Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4)

Key Takeaway
Your ultimate guide to Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4) starts here. Top-rated Orthopedic Pediatrics 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
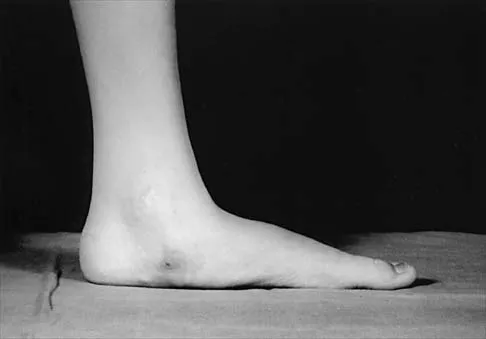
Figure 33 shows the oblique radiograph of an 11-year-old boy who has a mild left flatfoot deformity. Examination reveals that subtalar motion is limited and painful. Despite casting for 6 weeks, the patient reports foot pain that limits participation in sport activities. A CT scan shows no subtalar joint abnormalities. Management should now include
Explanation
Question 2
A nonambulatory verbal 6-year-old child with spastic quadriplegic cerebral palsy has progressive bilateral hip subluxation of more than 50%. There is no pain with range of motion, but abduction is limited to 20 degrees maximum. An AP radiograph is seen in Figure 34. Management should consist of
Explanation
Question 3
Figures 35a through 35c show the clinical photograph and radiographs of a 15-year-old boy who stubbed his toe 1 day ago while walking barefoot in the yard. Management should consist of
Explanation
Question 4
Figure 36 shows the radiograph of a 14-year-old boy who has been treated in the past for Perthes' disease with an abduction brace. He now has hip pain that limits his activity, and nonsteroidal anti-inflammatory drugs have failed to provide relief. What is the most appropriate treatment?
Explanation
Question 5
A newborn girl is referred for evaluation of suspected hip instability. What information from her history would place her in the highest risk category?
Explanation
Question 6
A teenager is undergoing a correction of deformity and lengthening of the femur. Distractions are proceeding as expected; however, during his 6-week follow-up examination, the patient reports that the distraction motors have become harder to turn over for the past 2 to 3 days. Figures 37a and 37b show current radiographs. What is the most likely complication being encountered?
Explanation
Question 7
A 4-year-old child was born with bilateral congenital radial clubhands. Which of the following associated conditions is a contraindication to centralization of the hands on the ulna?
Explanation
Question 8
A 6-year-old Little League pitcher has had pain in the right elbow for the past 2 weeks. Examination reveals mild lateral elbow joint tenderness with full range of motion and no effusion or collateral laxity. A radiograph is shown in Figure 38. Initial management should consist of
Explanation
Question 9
The parents of a 10-year-old boy with Down syndrome are seeking sports clearance for participation in the high jump at the Special Olympics. He is asymptomatic, and the neurologic examination is normal. The hips and patellae are clinically stable. Radiographs of the cervical spine in flexion and extension show a maximum atlanto-dens interval (ADI) of 6 mm. Based on these findings, what recommendation should be made?
Explanation
Question 10
An 18-month-old infant with myelomeningocele and rigid clubfeet has grade 5 quadriceps and hamstring strength, but no muscles are functioning below the knee. What is the best treatment option for the rigid clubfeet?
Explanation
Question 11
Figures 39a and 39b show the current radiographs of an 8-year-old girl who has had pain in the left thigh for the past 3 months. She was recently diagnosed with hypothyroidism and started treatment 1 week ago. Examination reveals a mild abductor deficiency limp on the left side. She lacks 30 degrees internal rotation on the left hip compared with the right hip. Management should consist of
Explanation
Question 12
A 7-year-old boy with spastic diplegia is a limited community ambulator. He has a moderately severe crouched gait. The parents request a treatment that will result in a permanent decrease in lower extremity muscle tone. This is best accomplished with
Explanation
Question 13
Figure 40 shows the radiographs of a 2-year-old boy who has a deformed leg. The patient is ambulatory and has no pain. What is the most appropriate management?
