Operative Management of Trigger Finger & De Quervain Disease

Key Takeaway
Stenosing tenosynovitis, encompassing trigger finger and de Quervain disease, requires precise surgical intervention when conservative measures fail. This guide details the step-by-step operative techniques for A1 pulley release, percutaneous methods, and first dorsal compartment reconstruction. Mastery of these procedures demands a thorough understanding of hand biomechanics, neurovascular anatomy, and meticulous surgical execution to restore optimal tendon glide and prevent recurrence.
Comprehensive Introduction and Patho-Epidemiology
Stenosing tenosynovitis represents a ubiquitous yet biomechanically complex spectrum of orthopaedic pathology characterized by a critical spatial mismatch between a hypertrophied, inflamed tendon (or its surrounding synovial sheath) and the rigid, unyielding fibro-osseous tunnel through which it must glide. Within the highly specialized anatomical confines of the hand and wrist, this pathological phenomenon most frequently manifests as Trigger Finger—involving the first annular (A1) pulley of the digital flexor tendon sheath—and de Quervain Disease, which involves the entrapment of the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons within the first dorsal extensor compartment of the wrist. These conditions account for a substantial volume of hand surgery consultations and require a nuanced understanding of upper extremity biomechanics to manage effectively.
Contrary to historical nomenclature suggesting a primary inflammatory etiology ("tenosynovitis"), contemporary histological analyses demonstrate that the fundamental pathological process in both Trigger Finger and de Quervain Disease is one of fibrocartilaginous metaplasia and myxoid degeneration. The retinacular structures and the pulleys undergo significant thickening, characterized by a proliferation of chondrocytes and an extracellular matrix heavily laden with type III collagen and mucopolysaccharide ground substance. True inflammatory cells (such as macrophages and lymphocytes) are notably sparse or absent in the chronic phases of the disease. This degenerative hypertrophy leads to a mechanical constriction that severely impedes the normal, frictionless excursion of the underlying tendons.
Epidemiologically, these conditions exhibit a strong predilection for the female demographic, typically presenting in the fifth and sixth decades of life. The lifetime risk for developing a trigger digit in the general population is approximately 2% to 3%, but this incidence skyrockets to over 10% in patients with concomitant endocrine or metabolic disorders, most notably diabetes mellitus. Diabetic patients not only present with multiple digit involvement more frequently but also demonstrate a notoriously recalcitrant clinical course, with significantly lower success rates following conservative interventions such as corticosteroid injections. Similarly, de Quervain disease is highly prevalent among postpartum women (often termed "baby wrist"), driven by a combination of hormonal fluid retention and the repetitive biomechanical stress of lifting an infant with a radially deviated and flexed wrist.
When conservative modalities—encompassing targeted corticosteroid injections, rigid or semi-rigid splinting, and nonsteroidal anti-inflammatory drugs (NSAIDs)—fail to provide durable symptomatic relief, surgical intervention becomes the definitive gold standard. This comprehensive masterclass details the evidence-based surgical techniques, highly specific biomechanical considerations, and advanced reconstructive options for both conditions. The protocols and anatomical insights provided herein are meticulously tailored for the practicing orthopaedic surgeon, hand specialist, and surgical resident seeking to master the operative management of stenosing tenosynovitis.
Detailed Histopathology and Cellular Mechanisms
The microscopic evaluation of the A1 pulley in trigger finger and the extensor retinaculum in de Quervain disease reveals a striking departure from normal fascial architecture. Normal pulleys are composed of highly organized, parallel bundles of type I collagen that provide immense tensile strength with minimal bulk. In the pathological state, the tissue undergoes a profound transformation into a fibrocartilaginous phenotype. The inner gliding layer of the pulley, which is normally lined by a delicate layer of synoviocytes, becomes hyperplastic and disorganized. This is accompanied by the focal deposition of chondroid-like cells and a shift towards type III collagen synthesis, which is mechanically inferior and significantly bulkier.
Within the tendon itself, particularly in trigger digits, the repetitive mechanical impingement against the thickened A1 pulley induces the formation of a reactive, localized swelling known as the Notta nodule. This nodule is not a true neoplasm or granuloma but rather a localized area of intratendinous myxoid degeneration and collagen fiber disarray. As the nodule enlarges, it acts as a mechanical block. During active flexion, the flexor musculature generates sufficient force to pull the nodule proximally through the stenotic A1 pulley. However, the weaker extensor mechanism struggles to pull the nodule back distally during extension, resulting in the characteristic "catching" or "locking" phenomenon that defines the clinical presentation.
