Osteoarthritis of the Wrist: SLAC Management
Key Takeaway
Scapholunate Advanced Collapse (SLAC) is the most common pattern of degenerative wrist osteoarthritis, typically resulting from chronic scapholunate instability. This predictable progression of articular wear spares the radiolunate joint, allowing for motion-preserving salvage procedures. Surgical management depends on the specific stage of degeneration, with options ranging from radial styloidectomy to proximal row carpectomy (PRC) and four-corner arthrodesis, aiming to relieve pain while maintaining functional wrist kinematics.
OSTEOARTHRITIS OF THE WRIST: SCAPHOLUNATE ADVANCED COLLAPSE (SLAC)
Degenerative arthritis developing in the wrist is most frequently characterized by a predictable pattern of articular wear known as Scapholunate Advanced Collapse (SLAC). This condition is intrinsically related to chronic instability around the scaphoid, typically manifesting as a posttraumatic sequela of an untreated or unrecognized scapholunate (SL) interosseous ligament tear.
While primary degenerative changes can occur, the vast majority of SLAC wrists are the end result of altered carpal kinematics. The uncoupling of the scaphoid and lunate disrupts the synchronous motion of the proximal carpal row, leading to abnormal load transmission across the radiocarpal and midcarpal joints. Understanding the pathoanatomy, biomechanics, and progressive staging of this condition is paramount for the orthopaedic surgeon when selecting the appropriate motion-preserving salvage procedure.
Biomechanics and Pathoanatomy
The scaphoid functions as an essential mechanical tie-rod bridging the proximal and distal carpal rows. During normal wrist kinematics, the scaphoid and lunate move synergistically; the scaphoid has a natural tendency to flex, while the triquetrum has a natural tendency to extend. The lunate, intercalated between the two, is balanced by the intact scapholunate and lunatotriquetral ligaments.
When the scapholunate ligament is ruptured, this delicate kinetic balance is destroyed.
1. Scaphoid Flexion: The scaphoid flexes and pronates uninhibitedly.
2. Lunate Extension: The lunate, now tethered only to the triquetrum via the intact lunatotriquetral ligament, falls into extension, creating a Dorsal Intercalated Segment Instability (DISI) deformity.
3. Altered Contact Pressures: The flexed scaphoid shifts its contact area on the elliptical scaphoid fossa of the distal radius. Instead of a broad, congruent surface distributing the load, the proximal pole of the scaphoid point-loads against the dorsal rim of the radius, while the distal pole impinges on the radial styloid.
Clinical Pearl: The radiolunate joint is remarkably preserved in SLAC wrist, even in advanced stages. This is due to the concentric, spherical anatomy of the lunate fossa and the proximal lunate, which maintains a congruent articulation regardless of the lunate's extended posture. This preservation is the foundational biomechanical principle that allows for motion-preserving salvage procedures like proximal row carpectomy (PRC) and four-corner arthrodesis.
Clinical Evaluation
Patients typically present with a history of remote wrist trauma, often dismissed years prior as a "sprain." Chief complaints include insidious onset of dorsal radial wrist pain, progressive loss of motion (particularly extension and radial deviation), and diminished grip strength.
Physical examination often reveals:
* Swelling and synovitis over the dorsal radiocarpal joint.
* Tenderness localized to the anatomic snuffbox and the dorsal scapholunate interval.
* A positive Watson Scaphoid Shift Test: As the wrist is moved from ulnar to radial deviation while applying volar pressure to the scaphoid tuberosity, the unstable scaphoid subluxates dorsally over the dorsal rim of the radius, producing a painful "clunk" upon release.
Radiographic Evaluation and Staging
Standard posteroanterior (PA), lateral, and clenched-fist views are mandatory. Advanced imaging, such as MRI or CT arthrography, may be utilized in early stages to assess ligamentous integrity and cartilage wear, but plain radiography remains the gold standard for staging SLAC wrist.
The progression of osteoarthritis in the SLAC wrist follows a highly predictable, sequential pattern as originally described by Watson.