Explanation
Question 14
Where is the most common site for tuberculosis (TB) spondylitis in children?
Explanation
Question 15
Examination of a 13-year-old boy with asymptomatic poor posture reveals increased thoracic kyphosis that is fairly rigid and accentuates during forward bending. The neurologic examination is normal. Spinal radiographs show 10 degrees of scoliosis at Risser stage 2, and there is no evidence of spondylolisthesis. A standing lateral view of the thoracic spine is shown in Figure 41. The kyphosis corrects to 50 degrees. Management should consist of
Explanation
Question 16
What is the most important sign of impending modulation with rapid progression of a spinal deformity in neurofibromatosis?
Explanation
Question 17
A 6-year-old child has a fixed flexion deformity of the interphalangeal (IP) joint of the right thumb. The thumb is morphologically normal, with a nontender palpable nodule at the base of the metacarpophalangeal joint. Clinical photographs are shown in Figures 42a and 42b. Based on these findings, what is the treatment of choice?
Explanation
Question 18
A 3-year-old boy had been treated with serial casting for a right congenital idiopathic clubfoot deformity. The parents are concerned because the child now walks on the lateral border of the right foot. Examination shows that the foot passively achieves a plantigrade position with neutral heel valgus and ankle dorsiflexion to 15 degrees. The forefoot inverts during active ankle dorsiflexion. Mild residual metatarsus adductus is present. Management should now consist of
Explanation
Question 19
Figures 43a and 43b show the clinical photographs of a 4-month-old child with bilateral popliteal pterygium. The fixed knee contractures measure 100 degrees bilaterally. What future treatment is most likely to successfully correct this deformity?
Explanation
Question 20
A 15-year-old boy reports a 2-day history of progressive left buttock pain and severe limping. He denies any history of trauma or radiation of the pain. He has an oral temperature of 100.4 degrees F (38 degrees C). Examination reveals that the lumbar spine and left hip have unguarded motion. The abdomen is nontender. There is moderate tenderness of the left sacroiliac region with no palpable swelling. Pain is elicited when the left lower extremity is placed in the figure-4 position (FABER test). Laboratory studies show a peripheral WBC count of 11,500/mm3 (normal to 10,500/mm3) and an erythrocyte sedimentation rate of 38 mm/h (normal up to 20 mm/h). Radiographs of the pelvis, hips, and lumbar spine are normal. A nucleotide bone scan (posterior view) is shown in Figure 44. Initial management should consist of
Explanation
Question 21
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Explanation
Question 22
What is the preferred treatment of a symptomatic curly toe deformity in a 6-year-old child?
Explanation
Question 23
A 12-year-old girl who is Risser stage 3 has had intermittent mild midback pain for the past 4 weeks. The pain is worse after prolonged sitting and after carrying a heavy backpack at school. She occasionally takes acetaminophen, but the pain does not limit sport activities. Examination reveals a mild right rib prominence during forward bending. Neurologic examination is normal. Radiographs show a 20-degree right thoracic scoliosis with no congenital anomalies or lytic lesions. Management should consist of
Explanation
Question 24
What zone of the physis is widened in rickets?
Explanation
Question 25
A 7-year-old boy has had low back pain for the past 3 weeks. Radiographs reveal apparent disk space narrowing at L4-5. The patient is afebrile. Laboratory studies show a WBC count of 9,000/mm3 and a C-reactive protein level of 10 mg/L. A lumbar MRI scan confirms the loss of disk height at L4-5 and reveals a small perivertebral abscess at that level. To achieve the most rapid improvement and to lessen the chances of recurrence, management should consist of
Explanation
Question 26
A 12-year-old boy with a BMI of 35 presents with a 3-week history of left groin pain and a limp. He is diagnosed with a stable left slipped capital femoral epiphysis (SCFE). Which of the following factors is the strongest indication for prophylactic pinning of the contralateral right hip?
Explanation
Question 27
A 6-year-old girl sustains a severely displaced, extension-type supracondylar humerus fracture. On arrival, the hand is pink and well-perfused but the radial pulse is absent. She is taken to the operating room for closed reduction and percutaneous pinning. Following anatomic reduction and pinning, the radial pulse remains absent, but the hand remains pink with brisk capillary refill. What is the most appropriate next step in management?