In de Quervain disease, the histopathological changes are virtually identical, localized to the extensor retinaculum overlying the radial styloid. The fibro-osseous tunnel becomes severely constricted by the thickened retinaculum, trapping the APL and EPB tendons. The mechanical friction is exacerbated by the sharp angulation of these tendons as they course over the radial styloid, creating a fulcrum effect that amplifies shear stress. Understanding this non-inflammatory, degenerative cellular mechanism is critical for the orthopaedic surgeon, as it explains why systemic anti-inflammatory medications are often ineffective and why mechanical release (either via corticosteroid-induced atrophy of the tissue or surgical division) is ultimately required for definitive resolution.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the surgical anatomy is the absolute prerequisite for the safe and effective operative management of stenosing tenosynovitis. The flexor tendon pulley system of the digits is an intricate biomechanical construct designed to maintain the flexor tendons in close apposition to the phalangeal longitudinal axis, thereby maximizing the mechanical advantage (moment arm) during active flexion. This system is composed of five sturdy annular pulleys (A1 through A5), which provide the primary mechanical restraint against tendon bowstringing, and three delicate, crisscrossing cruciate pulleys (C1 through C3), which allow the flexor sheath to collapse and expand smoothly during digital flexion without buckling.
The A1 pulley, the primary anatomical locus of trigger finger pathology, arises from the volar plate of the metacarpophalangeal (MCP) joint and the extreme proximal base of the proximal phalanx. It spans approximately 1 centimeter in length and is the first significant mechanical constriction point for the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons as they exit the palm. Immediately distal to the A1 pulley lies the A2 pulley, which originates directly from the periosteum of the proximal half of the proximal phalanx. The A2 pulley is the most critical biomechanical structure in the digit; iatrogenic injury to the A2 pulley during an overzealous trigger finger release results in catastrophic flexor tendon bowstringing, leading to a profound loss of mechanical advantage, a severe active flexion deficit, and a debilitating functional impairment of the hand.
The neurovascular anatomy surrounding the A1 pulley demands meticulous surgical respect. The common digital nerves bifurcate into proper digital nerves in the distal palm, coursing volar and parallel to the flexor tendon sheath. In the middle, ring, and small fingers, these nerves are relatively protected by the surrounding adipose tissue and their slightly lateral position. However, the radial digital nerve of the thumb is uniquely vulnerable. It courses obliquely across the flexor sheath just proximal to the MCP flexion crease, placing it in direct peril during both open and percutaneous trigger thumb releases. Furthermore, the digital arteries, running dorsal to the nerves, provide the critical vincula (blood supply) to the flexor tendons; inadvertent injury to these vessels can lead to localized tendon ischemia and subsequent rupture.
The First Dorsal Compartment and Radial Nerve Anatomy
The first dorsal extensor compartment of the wrist is a highly specialized fibro-osseous tunnel situated directly over the radial styloid process. Its roof is formed by the extensor retinaculum, and its floor is the osseous groove of the radius. This compartment houses the tendons of the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB). The anatomical variations within this compartment are notoriously frequent and are the primary cause of surgical failure in de Quervain disease. The APL tendon is rarely a single structure; it typically consists of multiple tendon slips (ranging from two to four, and occasionally up to seven) that insert variably onto the base of the first metacarpal, the trapezium, and the fascia of the abductor pollicis brevis.
The EPB tendon, in contrast, is usually a single slip that inserts onto the base of the proximal phalanx of the thumb. Crucially, in up to 60% of the general population, the first dorsal compartment is divided by a distinct intracompartmental longitudinal septum, effectively creating a separate subcompartment for the EPB tendon. Failure to recognize and surgically release this isolated EPB subcompartment is the most common etiology for persistent, recalcitrant de Quervain disease post-operatively. The surgeon must routinely assume the presence of this septum until definitively proven otherwise through meticulous intraoperative exploration.

Figure: Cross-sectional anatomy demonstrating the first dorsal compartment. Note the distinct septation separating the APL and EPB tendons, a frequent site of missed pathology.
