Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 2)
Key Takeaway
Looking for accurate information on Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 2)? Top-rated Orthopedic Pediatrics 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 2)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The parents of a 15-month-old child report that he is not yet walking. Further evaluation, rather than reassurance and observation, should be conducted if the child is not performing what other activity?
Explanation
Question 2
Of the following clinical situations, which is most likely to lead to osteonecrosis associated with a slipped capital femoral epiphysis (SCFE)?
Explanation
Question 3
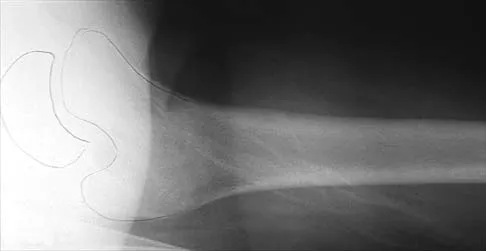
An 8-year-old boy has had pain and swelling around the right knee for the past 4 weeks. He recalls bumping it about 4 weeks ago. He has no pain in other joints, and denies any fevers, chills, or other symptoms. A radiograph is shown in Figure 13. Laboratory studies show a WBC count of 9,700/mm3, an erythrocyte sedimentation rate of 18 mm/h, and a C-reactive protein level of 3.7 mg/L. What is the next most appropriate step in management?
Explanation
Question 4
A 2-year-old child is being evaluated for limb-length and girth discrepancy. As a newborn, the patient was large for gestational age and had hypoglycemia. Current examination shows enlargement of the entire right side of the body, including the right lower extremity and foot. The skin shows no abnormal markings, and the neurologic examination is normal. The spine appears normal. Radiographs confirm a 2-cm discrepancy in the lengths of the lower extremities. Additional imaging studies should include
Explanation
Question 5
A 12 1/2-year-old boy reports intermittent knee pain and limping that interferes with his ability to participate in sports. He actively participates in football, basketball, and baseball. He denies any history of injury. Examination shows full range of motion without effusion. Radiographs reveal an osteochondritis dissecans (OCD) lesion on the lateral aspect of the medial femoral condyle. MRI scans are shown in Figures 14a and 14b. Initial treatment should consist of
Explanation
Question 6
A 14-year-old boy undergoes application of a circular frame with tibial and fibular osteotomy for gradual limb lengthening. He initiates lengthening 7 days after surgery. During the first week of lengthening, he reports that turning of the distraction devices is becoming increasingly difficult. On the 9th day of lengthening, he is seen in the emergency department after feeling a pop in his leg and noting the acute onset of severe pain. What complication has most likely occurred?
Explanation
Question 7
What is the most common primary malignant bone or cartilage tumor in children?
Explanation
Question 8
What is the peak period of onset in children with pauciarticular juvenile rheumatoid arthritis?
Explanation
Question 9
A 10-year-old girl who is Risser stage 0 has back deformity associated with neurofibromatosis type 1 (NF1). She has no back pain. Examination shows multiple cafe-au-lait nevi with normal lower extremity neurologic function and reflexes. Standing radiographs of the spine show a short 50-degree right thoracic scoliosis with a kyphotic deformity of 55 degrees (apex T8). A 10-degree progression in scoliosis has occurred during the past 1 year. There is no cervical deformity. MRI shows mild dural ectasia, primarily in the upper lumbar region. Management should consist of
Explanation
Question 10
In obstetrical brachial plexus palsy, which of the following signs is associated with the poorest prognosis for recovery in a 2-month-old infant?
Explanation
Question 11
A 6-year-old boy with acute hematogenous osteomyelitis of the distal femur is being treated with intravenous antibiotics. The most expeditious method to determine the early success or failure of treatment is by serial evaluations of which of the following studies?
Explanation
Question 12
A 6-year-old girl has a painless spinal deformity. Examination reveals 2+ and equal knee jerks and ankle jerks, negative clonus, and a negative Babinski. The straight leg raising test is negative. Abdominal reflexes are asymmetrical. PA and lateral radiographs are shown in Figures 15a and 15b. What is the next most appropriate step in management?
