
The surgical release of a Dupuytren contracture is only half the battle; the final functional outcome is heavily dependent on a rigorous, phased postoperative rehabilitation protocol directed by a certified hand therapist (CHT). Meticulous hemostasis is mandatory before closure.
- Deflate the tourniquet and achieve pinpoint hemostasis using bipolar electrocautery.
- If a transverse palmar incision was used, it may be left open to heal by secondary intention (McCash open palm technique).
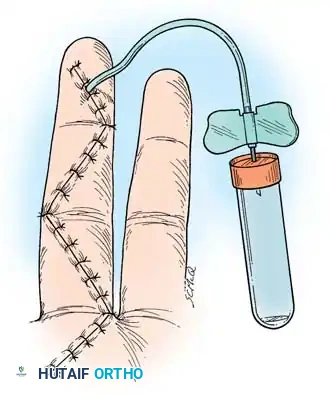
- Close zigzag incisions with interrupted 5-0 or 4-0 non-absorbable sutures (e.g., Nylon or Prolene) without tension.
- Insert a small closed-suction drain or a passive capillary drain (e.g., Penrose) if dead space is significant.
Phase I: Protective Phase (Days 0 to 14)
- Immobilization: In the operating room, apply a bulky, non-compressive soft dressing with a volar plaster or fiberglass splint holding the MCP joints in extension and the PIP joints in extension (or slight flexion if neurovascular tension or skin blanching is a concern upon full extension).
- Edema Control: Strict elevation of the hand above the level of the heart for the first 48-72 hours. Gentle active range of motion (AROM) of the uninvolved digits, wrist, elbow, and shoulder is encouraged immediately.
- Wound Care: The first dressing change occurs at 3 to 5 days postoperatively. Sutures are typically removed between 10 and 14 days, depending on flap viability and wound edge epithelialization.
Phase II: Mobilization Phase (Weeks 2 to 6)
- Splinting: The bulky surgical splint is transitioned to a custom-molded thermoplastic resting hand splint. This is worn strictly at night and intermittently during the day.
- Range of Motion: Aggressive AROM and passive range of motion (PROM) exercises are initiated. Tendon gliding exercises are crucial to prevent flexor tendon adhesions within the surgical bed.
- Scar Management: Once the wounds are fully closed and scabs have resolved, aggressive scar massage using silicone gel pads and elastomer putty is