Superficial to the first dorsal compartment lies the superficial branch of the radial nerve (SBRN). The SBRN emerges from beneath the brachioradialis muscle approximately 9 centimeters proximal to the radial styloid and arborizes extensively over the first dorsal compartment to provide sensation to the dorsoradial aspect of the hand. The nerve branches are highly variable and often intertwine with the superficial venous plexus. Iatrogenic injury to the SBRN—whether via direct transection, traction neuropraxia, or entrapment in postoperative scar tissue—results in a devastating, highly symptomatic neuroma. This complication often eclipses the original de Quervain pathology in terms of patient morbidity, causing severe, burning, neuropathic pain that is extraordinarily difficult to manage.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for stenosing tenosynovitis must be predicated on a thorough clinical evaluation, a documented failure of appropriate conservative modalities, and a careful assessment of the patient's functional demands and comorbidities. Surgery is rarely indicated as a first-line treatment, except in highly specific clinical scenarios such as a rigidly locked digit that cannot be passively corrected, or in the case of pediatric trigger thumb, which has a drastically different natural history than adult trigger digits. The primary goal of surgery is the restoration of unimpeded tendon glide, the elimination of pain, and the prevention of secondary joint contractures.
For trigger finger, the indications are typically guided by the Quinnell grading system or the Green classification. Patients presenting with Grade III (actively locked digit requiring passive manipulation to extend) or Grade IV (rigidly locked digit with fixed flexion contracture) who have failed at least one, and typically two, precisely placed corticosteroid injections are definitive surgical candidates. Furthermore, patients with insulin-dependent diabetes mellitus represent a unique cohort; literature demonstrates that the efficacy of corticosteroid injections in this population is significantly diminished, with recurrence rates approaching 50-60%. Consequently, a lower threshold for surgical intervention is justified in diabetic patients to prevent prolonged morbidity and the development of fixed proximal interphalangeal (PIP) joint contractures.
In the context of de Quervain disease, surgical release is indicated for patients who continue to experience debilitating dorsoradial wrist pain, functional limitation in grip and pinch strength, and a positive Finkelstein or Eichhoff test despite a minimum of three to six months of conservative management. This conservative trial should rigidly include customized thumb spica splinting and at least one ultrasound-guided corticosteroid injection into the first dorsal compartment (ensuring infiltration into both the APL and EPB subcompartments). Severe, unrelenting pain that severely impacts activities of daily living, or the presence of an impending tendon rupture (though rare), accelerates the timeline for surgical decompression.
Table of Indications and Contraindications
| Pathology | Definitive Surgical Indications | Relative / Absolute Contraindications |
|---|---|---|
| Trigger Finger | - Failure of 1-2 corticosteroid injections. - Actively or passively locked digit (Quinnell Grade III/IV). - Severe triggering in diabetic patients (low injection efficacy). - Pediatric trigger thumb unresolved by age 2-3 years. - Concomitant severe inflammatory arthritis requiring tenosynovectomy. |
- Absolute: Active localized soft tissue infection. - Relative: First-time presentation with mild triggering (Grade I/II). - Relative: Patient unable to participate in post-op early active motion. - Relative: Severe, untreated Complex Regional Pain Syndrome (CRPS). |
| De Quervain Disease | - Failure of conservative management (splinting, NSAIDs, injections). - Persistent, severe pain limiting ADLs and work capacity. - Documented failure to improve after ultrasound-guided injection. - Recurrent disease after previous incomplete surgical release. |
- Absolute: Active localized soft tissue infection. - Relative: Diagnostic ambiguity (e.g., overlapping CMC joint arthritis without clear tenosynovitis). - Relative: Isolated Wartenberg's syndrome (SBRN neuritis) masquerading as de Quervain's. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is essential to optimize surgical outcomes and minimize the risk of catastrophic iatrogenic complications. A critical component of this planning phase is the selection of the appropriate anesthetic modality. Historically, these procedures were performed under general anesthesia or regional blocks with the use of a pneumatic arm tourniquet. However, the modern paradigm has shifted overwhelmingly towards the Wide-Awake Local Anesthesia No Tourniquet (WALANT) technique. WALANT utilizes a tumescent infiltration of local anesthetic (typically 1% lidocaine) combined with epinephrine (1:100,000) and buffered with 8.4% sodium bicarbonate (in a 10:1 ratio) to neutralize the acidic pH of the lidocaine, significantly reducing injection pain.
The use of WALANT provides several profound surgical advantages. First, the epinephrine-induced vasoconstriction provides a virtually bloodless surgical field without the ischemic pain and systemic risks associated with a pneumatic tourniquet. Second, and most importantly, the awake, un-sedated patient can actively flex and extend their digits intraoperatively. This allows the surgeon to dynamically assess the adequacy of the pulley release or compartmental decompression in real-time, completely eliminating the risk of incomplete release and subsequent surgical failure. The surgeon can visually confirm that the Notta nodule glides smoothly through the remaining tendon sheath and that there is no residual catching or subluxation.