Explanation
Question 13
Figure 16 shows the radiograph of a 7-year-old boy who sustained a pathologic fracture of the left humerus 1 day ago. Initial management should consist of
Explanation
Question 14
Figure 17 shows the AP radiograph of a 5-year old child who has mild short stature and a painless bilateral gluteus medius lurch. Initial work-up should include
Explanation
Question 15
A 7-year-old girl with spinal muscular atrophy (SMA) type II has popping of the left hip. Examination reveals painless subluxation of the joint in adduction with palpable reduction in abduction. Radiographs show coxa valga, subluxation of the left hip, and pelvic obliquity with elevation of the left hemipelvis. Treatment should consist of
Explanation
Question 16
A newborn with myelomeningocele has no movement below the waist and has bilateral hips that dislocate with provocative flexion and adduction. What is the best treatment option for the hip instability?
Explanation
Question 17
A 14-year-old boy reports a 4-month history of increasing backache with difficulty walking long distances. His parents state that he walks with his knees slightly flexed and is unable to bend forward and get his hands to his knees. He denies numbness, tingling, and weakness in his legs and denies loss of bladder and bowel control. A lateral radiograph of the lumbosacral spine is shown in Figure 18. What is the best surgical management for this condition?
Explanation
Question 18
Duchenne's muscular dystrophy is a genetic disorder that is transmitted by which of the following modes of inheritance?
Explanation
Question 19
A 4-month-old infant is referred for evaluation of congenital scoliosis. The child has no congenital heart anomalies, and a renal ultrasound shows that he has one kidney. Examination reveals mild scoliosis and a large hairy patch on the child's back. Neurologic evaluation is normal for his age. A clinical photograph and radiograph are shown in Figures 19a and 19b. Initial management should consist of
Explanation
Question 20
A 12-year-old boy reports limping and chronic knee pain that is now inhibiting his ability to participate in sports. Clinical examination and radiographs of the knee are normal. Additional evaluation should include
Explanation
Question 21
In children with moderate to severe osteogenesis imperfecta (OI), intravenous pamidronate therapy has been shown to increase the thickness of cortical bone. This occurs primarily as a consequence of
Explanation
Question 22
Split posterior tibial tendon transfer is used in the treatment of children with cerebral palsy. Which of the following patients is considered the most appropriate candidate for this procedure?
Explanation
Question 23
Late surgical treatment of posttraumatic cubitus varus (gunstock deformity) is usually necessitated by the patient reporting problems related to
Explanation
Question 24
An 11-year-old boy sustained an ankle injury while playing football. Figure 20 shows an AP radiograph obtained the day of injury. Treatment should consist of
Explanation
Question 25
A 3-year-old child has bilateral genu varum and short stature. Radiographs show physeal widening and generalized osteopenia. The femora and tibiae show anterolateral bowing. Laboratory studies show low normal serum calcium values, significantly decreased serum phosphate levels, and normal parathyroid hormone (PTH), alkaline phosphatase, and vitamin-D levels. These findings are consistent with
Explanation
Question 26
A 6-year-old boy falls from the monkey bars and presents with a severely displaced extension-type supracondylar humerus fracture. On examination in the emergency department, his hand is pink, but the radial pulse is not palpable. He is taken to the operating room, where closed reduction and percutaneous pinning are performed. Postoperatively, the hand remains pink and well-perfused, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 27
A 6-week-old female infant is being treated with a Pavlik harness for an easily reducible dislocated left hip. At her 2-week follow-up appointment, the parents report that she is no longer kicking her left leg as much as her right. On physical examination, she demonstrates decreased active knee extension on the left, though she does not appear to be in pain. What is the most likely cause of this clinical finding?
Explanation
Question 28
A 13-year-old obese male presents to the emergency department after a minor slip. He is unable to bear weight on his right leg, even with crutches. Radiographs reveal a severe slipped capital femoral epiphysis (SCFE). Which of the following interventions during surgical treatment has been shown to potentially decrease the risk of osteonecrosis in this specific clinical scenario?
Explanation
Question 29
A 4-year-old boy who was treated successfully for idiopathic clubfoot during infancy with the Ponseti method presents with a dynamic supination deformity of the foot during the swing phase of gait. On examination, his ankle passive dorsiflexion is 15 degrees past neutral with the knee extended, and the foot is completely flexible. What is the most appropriate management for this patient?