Explanation
Question 28
A 6-week-old female infant is treated with a Pavlik harness for a dislocated left hip (Graf type IV). At her 2-week follow-up, the mother reports that the infant is not moving her left leg as much as the right. On examination, the infant lacks active knee extension on the left, but hip and ankle movements are intact. What is the most likely cause of this finding?
Explanation
Question 29
An 8-year-old boy presents with a 2-month history of a painless limp. Radiographs demonstrate sclerosis and fragmentation of the right capital femoral epiphysis. Which of the following radiographic findings at presentation is the most significant indicator of a poor prognosis in Legg-Calvé-Perthes disease?
Explanation
Question 30
In the Ponseti method for the treatment of idiopathic clubfoot, what is the correct sequence of deformity correction?
Explanation
Question 31
A 10-year-old boy complains of a clunking sensation and pain in his lateral right knee. He has no history of trauma. MRI confirms the diagnosis of a symptomatic complete discoid lateral meniscus. There is no meniscal tear. What is the most appropriate surgical treatment?
Explanation
Question 32
A 9-year-old boy sustains a type III tibial spine eminence fracture after a bicycle accident. Radiographs show complete displacement of the avulsed fragment. What is the primary risk of nonoperative management (casting without reduction) for this specific fracture pattern?
Explanation
Question 33
A 3-year-old girl is brought to the emergency department after falling from a slide. Radiographs reveal a closed, isolated, spiral fracture of the middle third of the left femoral shaft. She has no neurovascular deficits and no other injuries. What is the most appropriate definitive management for this patient?
Explanation
Question 34
A 2-year-old girl presents with progressive bilateral bowing of the legs. Radiographs show an abrupt, sharp varus angulation at the proximal tibial metaphysis with a Drennan metaphyseal-diaphyseal angle of 18 degrees. What is the most appropriate initial management?
Explanation
Question 35
A 13-year-old boy presents with recurrent right ankle sprains and a rigid, painful flatfoot. Clinical examination reveals a lack of subtalar motion and peroneal spasticity. Computed tomography confirms a large, osseous talocalcaneal coalition involving the middle facet. The coalition involves approximately 60% of the posterior subtalar joint surface area, and there are moderate osteoarthritic changes in the posterior facet. What is the most appropriate surgical management?
Explanation
Question 36
A 4-year-old girl is brought in by her parents for an abnormal gait and limb length discrepancy. She has no prior orthopedic history. Radiographs show a high dislocated left hip with a false acetabulum and severe acetabular dysplasia.
What is the most appropriate surgical management?

Explanation
Question 37
A 6-year-old boy falls from the monkey bars and sustains a widely displaced Gartland type III supracondylar humerus fracture. On arrival at the emergency department, his hand is pink but the radial pulse is not palpable. Closed reduction and percutaneous pinning are performed. After pinning, the hand remains well-perfused and pink, but the radial pulse is still absent on palpation and Doppler. What is the most appropriate next step in management?
Explanation
Question 38
A 12-year-old obese boy presents with a left chronic stable slipped capital femoral epiphysis (SCFE) and undergoes uncomplicated in situ pinning. Which of the following is the most significant risk factor indicating the need for prophylactic pinning of the contralateral asymptomatic hip?
Explanation
Question 39
An 8-year-old boy with a chronic limp is diagnosed with Legg-Calvé-Perthes disease. Which of the following radiographic findings is considered a 'head at risk' sign according to Catterall, indicating a poor prognosis and a higher risk of femoral head deformation?
Explanation
Question 40
An infant is undergoing serial casting for idiopathic clubfoot using the Ponseti method. After the fifth cast, the midfoot cavus, forefoot adductus, and hindfoot varus have been fully corrected. However, evaluation reveals only 0 degrees of ankle dorsiflexion. What is the most appropriate next step in management?
Explanation
Question 41
A 13-year-old boy presents with severe groin pain after a minor fall. He is completely unable to bear weight, even with crutches. Radiographs confirm a severe slipped capital femoral epiphysis (SCFE).