Patient positioning is standardized for both procedures. The patient is placed in the supine position with the operative upper extremity extended on a radiolucent hand table. The limb is meticulously prepped and draped in a standard sterile fashion. If the surgeon opts for a traditional approach over WALANT, a well-padded pneumatic tourniquet is applied to the proximal arm. Alternatively, a high forearm Esmarch bandage can be utilized for exsanguination and temporary hemostasis, though this limits the duration of the ischemic window. Proper illumination, preferably with surgical loupe magnification (2.5x to 3.5x), is mandatory to facilitate the precise identification of the delicate neurovascular structures and the pathological retinacular tissues.
Incision Planning and Anatomical Landmarks
Precise incision placement is the foundation of a successful surgical release, ensuring adequate anatomical exposure while mitigating the risk of hypertrophic scarring and flexion contractures. In the hand, incisions must never cross flexion creases perpendicularly, as this predictably leads to scar contracture and functional deficit. For trigger finger release in the middle, ring, and small fingers, a transverse incision measuring approximately 1.5 to 2.0 centimeters is marked several millimeters distal to the distal palmar crease. This placement directly overlies the proximal margin of the A1 pulley. For the index finger, the incision is placed slightly more proximally, several millimeters distal to the proximal palmar crease, reflecting the more proximal location of the index finger's MCP joint.
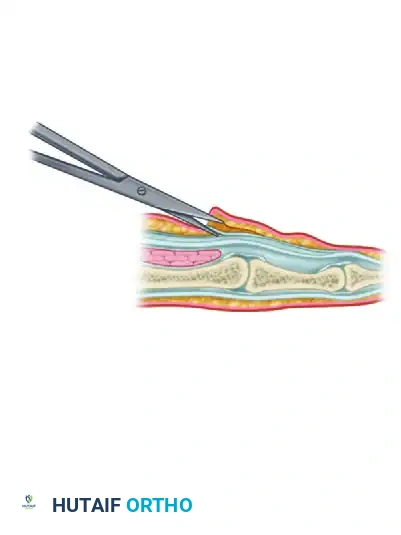
Figure: Standard transverse incision markings for open surgical treatment of trigger finger.
The thumb requires specialized consideration due to its unique kinematics and neurovascular anatomy. Alternative incisions can be utilized, including a transverse incision directly over the MCP flexion crease, or an oblique/longitudinal incision placed precisely between the MCP and distal palmar creases. The critical mandate during thumb incision planning is to anticipate the superficial and obliquely coursing radial digital nerve, which is frequently encountered immediately deep to the dermis in this region.
For de Quervain disease, the incision is planned over the first dorsal compartment. A transverse incision, approximately 2 to 3 centimeters in length, is marked in line with the natural skin creases (Langer's lines) directly over the radial styloid. While a longitudinal incision provides more extensile exposure of the compartment, it is universally associated with a higher incidence of unsightly, hypertrophic scarring and a significantly increased risk of causing a traction injury to the perpendicular branches of the superficial radial nerve. Therefore, the transverse incision remains the gold standard, requiring meticulous, gentle retraction to visualize the proximal and distal extents of the extensor retinaculum.
Step-by-Step Surgical Approach and Fixation Technique
Open Surgical Technique for Trigger Finger (Technique 76-6)
The open surgical release of the A1 pulley remains the highly reliable, gold-standard intervention for trigger digits, offering direct visualization of the pathology and minimizing the risk of collateral damage. Following the administration of WALANT anesthesia and appropriate sterile prep, the planned transverse incision is made through the dermis using a No. 15 scalpel blade. Extreme caution must be exercised to avoid plunging into the subcutaneous tissues, as the digital nerves are located superficially. Dissection through the subcutaneous adipose tissue is performed exclusively using blunt spreading technique with Stevens tenotomy scissors. This blunt dissection sweeps the neurovascular bundles radially and ulnarly, safely isolating them from the midline surgical field.
Once the subcutaneous fat is cleared, small Ragnell or Senn retractors are placed to maintain exposure. The surgeon must then identify the glistening, transversely oriented fibers of the first annular (A1) pulley. A small blunt probe or elevator is used to definitively identify the discrete proximal edge of the A1 pulley, differentiating it from the more proximal palmar fascia. The overlying fascial layers are meticulously cleared to expose the entire length of the A1 pulley. The surgeon must visualize the exact midline of the flexor tendon sheath to ensure the release is centralized, thereby avoiding the eccentric neurovascular bundles.