Explanation
Question 30
An 8-year-old boy is diagnosed with Legg-Calve-Perthes disease. Anteroposterior pelvic radiographs demonstrate sclerosis and fragmentation of the left capital femoral epiphysis. According to the Herring lateral pillar classification, which of the following radiographic findings indicates a Group C classification, which is associated with the poorest prognosis?
Explanation
Question 31
A 14-year-old boy twists his ankle while playing basketball. Radiographs demonstrate a Salter-Harris type III fracture of the anterolateral distal tibial epiphysis. What is the primary mechanism and deforming force responsible for this specific fracture pattern?
Explanation
Question 32
A 5-year-old boy with a history of multiple low-energy fractures, blue sclerae, and dentinogenesis imperfecta is being evaluated for surgical intervention of a severely bowed femur. He receives intravenous bisphosphonate therapy every 3 months. What is the primary mechanism of action of bisphosphonates in this condition?
Explanation
Question 33
A 6-year-old girl with spastic quadriplegic cerebral palsy, GMFCS level V, undergoes routine hip surveillance. Anteroposterior pelvic radiographs reveal a migration percentage (Reimers' index) of 45% in the right hip. She experiences minimal pain, but hip abduction is limited to 15 degrees bilaterally. What is the most appropriate next step in surgical management?
Explanation
Question 34
A 12-year-old boy presents with a history of recurrent ankle sprains and a painful, rigid flatfoot. On examination, subtalar motion is severely restricted, and there is palpable spasm of the peroneal muscles. Oblique radiographs of the foot demonstrate an 'anteater nose' sign. Which of the following is the most likely diagnosis?
Explanation
Question 35
A 3-year-old girl is diagnosed with infantile idiopathic scoliosis. Radiographs reveal a primary left thoracic curve of 35 degrees. The rib-vertebra angle difference (RVAD) of Mehta is measured at 25 degrees. What is the most appropriate initial management for this patient to control deformity progression?
Explanation
Question 36
A 3-year-old girl is diagnosed with a neglected developmental dysplasia of the left hip. Radiographs show a high dislocation of the femoral head. What is the standard surgical management for this patient?
Explanation
Question 37
A 2-year-old boy who was treated for idiopathic clubfoot with the Ponseti method presents with recurrent equinovarus deformity. What is the most common cause of relapse in this clinical scenario?
Explanation
Question 38
A 14-year-old boy is evaluated for hip pain and severe stiffness 6 months after undergoing in situ pinning for a stable slipped capital femoral epiphysis (SCFE) of the right hip. On examination, he has globally restricted range of motion of the right hip. Radiographs reveal narrowing of the joint space to less than 3 mm, osteopenia, and no evidence of hardware penetration into the joint. What is the most likely diagnosis?
Explanation
Question 39
A 6-year-old boy sustains a completely displaced extension-type supracondylar fracture of the humerus. On physical examination in the emergency department, the patient is unable to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which of the following nerves is most likely injured?
Explanation
Question 40
An 8-year-old boy presents with a painless limp of 3 months' duration. Radiographs show fragmentation of the femoral head consistent with Legg-Calvé-Perthes disease. According to the Herring Lateral Pillar classification, which of the following radiographic findings portends the worst prognosis?
Explanation
Question 41
A 2.5-year-old girl is brought in by her parents for evaluation of bowing of her legs. On standing full-length radiographs, the metaphyseal-diaphyseal angle (Drennan's angle) is measured at 18 degrees bilaterally. What is the most appropriate next step in management?
Explanation
Question 42
A 4-year-old boy with a history of multiple low-energy long bone fractures, blue sclerae, and dentinogenesis imperfecta is evaluated. A genetic disorder is suspected. The pathophysiology of this condition is primarily related to a defect in the synthesis of which of the following?
Explanation
Question 43
A 4-year-old boy who weighs 18 kg (40 lbs) sustains an isolated, closed, length-stable, spiral fracture of the mid-diaphyseal femur after a fall from a playground structure. What is the most appropriate definitive management?
Explanation
Question 44
A 14-year-old girl sustains an ankle injury while playing soccer. Radiographs reveal a Salter-Harris III fracture of the anterolateral distal tibial epiphysis. The mechanism of injury involves avulsion by which of the following structures?