What is the most devastating complication specific to this type of presentation, and what surgical technique is frequently utilized to minimize its risk?

Explanation
Question 42
A 2-year-old boy with a history of anterolateral bowing of the tibia presents with a new diaphyseal fracture that fails to heal after 3 months of immobilization. Physical examination reveals multiple café-au-lait spots on his trunk.
What is the most likely underlying diagnosis and the optimal surgical strategy for achieving union?

Explanation
Question 43
A 14-year-old girl sustains an ankle injury while playing soccer. Radiographs and a CT scan reveal a Salter-Harris III fracture of the anterolateral distal tibial epiphysis with 4 mm of displacement.
What is the specific pathomechanics of this fracture pattern?
Explanation
Question 44
A 4-year-old girl is evaluated for severe and worsening bilateral bowlegs. Her BMI is in the 98th percentile. Standing radiographs reveal bilateral genu varum with sharp varus angulation at the proximal tibial metaphysis and significant medial metaphyseal beaking (Langenskiöld stage III).
Which of the following is the most definitively appropriate initial management for this patient?

Explanation
Question 45
A 5-year-old boy with spastic quadriplegic cerebral palsy (Gross Motor Function Classification System [GMFCS] level V) is evaluated in the clinic. He is nonambulatory and nonverbal. His mother reports difficulty with perineal care, but there is no apparent pain with passive range of motion.
According to established international hip surveillance guidelines, how frequently should this patient undergo screening AP pelvis radiographs?

Explanation
Question 46
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. Upon initial presentation, he has a pink, pulseless hand. Urgent closed reduction and percutaneous pinning is performed. In the recovery room, the hand remains pink and pulseless with a capillary refill time of less than 2 seconds. What is the most appropriate next step in management?
Explanation
Question 47
A 6-month-old girl presents for follow-up of a dislocated left hip. She had been treated with a Pavlik harness for 6 weeks starting at 1 month of age, which failed to reduce the hip.
What is the next most appropriate step in management?
Explanation
Question 48
An 8-year-old boy presents with a 2-month history of right hip pain and a limp. Radiographs demonstrate fragmentation of the capital femoral epiphysis with lateral subluxation consistent with Legg-Calvé-Perthes disease. Which of the following is considered the most significant prognostic factor for long-term hip outcome in this patient?
Explanation
Question 49
A 12-year-old boy with a BMI of 32 presents with severe left hip pain and inability to bear weight after a minor fall. Radiographs show an acute-on-chronic slipped capital femoral epiphysis (SCFE). During discussion of treatment, prophylactic pinning of the contralateral hip is considered. In which of the following scenarios is prophylactic pinning of the contralateral hip most strongly indicated?
Explanation
Question 50
An 8-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level V) is evaluated for hip surveillance. His migration percentage on an AP pelvis radiograph is 45% bilaterally. He has no pain, but hip abduction is limited to 20 degrees bilaterally. What is the most appropriate management?
Explanation
Question 51
A 2.5-year-old obese boy presents with progressive left-sided genu varum.
Radiographs demonstrate a metaphyseal-diaphyseal angle (MDA) of 18 degrees with early medial metaphyseal beaking. What is the most appropriate initial management?

Explanation
Question 52
A 2-year-old boy who was successfully treated for idiopathic right clubfoot with the Ponseti method presents with a recurrent deformity. Examination shows dynamic supination of the foot during the swing phase of gait and fixed equinus of 10 degrees. The parents report poor compliance with the abduction brace. What is the most appropriate surgical management?
Explanation
Question 53
A 6-year-old boy presents with a 6-month history of a painless snapping sound in his right knee. Examination reveals a palpable clunk at 20 degrees of flexion during extension of the knee. MRI confirms a complete discoid lateral meniscus with no evidence of a meniscal tear. What is the most appropriate management?
Explanation
Question 54
A 14-year-old boy sustains an ankle injury while playing soccer.
Radiographs and a CT scan reveal a displaced Salter-Harris III fracture of the anterolateral distal tibia with a 3 mm articular step-off. Which of the following best describes the pathomechanics of this specific fracture pattern?