To execute the release, a small knife blade or the lower blade of a pair of slightly opened, blunt-tipped Stevens tenotomy scissors is introduced just beneath the proximal edge of the A1 pulley. The instrument is gently advanced distally, sharply dividing the transverse fibers of the pulley strictly in the midline. The release is carried distally for approximately 1 centimeter.
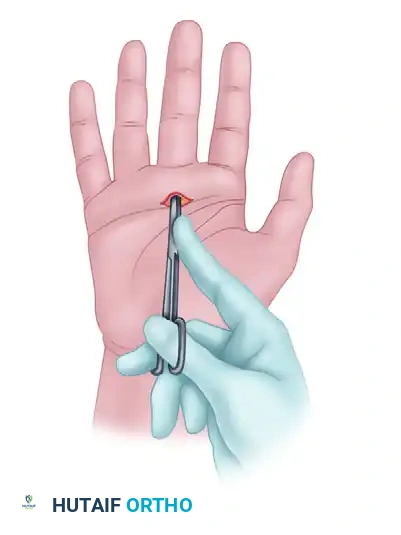
Figure: One blade of scissors has been placed beneath the proximal edge of the tendon sheath, opening the flexor sheath from proximal to distal.
The absolute most crucial step of the procedure follows the anatomical release: the dynamic assessment. The awake patient is instructed to actively flex and extend the digit through a full range of motion. The surgeon directly observes the flexor tendons, ensuring the Notta nodule glides flawlessly without any residual impingement. The surgeon must also carefully inspect the distal extent of the release to ensure the critical A2 pulley remains completely intact.
💡 CLINICAL PEARL: Avoid cutting too far distally. In the fingers, extending the release too far risks disrupting the A2 pulley, leading to catastrophic bowstringing. In the thumb, overzealous distal release risks disrupting the oblique pulley, which is absolutely essential for normal thumb kinematics and pinch strength.
Percutaneous Release Technique for Trigger Finger
Percutaneous release represents a minimally invasive alternative to the open approach, offering the theoretical advantages of reduced scar formation, minimal postoperative pain, and an accelerated return to work. However, this technique is strictly indicated only for the middle and ring fingers. It is generally considered an absolute contraindication in the thumb and index finger due to the extreme proximity of the digital nerves to the midline flexor sheath in these digits, making blind percutaneous release unacceptably hazardous.
The technique relies heavily on precise anatomical landmarks and tactile feedback. The metacarpophalangeal joint of the affected digit is firmly hyperextended by the surgeon. This maneuver serves two critical purposes: it places the A1 pulley under maximal longitudinal tension, making it easier to cut, and it displaces the neurovascular bundles dorsally, moving them away from the percutaneous needle path. A sturdy 18-gauge or 19-gauge needle is selected as the cutting instrument. The needle is inserted strictly in the midline, just distal to the flexor crease, with the bevel oriented longitudinally, perfectly parallel with the underlying flexor tendon fibers.

Figure: Initial percutaneous needle insertion.
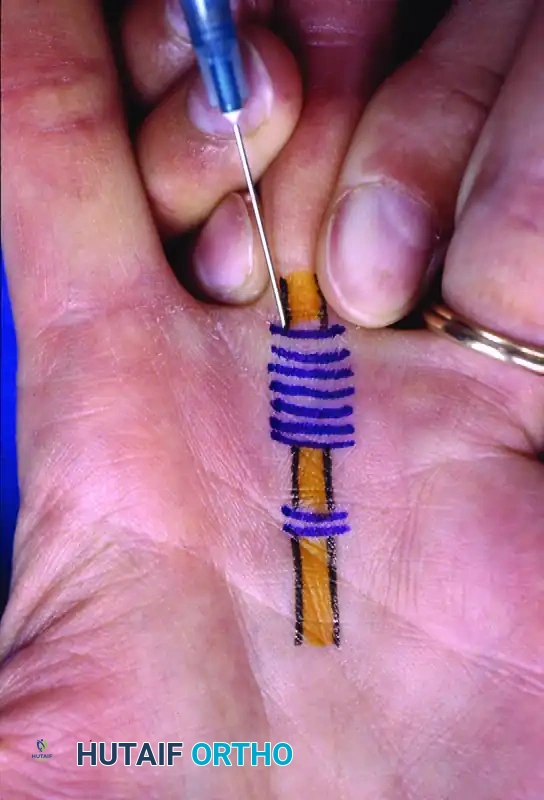
Figure: Percutaneous release of long finger A1 pulley. Metacarpophalangeal joint hyperextended and 19-gauge needle inserted just distal to the flexor crease. Skin markings indicate the path of flexor tendons.