Explanation
Question 45
A 13-year-old boy with a BMI of 35 presents to the emergency department unable to bear weight on his left leg after a minor slip. Radiographs confirm an acute, severe left slipped capital femoral epiphysis (SCFE). He cannot bear weight even with crutches. What is the current consensus regarding surgical treatment for this patient to minimize complications?
Explanation
Question 46
A 4-year-old boy who was successfully treated for bilateral idiopathic clubfeet as an infant using the Ponseti method presents with returning deformity in the right foot. During the swing phase of gait, the right foot supinates dynamically. Passive range of motion demonstrates fully correctable deformities without residual equinus. What is the most appropriate next step in surgical management?
Explanation
Question 47
A 9-year-old boy weighing 55 kg (121 lbs) sustains a closed, length-unstable, midshaft femur fracture. Among the following options, which surgical intervention carries the highest risk of complication, specifically loss of reduction and malunion, in this specific patient?
Explanation
Question 48
A 6-week-old female is being treated with a Pavlik harness for a developmental dysplasia of the hip (DDH) that was dislocated but reducible on exam. At her 1-week follow-up, the parents report she has stopped kicking her left leg. On clinical examination, she holds the left knee in extension and does not actively contract her quadriceps with tickling. Ultrasound confirms the hip is currently reduced. What is the most appropriate next step in management?
Explanation
Question 49
A 7-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level IV) presents with a slowly progressing scissoring gait, pain with diaper changes, and difficulty sitting in his wheelchair. A recent AP pelvis radiograph demonstrates a right hip Reimers migration percentage of 55%. The acetabulum is dysplastic, but there is no evidence of degenerative arthritis. What is the most appropriate definitive management?
Explanation
Question 50
A 13-year-old boy with a BMI in the 99th percentile presents to the emergency department with acute left groin pain. He states he twisted his leg getting out of bed. On examination, he is completely unable to bear weight on the left leg, even with the use of crutches. Radiographs demonstrate a severe posterior and inferior displacement of the left capital femoral epiphysis. According to the Loder classification, his inability to bear weight puts him at highest risk for which of the following complications?
Explanation
Question 51
A 6-year-old girl falls from monkey bars and sustains a widely displaced, extension-type supracondylar humerus fracture. On initial presentation, she has no palpable radial pulse, but the hand is warm, pink, and has a brisk capillary refill of less than 2 seconds. She is taken urgently to the operating room, where an anatomic closed reduction is achieved and stabilized with three divergent lateral pins. After pinning, the hand remains pink and warm, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 52
An 8-year-old boy presents with a 4-month history of a painless limp. Radiographs demonstrate fragmentation and sclerosis of the left proximal femoral epiphysis consistent with Legg-Calvé-Perthes disease. The lateral one-third of the femoral head exhibits a 60% loss of height compared to the contralateral normal hip. According to the Herring lateral pillar classification, what is his expected prognosis without surgical intervention?
Explanation
Question 53
A 14-year-old boy presents with chronic, vague lateral foot pain and a history of multiple ankle sprains. On physical examination, he has a rigid pes planovalgus deformity with absent subtalar motion. A lateral radiograph of the foot demonstrates an elongated anterior process of the calcaneus projecting toward the navicular. To properly characterize this anatomy prior to surgical intervention, what is the best diagnostic imaging modality?
Explanation
Question 54
A 12-year-old female presents to the clinic with an adolescent idiopathic scoliosis (AIS) right thoracic curve of 28 degrees. When counseling her parents about the risk of curve progression, you explain the concept of peak height velocity (PHV). Which of the following maturity indicators most closely corresponds to the peak velocity of growth in a patient with AIS?
Explanation
Question 55
A 4-year-old girl whose weight is above the 95th percentile presents with a waddling gait and progressive bowing of both legs. Standing long-leg radiographs show medial metaphyseal beaking of the proximal tibiae and a metaphyseal-diaphyseal angle of 18 degrees. What physiological principle best explains the progression of her proximal medial tibial physeal deformity?