Explanation
Question 55
A 13-year-old girl presents with progressive knee pain for 3 months. Radiographs demonstrate a mixed sclerotic and lytic lesion in the distal femoral metaphysis with a 'sunburst' periosteal reaction. Biopsy confirms high-grade osteosarcoma. What is the current standard treatment protocol for this condition?
Explanation
Question 56
A 13-year-old girl presents with left ankle pain and swelling following a twisting injury while playing soccer.
Radiographs reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. What is the primary deforming force and associated anatomical structure responsible for this specific fracture pattern?
Explanation
Question 57
A 6-year-old boy sustains a severe extension-type supracondylar humerus fracture. On initial presentation, his hand is pale and pulseless.
He is immediately taken to the operating room. After successful closed reduction and percutaneous pinning, the hand remains pale and pulseless. A warming blanket is applied and the arm is slightly lowered, but there is no improvement after 15 minutes. What is the most appropriate next step in management?
Explanation
Question 58
An 8-year-old boy presents with a painless limp that has progressively worsened over the past 3 months.
Radiographs confirm Legg-Calvé-Perthes disease in the fragmentation stage. The surgeon classifies the hip using the Herring Lateral Pillar classification. According to this system, which of the following radiographic criteria defines a Lateral Pillar Type B?
Explanation
Question 59
A 12-year-old boy with a BMI in the 99th percentile presents to the emergency department with acute severe left groin pain after a minor slip.
He refuses to bear weight on the left leg, even with the assistance of crutches. Radiographs demonstrate a slipped capital femoral epiphysis (SCFE). According to the Loder classification, this clinical presentation is associated with a significantly increased risk of which of the following complications?
Explanation
Question 60
A 4-year-old boy presents for follow-up of a right idiopathic clubfoot that was treated in infancy with the Ponseti method.
His parents report he walks with a persistent inward turn of the foot. Examination reveals correctable forefoot adductus, a neutral hindfoot, and dynamic supination of the foot during the swing phase of gait. What is the most appropriate next step in management?
Explanation
Question 61
A 2-year-old girl is undergoing an open reduction for developmental dysplasia of the hip (DDH) via a medial approach.
The surgeon encounters several obstacles preventing concentric reduction of the femoral head into the true acetabulum. Which of the following structures is considered an extracapsular obstacle to reduction?

Explanation
Question 62
A 32-month-old, obese boy presents with progressive bilateral bowing of the lower extremities.
Standing radiographs reveal bilateral genu varum, metaphyseal beaking, and an exact metaphyseal-diaphyseal angle of 20 degrees. He is diagnosed with Langenskiöld Stage II infantile Blount disease. What is the most appropriate initial management?

Explanation
Question 63
An 11-year-old boy weighing 65 kg (143 lbs) sustains a length-unstable spiral fracture of the femoral shaft following a fall from a tree.
Which of the following surgical interventions is most appropriate for this patient, optimizing biomechanical stability while minimizing the risk of iatrogenic avascular necrosis (AVN) of the femoral head?

Explanation
Question 64
A 14-year-old male athlete presents with a rigid left flatfoot and a history of frequent ankle sprains. Examination shows marked restriction of subtalar motion and peroneal spasm.
A lateral weight-bearing radiograph displays an unbroken halo of sclerosis corresponding to the C-sign. Which anatomical region is primarily affected by the underlying pathology?
Explanation
Question 65
A 7-year-old child with a known mutation in the COL1A1 gene presents with worsening anterolateral bowing of both femurs and a history of four prior low-energy femoral fractures.
The family requests a durable surgical solution to prevent future fractures and correct the deformity. Which of the following is considered the gold-standard surgical technique for this patient?

Explanation
Question 66
A 15-year-old boy presents with progressive bowing of his left lower extremity, a waddling gait, and medial knee pain. His body mass index is 38. Standing full-length radiographs reveal a severe varus deformity of the proximal tibia, internal tibial torsion, and a procurvatum deformity. The mechanical axis falls medial to the medial compartment of the knee. What is the most appropriate definitive management for this patient?