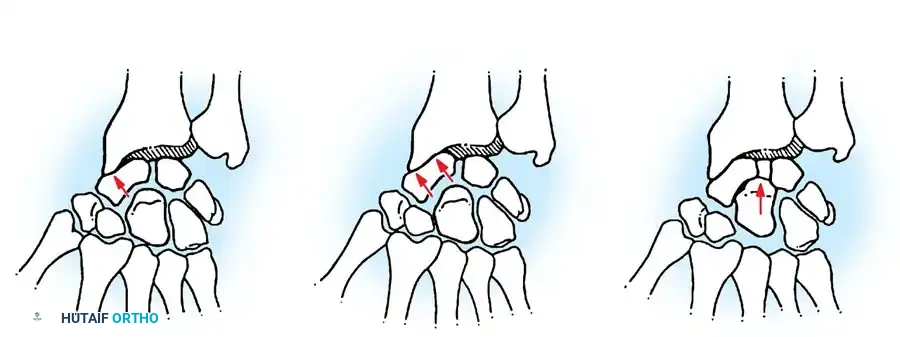
Fig. 66-91 Scapholunate advanced collapse wrist stages I, II, and III. In stage I, changes are limited to the radial styloid. In stage II, the scaphoid fossa is involved. In stage III, the capitolunate joint is additionally narrowed and sclerotic. (From Krakauer JD, Bishop AT, Cooney WP: Surgical treatment of scapholunate advanced collapse, J Hand Surg 19A:751, 1994. Copyright Mayo Clinic.)
- Stage I: Degenerative changes (osteophyte formation, joint space narrowing, sclerosis) are strictly localized to the articulation between the radial styloid and the distal pole of the scaphoid.
- Stage II: Osteoarthritis progresses to involve the entire radioscaphoid articulation (the scaphoid fossa of the distal radius). The radiolunate joint remains completely spared.
- Stage III: The degenerative process advances to the midcarpal joint, specifically the capitolunate articulation. The capitate migrates proximally into the widened scapholunate interval. The radiolunate joint continues to remain preserved.
- Stage IV (Pancarpal): While not part of the original Watson classification, some authors describe a Stage IV involving the radiolunate joint or the entire carpus, usually representing an end-stage pancarpal arthritis that precludes motion-preserving procedures.
Surgical Management and Decision Making
The goal of surgical intervention is to provide a painless, stable wrist while preserving a functional arc of motion and grip strength. The choice of procedure is dictated by the radiographic stage of the disease, the patient's age, occupation, and functional demands.
Stage I Management
For isolated radial styloid impingement, a Radial Styloidectomy (often combined with scaphoid stabilization or denervation) may be indicated.
* Surgical Warning: Resection of the radial styloid must not exceed 3 to 4 mm. Excessive resection will detach the origin of the radioscaphocapitate (RSC) ligament, leading to ulnar translation of the carpus and catastrophic destabilization.
Stage II and III Management
The definitive surgical treatment for advanced SLAC wrist involves excising the pathologic radioscaphoid articulation. As advocated by Watson, Krakauer, Bishop, and Cooney, the two primary motion-preserving procedures are Proximal Row Carpectomy (PRC) and Scaphoid Excision with Four-Corner Arthrodesis.
Historically, limited intercarpal arthrodesis was sometimes augmented with a Silastic (silicone) scaphoid replacement. However, due to the high incidence of particulate wear debris leading to severe "silicone synovitis" and subsequent carpal osteolysis, this practice has been largely abandoned. Modern surgeons prefer the use of biological spacers (such as rolled tendon or fascia) or, more commonly, no spacer at all following scaphoid excision.
Proximal Row Carpectomy (PRC)
PRC involves the en bloc excision of the scaphoid, lunate, and triquetrum, allowing the capitate to articulate directly with the lunate fossa of the distal radius.
Indications:
* Stage II SLAC wrist.
* Absolute Prerequisite: The articular cartilage of the proximal capitate and the lunate fossa of the distal radius must be pristine. If Stage III changes are present (capitolunate arthritis), PRC is contraindicated unless combined with a resurfacing procedure (e.g., capitate resurfacing implant or dorsal capsule interposition), which has variable outcomes.
Surgical Technique (PRC):
1. Positioning: Supine, arm on a hand table, tourniquet applied.
2. Approach: A dorsal longitudinal incision is made centered over the radiocarpal joint. The extensor retinaculum is incised over the third dorsal compartment, and the extensor pollicis longus (EPL) is transposed radially.
3. Capsulotomy: A ligament-sparing dorsal capsulotomy (e.g., Berger's Mayo approach) is performed to expose the proximal carpal row.
4. Bone Excision: Threaded Steinmann pins or a corkscrew are inserted into the scaphoid, lunate, and triquetrum to aid in extraction. The bones are carefully dissected free from their volar ligamentous attachments.
> Pitfall: Extreme care must be taken to preserve the volar radioscaphocapitate (RSC) ligament. Damage to the RSC ligament will result in volar ulnar subluxation of the capitate postoperatively.