Once the needle tip engages the firm, gritty texture of the A1 pulley, the surgeon stabilizes the needle hub. Using a sweeping, piston-like motion, the sharp bevel of the needle is used to meticulously score and release the pulley fibers from proximal to distal. The surgeon relies entirely on the tactile sensation of the needle cutting through the dense fibrocartilage. A distinct loss of the grating, resistant sensation indicates the complete division of the pulley. Following the release, the patient is again asked to actively flex and extend the digit to confirm the resolution of triggering. If triggering persists, the needle sweeping maneuver is repeated until full, unimpeded excursion is achieved.

Figure: Needle stabilized and pulley released from proximal to distal.
Primary Release and Compartment Reconstruction for De Quervain Disease
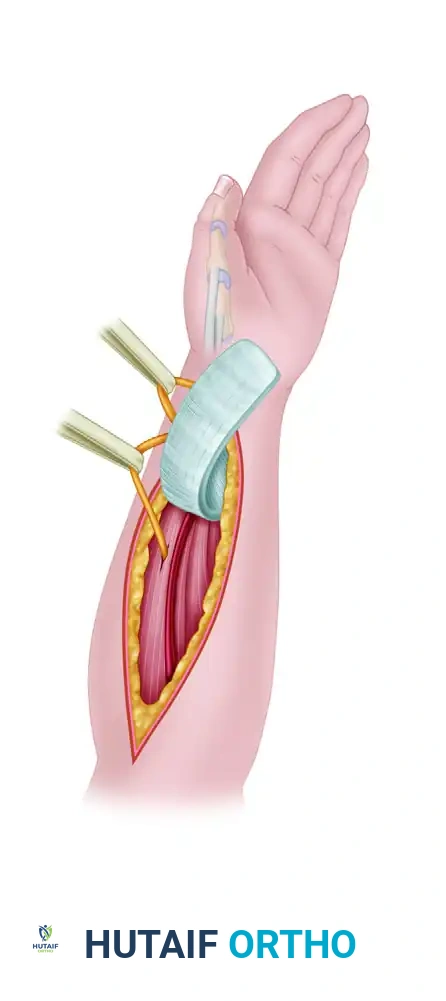
The surgical management of de Quervain disease demands an exacting approach to the first dorsal compartment, prioritizing complete tendon decompression while meticulously preserving the superficial radial nerve and preventing post-operative tendon subluxation. Following the transverse skin incision over the radial styloid, blunt dissection is employed longitudinally to identify the superficial branch of the radial nerve (SBRN). The SBRN branches are highly variable and often intimately associated with the superficial veins. These nerve branches must be rigorously identified, gently mobilized, and protected with small vessel loops or blunt retractors.
Figure: Transverse incision at the level of the first extensor compartment. The superficial radial nerve is identified and rigorously protected.
Once the extensor retinaculum is exposed, the surgeon must plan the retinacular incision. A simple, midline longitudinal division of the retinaculum is strongly discouraged, as it frequently leads to symptomatic volar subluxation of the APL and EPB tendons during active wrist flexion. Instead, the retinacular sheath is incised along its extreme dorsoulnar margin. This highly specific placement leaves a robust volar flap of retinacular tissue, which acts as a mechanical buttress to prevent anterior tendon displacement. The compartment is then fully opened and explored.
Figure: The retinacular sheath is incised. The Extensor pollicis brevis (b) is retracted from the first dorsal compartment. Note the abductor pollicis longus (a).
The critical phase of the operation is the definitive identification of both the APL and EPB tendons and the search for an intracompartmental septum. The surgeon must individually isolate the multiple slips of the APL and the single slip of the EPB. Traction is applied to each tendon independently while observing the thumb to confirm their respective actions (abduction vs. MCP extension). If a longitudinal septum is identified separating the EPB from the APL, it must be completely and sharply excised to ensure profound decompression of the EPB subcompartment. Failure to execute this step guarantees persistent post-operative pain.

Figure: Excision of the intracompartmental septum separating the APL and EPB tendons.
To finalize the procedure and prevent the dreaded
Clinical & Radiographic Imaging Archive