Explanation
Question 67
A 12-year-old boy is brought to the emergency department unable to bear weight on his right leg after a minor slip. He reports a 4-week history of dull, intermittent right thigh pain prior to the fall. Anteroposterior and frog-leg lateral radiographs demonstrate a severe right slipped capital femoral epiphysis (SCFE). Which of the following approaches is most strongly supported by recent literature to minimize the risk of avascular necrosis (AVN) in this unstable slip?
Explanation
Question 68
A 6-week-old female infant is undergoing treatment with a Pavlik harness for developmental dysplasia of the left hip (DDH). At the routine two-week follow-up, the mother notes that the infant is no longer actively kicking her left leg. On examination, the infant cries with passive movement, lacks active extension of the left knee, but retains normal toe and ankle movements. The patellar reflex is absent on the left. What is the most appropriate next step in management?
Explanation
Question 69
A 6-year-old boy sustains a completely displaced, extension-type supracondylar fracture of the humerus. On initial evaluation, the hand is pink but the radial pulse is absent. He is taken emergently to the operating room, where a closed reduction and percutaneous pinning are successfully performed. Postoperatively, the fracture alignment is excellent, the hand remains warm with a capillary refill of less than 2 seconds, and oxygen saturation on the index finger is 99%; however, the radial pulse remains non-palpable. What is the most appropriate next step in management?
Explanation
Question 70
A 3-year-old boy presents with a relapsed right idiopathic clubfoot. He was initially treated successfully with the Ponseti method, including an Achilles tenotomy. He now walks with a dynamic supination of the foot during the swing phase of gait and has a fixed varus deformity of the hindfoot. Passive correction of the hindfoot is not possible. What is the most appropriate next step in management?
Explanation
Question 71
A 4-year-old girl with spastic quadriplegic cerebral palsy is evaluated in the orthopedic clinic. She is entirely dependent for mobility and utilizes a custom manual wheelchair for transport. She is classified as Gross Motor Function Classification System (GMFCS) Level V. Based on current hip surveillance guidelines, what is her approximate lifetime risk of developing hip displacement (migration percentage >30%), and what is the recommended frequency for radiographic screening?
Explanation
Question 72
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease. Radiographs reveal that he is in the fragmentation stage. According to the Herring Lateral Pillar classification, which of the following radiographic findings places this patient in Lateral Pillar Group C, portending a poorer prognosis?
Explanation
Question 73
A 14-year-old boy presents with vague, deep medial hindfoot pain and a history of multiple ankle sprains. Physical examination reveals a rigid flatfoot with marked limitation of subtalar motion and peroneal spasticity. A lateral radiograph of the ankle demonstrates a continuous bony bridge extending from the posterior aspect of the talus to the calcaneus, creating a continuous 'C-sign'. What is the most likely diagnosis, and what is the best advanced imaging modality to define the pathoa-natomy?
Explanation
Question 74
A 2-year-old girl is referred for anterolateral bowing of her left lower leg. The mother reports a recent minor fall, after which the child refused to bear weight. Radiographs show a fracture through a dysplastic, sclerotic mid-diaphyseal segment of the tibia that has failed to heal after 4 months of casting. This presentation of congenital pseudarthrosis of the tibia (CPT) is most strongly associated with which of the following underlying conditions?
Explanation
Question 75
An 8-year-old boy complains of a painless snapping sensation and intermittent lateral pain in his right knee. Radiographs reveal widening of the lateral joint space, squaring of the lateral femoral condyle, and a cupped appearance of the lateral tibial plateau. MRI demonstrates a complete, intact discoid lateral meniscus with no evidence of a tear. Given his symptomatic presentation, what is the recommended surgical management?
Explanation
Question 76
A 13-year-old boy undergoes in situ pinning of a stable slipped capital femoral epiphysis (SCFE) of the right hip. Six months postoperatively, he presents with worsening right hip pain, a significant limp, and severely restricted range of motion in flexion and abduction. Radiographs demonstrate severe diffuse joint space narrowing, generalized osteopenia around the joint, but no evidence of segmental collapse or sclerosis of the femoral head. What is the most likely diagnosis?