Explanation
Question 56
A 3-month-old infant with developmental dysplasia of the hip (DDH) is being treated with a Pavlik harness. During a follow-up visit, the parents report that the infant is not moving the right leg as much as the left. On physical examination, the right knee is held in extension, and the patellar reflex is absent on the right side. What is the most likely cause of this clinical finding?
Explanation
Question 57
A 12-year-old boy presents with right hip pain and an antalgic gait. He is diagnosed with a severe right slipped capital femoral epiphysis (SCFE). His weight is greater than the 95th percentile for his age. You plan to perform in situ pinning of the right hip. Which of the following is considered the strongest indication for prophylactic pinning of the contralateral asymptomatic hip?
Explanation
Question 58
A 3-year-old girl is evaluated for progressive bowing of both lower extremities. She is at the 95th percentile for weight. Standing long-leg radiographs show significant genu varum with a metaphyseal-diaphyseal angle (Drennan angle) of 18 degrees bilaterally, as well as prominent medial metaphyseal beaking. What is the most appropriate initial management for this patient?
Explanation
Question 59
A 6-year-old boy falls from the monkey bars and sustains a widely displaced, extension-type supracondylar humerus fracture. On presentation to the emergency department, his hand is pink and warm with brisk capillary refill, but the radial pulse is absent. Neurological examination reveals weakness in flexing the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. What is the most appropriate next step in management?
Explanation
Question 60
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease (LCPD). While evaluating his plain radiographs, you are assessing the "head-at-risk" signs described by Catterall, which are indicative of a poorer prognosis. Which of the following radiographic findings represents a Catterall "head-at-risk" sign?
Explanation
Question 61
A 2-week-old infant is undergoing serial casting for a severe right idiopathic clubfoot using the Ponseti method. After 5 weeks of weekly cast changes, the cavus, adductus, and varus deformities have been fully corrected, but there is residual equinus of 15 degrees. What is the most appropriate next step in management?
Explanation
Question 62
A 2-year-old child with a known diagnosis of neurofibromatosis type 1 (NF1) presents with anterolateral bowing of the tibia that has progressed to a complete fracture. Radiographs confirm congenital pseudarthrosis of the tibia (CPT). Which of the following biological adjuncts is most strongly supported in the surgical management of this condition to improve bone union rates?
Explanation
Question 63
A 14-year-old female gymnast complains of lower back pain that worsens with extension and twisting movements. Physical examination reveals tight hamstrings and pain elicited on the single-leg hyperextension test (Stork test). Standing AP and lateral radiographs of the lumbar spine show no distinct abnormalities. If advanced imaging is to be ordered to confirm an acute pars interarticularis stress reaction, which imaging modality is highly sensitive and best avoids ionizing radiation?
Explanation
Question 64
A 6-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level V) is undergoing routine orthopedic surveillance. According to established hip surveillance guidelines for children with cerebral palsy, which of the following radiographic measurements is the most critical parameter to track for evaluating the risk and progression of hip displacement?
Explanation
Question 65
A 13-year-old boy presents with a 6-month history of frequent ankle sprains, difficulty running, and lateral foot pain. On physical examination, he has a rigid flatfoot with marked restriction of subtalar motion, and the peroneal tendons appear spastic. A lateral radiograph of the foot reveals a distinct "C-sign". Which of the following is the most likely primary diagnosis, and what is the best initial advanced imaging modality to clearly delineate the extent of the pathology for preoperative planning?
Explanation
Question 66
A 12-year-old boy who is at the 99th percentile for BMI presents with right thigh pain and an antalgic gait. Radiographs confirm a mild right slipped capital femoral epiphysis (SCFE). Which of the following is the most reliable radiographic predictor that this patient will subsequently develop a contralateral SCFE?
Explanation
Question 67
A 4-year-old boy, successfully treated for an idiopathic left clubfoot as an infant using the Ponseti method, presents with recurrence. On physical examination, the foot is plantigrade at rest, but he exhibits dynamic supination during the swing phase of gait. Passive range of motion is full, and the heel easily rests in a neutral position. What is the most appropriate management for this patient?
Explanation
Question 68
A 6-year-old girl sustains a severely displaced, extension-type supracondylar humerus fracture. On initial presentation in the emergency department, her hand is pale and pulseless. Following urgent closed reduction and percutaneous pinning in the operating room, the fracture is anatomically aligned, but the hand remains pale, cold, and pulseless after 15 minutes of observation. What is the next most appropriate step in management?