5. Closure: The capitate is seated into the lunate fossa. The dorsal capsule is meticulously repaired to prevent dorsal subluxation. The EPL is left transposed in the subcutaneous tissue.
Four-Corner Arthrodesis (Capitate-Hamate-Triquetrum-Lunate Fusion)
For Stage III SLAC wrist, where the capitolunate joint is compromised, a four-corner fusion with scaphoid excision is the procedure of choice. Reports by Wyrick, Stern, Kiefhaber, and Tomaino confirm that this procedure provides excellent pain relief and preserves approximately 50% of normal wrist motion and 70-80% of grip strength.
Indications:
* Stage II or Stage III SLAC wrist.
* High-demand patients (manual laborers) where grip strength preservation is prioritized over maximal range of motion.
Surgical Technique (Four-Corner Fusion):
1. Approach and Exposure: Similar dorsal approach as described for PRC. A posterior interosseous nerve (PIN) neurectomy is routinely performed at the proximal edge of the extensor retinaculum to provide adjunctive pain relief.
2. Scaphoid Excision: The scaphoid is excised piecemeal using a rongeur or en bloc. Excision decompresses the radial side of the wrist and removes the primary source of pain.
3. Joint Preparation: The articular surfaces between the capitate, hamate, lunate, and triquetrum are meticulously decorticated down to bleeding cancellous bone using a high-speed burr or curettes.
> Surgical Warning: Thermal necrosis must be avoided. Copious cold saline irrigation should be used if a high-speed burr is utilized.
4. Reduction and Alignment: The DISI deformity of the lunate must be corrected. A K-wire is used as a joystick to flex the lunate into a neutral position relative to the radius. The capitate is then reduced onto the lunate, restoring the collinear relationship of the radius, lunate, and capitate on the lateral fluoroscopic view.
5. Fixation: Temporary K-wire fixation holds the four bones in compression. Definitive fixation can be achieved via multiple techniques:
* K-wires: Traditional, but requires prolonged casting.
* Headless Compression Screws: Provide excellent compression but can be technically demanding to place without intersecting.
* Circular/Spider Plates: Specifically designed dorsal plates (e.g., locking carpal fusion plates) provide rigid construct stability and allow for early mobilization. The dorsal surfaces of the carpal bones must be flattened to accommodate the plate without causing extensor tendon irritation.
6. Bone Grafting: Cancellous bone graft, harvested from the excised scaphoid (if not sclerotic) or the distal radius (Lister's tubercle), is tightly packed into the interstices of the four-corner fusion mass.
7. Closure: The dorsal capsule is repaired, and the extensor retinaculum is closed over the tendons, leaving the EPL transposed.
Postoperative Protocol and Rehabilitation
For Proximal Row Carpectomy:
* The wrist is immobilized in a bulky dressing and volar splint for 2 to 3 weeks.
* Following splint removal, active and active-assisted range of motion (ROM) exercises are initiated.
* Strengthening begins at 6 weeks. Patients typically achieve their final ROM by 3 to 6 months postoperatively.
For Four-Corner Arthrodesis:
* If rigid internal fixation (dorsal plate) is used, a short-arm cast or rigid splint is applied for 2 to 4 weeks, followed by gentle active ROM.
* If K-wires or less rigid fixation is used, cast immobilization is maintained for 6 to 8 weeks until radiographic evidence of trabecular bridging is observed.
* Heavy lifting and impact loading are restricted until complete radiographic union is confirmed, often taking 10 to 12 weeks.
Complications and Salvage
While both PRC and four-corner fusion are highly successful, complications can occur.
* Nonunion: The most common complication of four-corner fusion, particularly at the capitolunate interface. Smoking is a significant risk factor. Asymptomatic nonunions may be observed; symptomatic nonunions require revision bone grafting and fixation.
* Hardware Impingement: Dorsal plates can cause extensor tendon tenosynovitis or rupture if not adequately countersunk or covered by the dorsal capsule.
* Progressive Osteoarthritis: Following PRC, radiocapitate arthritis can develop over time, though it is often clinically well-tolerated for years.
* Total Wrist Arthrodesis: If motion-preserving procedures fail, or if the patient presents with Stage IV pancarpal arthritis, a total wrist arthrodesis (fusion of the radius to the carpus and third metacarpal) remains the ultimate salvage procedure, providing reliable pain relief at the absolute expense of wrist motion.
You Might Also Like