Explanation
Question 77
A 5-year-old boy with spastic quadriplegic cerebral palsy (GMFCS level IV) presents for routine hip surveillance.
His parents report no pain, but the physical examination reveals hip abduction of 20 degrees bilaterally. An AP pelvis radiograph demonstrates a Reimers migration percentage of 45% bilaterally with early acetabular dysplasia. What is the most appropriate management?
Explanation
Question 78
A 12-year-old boy presents with a 6-month history of frequent lateral ankle sprains and deep hindfoot pain exacerbated by sports. Examination reveals a rigid flatfoot with absent subtalar motion and peroneal spasticity.
Lateral radiographs of the foot reveal a distinct 'C-sign'. What is the most likely anatomical location of the primary pathology?
Explanation
Question 79
A 6-year-old girl falls from monkey bars and sustains a completely displaced, extension-type supracondylar fracture of the distal humerus.
During the preoperative evaluation, the hand is pink with palpable pulses, but she is unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured, and what is the typical prognosis?
Explanation
Question 80
A 2-year-old girl is evaluated for a painless limp. Examination demonstrates a positive Galeazzi sign and asymmetric thigh folds. Radiographs reveal a dislocated right hip with a false acetabulum. The surgeon is considering closed reduction and spica casting versus open reduction. Which of the following is an absolute contraindication to closed reduction in this clinical scenario?
Explanation
Question 81
A 3-year-old boy, initially treated with the Ponseti method for idiopathic right clubfoot, presents with a relapse.
His parents report that he walks on the outside border of his right foot. Gait analysis shows dynamic supination of the foot during the swing phase. Passive range of motion indicates the deformity is fully correctable. What is the most appropriate next step in management?
Explanation
Question 82
A 14-year-old boy presents to the emergency department after a twisting injury to his ankle while playing soccer.
Radiographs and a CT scan reveal a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis, displaced by 3 mm. What is the pathomechanical etiology of this specific fracture pattern?
Explanation
Question 83
A 4-year-old boy is brought to the clinic for progressive, severe bilateral leg bowing. Standing radiographs reveal a metaphyseal-diaphyseal angle (MDA) of 20 degrees bilaterally with profound medial physeal beaking (Langenskiöld stage III). He has previously worn KAFO braces for 1 year without improvement. What is the most appropriate management?
Explanation
Question 84
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease.
Which of the following radiographic findings is considered one of Catterall's 'head at risk' signs, indicating a potentially poorer prognosis and an increased likelihood of epiphyseal extrusion?
Explanation
Question 85
A 5-year-old boy sustains a severe, completely displaced extension-type supracondylar fracture of the humerus. On presentation, the hand is pink and warm, but the radial pulse is absent. He has normal capillary refill and intact median, ulnar, and radial nerve motor and sensory function. Following an urgent closed reduction and percutaneous pinning, the hand remains pink and warm, and the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 86
A 3-year-old child who was successfully treated with the Ponseti method for idiopathic clubfoot now presents with dynamic supination of the foot during the swing phase of gait. On examination, the foot is fully correctable passively with no fixed structural deformity. What is the most appropriate next step in management?
Explanation
Question 87
A 6-month-old infant with developmental dysplasia of the hip (DDH) was treated with a Pavlik harness starting at age 4 weeks. After 4 weeks of harness wear, the hip remained dislocated, and the harness was discontinued. Currently, ultrasound confirms persistent dislocation. What is the most appropriate next step in management?
Explanation
Question 88
A 14-year-old boy with spastic diplegic cerebral palsy presents with severe crouch gait. Physical examination reveals a popliteal angle of 80 degrees, knee flexion contractures of 15 degrees bilaterally, and severe planovalgus foot deformities. Radiographs demonstrate patella alta. Which of the following combinations of surgical procedures is most appropriate to address his knee pathology?
Explanation
Question 89
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. On initial examination, the hand is pink, but the radial pulse is absent. He is taken to the operating room for closed reduction and percutaneous pinning. Post-reduction, the hand remains pink and warm with a capillary refill of less than 2 seconds, but the radial pulse remains unpalpable. Doppler ultrasound confirms flow in the palmar arch. What is the most appropriate next step?
Explanation
Question 90
A 2.5-year-old girl is evaluated for bilateral bowlegs. Her BMI is in the 95th percentile. Radiographs reveal a metaphyseal-diaphyseal angle (Drennan's angle) of 18 degrees on the right and 19 degrees on the left. There is prominent medial metaphyseal beaking. What is the most appropriate initial management?
Explanation
Question 91
A 12-year-old boy with a BMI of 32 presents with knee pain. He walks with a limp and his foot is externally rotated. Examination shows obligatory external rotation with hip flexion. AP and frog-leg lateral radiographs of the pelvis show a mild left slipped capital femoral epiphysis (SCFE) and a normal right hip. What is the most appropriate management?
Explanation
Question 92
A 7-year-old girl with Down syndrome wishes to participate in Special Olympics gymnastics. She is completely asymptomatic, has no history of neck pain or weakness, and her neurologic examination is normal. Based on the American Academy of Pediatrics (AAP) guidelines, what is the recommendation regarding pre-participation cervical spine screening?
Explanation
Question 93
A 14-year-old girl sustains an ankle injury. Radiographs show a Salter-Harris III fracture of the anterolateral aspect of the distal tibial epiphysis. Which structure is responsible for the avulsion of this fracture fragment?
Explanation
Question 94
A 6-month-old infant is evaluated for frequent fractures and is found to have blue sclerae and dentinogenesis imperfecta. A diagnosis of osteogenesis imperfecta is made. This condition is primarily associated with a defect in the synthesis of which of the following?
Explanation
Question 95
An 8-year-old boy presents with a limp. Radiographs confirm Legg-Calvé-Perthes disease with fragmentation of the femoral head and more than 50% collapse of the lateral pillar. According to the Herring lateral pillar classification, which of the following best describes his prognosis and indicated management?
Explanation
Question 96
An 11-year-old obese boy presents with right hip pain and a limp. Radiographs confirm a unilateral right slipped capital femoral epiphysis (SCFE), which is treated with in situ single-screw fixation. The parents ask about the risk of the left hip developing the same condition. Which of the following radiographic findings is the strongest predictor for a subsequent contralateral slip and most justifies prophylactic pinning of the asymptomatic left hip?
Explanation
Question 97
A 6-year-old girl is brought to the emergency department after falling from monkey bars. She sustains a severely displaced Gartland type III supracondylar humerus fracture. On initial examination, her hand is pink and well-perfused, but the radial pulse is absent. She is taken to the operating room for urgent closed reduction and percutaneous pinning. Following stable anatomic reduction and pinning, the hand remains pink with brisk capillary refill (< 2 seconds), but the radial pulse remains nonpalpable by Doppler. What is the most appropriate next step in management?
Explanation
Question 98
A 5-week-old infant is being treated with a Pavlik harness for developmental dysplasia of the left hip. During the 2-week follow-up visit, the parents report that the infant has stopped kicking the left leg. On physical examination, the infant exhibits an absence of active knee extension on the left side, though hip flexion and ankle movements are preserved. Ultrasound confirms the hip is well-reduced. What is the most appropriate management of this complication?
Explanation
Question 99
A 17-year-old non-ambulatory male (GMFCS Level V) with spastic quadriplegic cerebral palsy presents with severe right hip pain that interferes with seating, perineal care, and sleep. Radiographs demonstrate a chronically dislocated right hip with severe degenerative changes and a deformed femoral head. He has failed extensive non-operative management, including optimizing medical therapy and seating modifications. Which of the following surgical interventions is most appropriate to alleviate his pain and improve nursing care?
Explanation
Question 100
An 9-year-old boy presents with a 5-month history of a painless limp and right hip stiffness. Radiographs demonstrate Legg-Calvé-Perthes disease in the fragmentation stage.
Which of the following factors is the most reliable predictor of a poor long-term radiographic and clinical outcome, often necessitating surgical containment?
Explanation
None