Explanation
Question 69
A 7-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level V) is evaluated in the clinic. He is non-ambulatory. Pelvic radiographs demonstrate a Reimers Migration Percentage of 55% on the right and 45% on the left, with an intact Shenton's line and minimal degenerative changes. On physical exam, his hips can be abducted to 30 degrees bilaterally. What is the most appropriate surgical intervention?
Explanation
Question 70
A 9-year-old boy presents with an 8-month history of a painless limp. Radiographs reveal fragmentation of the left femoral head. According to the Herring lateral pillar classification, the hip is categorized as Type B. Range of motion is well preserved. Based on current evidence, which of the following treatments provides the best long-term radiographic outcome for this patient?
Explanation
Question 71
A 15-year-old severely obese male presents with worsening bilateral bowing of his legs. Standing radiographs reveal severe varus, procurvatum, and internal rotation deformities. The medial proximal tibial physes appear to be prematurely closed, and the mechanical axis passes entirely medial to the knee joints. Which of the following is the most appropriate definitive management?
Explanation
Question 72
A 24-month-old girl presents with a waddling gait. An anteroposterior radiograph of the pelvis demonstrates a completely dislocated left hip. The acetabular index on the left is 42 degrees, compared to 20 degrees on the right. She has not had any prior treatment. What is the most appropriate management strategy?
Explanation
Question 73
A 13-year-old boy presents with a history of recurrent ankle sprains and an increasingly rigid, painful right flatfoot. Peroneal spasm is noted on physical examination. A lateral radiograph of the foot demonstrates a continuous osseous bridge connecting the talar dome to the sustentaculum tali (the 'C-sign'). What is the initial treatment of choice for this condition?
Explanation
Question 74
A 14-year-old girl sustains an inversion injury to her right ankle while playing soccer. Radiographs demonstrate an isolated Salter-Harris type III fracture of the anterolateral aspect of the distal tibial epiphysis. The mechanism of this specific fracture pattern is primarily due to avulsion by which of the following ligamentous structures?
Explanation
Question 75
A 13-year-old obese male presents with a 1-day history of extreme left groin pain following a minor fall. He is completely unable to bear weight on the left leg, even with the assistance of crutches. Radiographs reveal a severe left slipped capital femoral epiphysis (SCFE). He is scheduled for urgent surgical stabilization. Which of the following surgical steps is associated with the highest increased risk of postoperative avascular necrosis (AVN) in this patient?
Explanation
Question 76
A 6-year-old child with spastic quadriplegic cerebral palsy (GMFCS level V) presents for routine follow-up. An AP pelvis radiograph demonstrates a migration percentage of 48% bilaterally. What is the most appropriate management?
Explanation
Question 77
A 5-year-old girl sustains a severely displaced extension-type supracondylar humerus fracture. On arrival in the emergency department, her hand is pink and well-perfused, but the radial pulse is not palpable. After prompt closed reduction and percutaneous pinning in the operating room, the hand remains pink and warm with a capillary refill of less than 2 seconds, but the pulse remains non-palpable. What is the next most appropriate step?
Explanation
Question 78
A 6-week-old female infant is diagnosed with a completely dislocated but reducible left hip (Developmental Dysplasia of the Hip). She is placed in a Pavlik harness. At the 3-week follow-up ultrasound, the left hip remains dislocated within the harness. What is the next best step in management?
Explanation
Question 79
A 12-year-old obese boy presents with left groin and knee pain for 2 months. Radiographs confirm a mild, stable slipped capital femoral epiphysis (SCFE) on the left. In which of the following scenarios is prophylactic percutaneous pinning of the contralateral (asymptomatic) right hip most strongly indicated?
Explanation
Question 80
A 7-year-old boy presents with a painless limp of 3 months' duration. Radiographs show sclerosis, fragmentation, and lateral displacement of the right capital femoral epiphysis, consistent with Legg-Calvé-Perthes disease. Which of the following radiographic findings represents one of Catterall's 'head-at-risk' signs, indicating a poorer prognosis?
Explanation
Question 81
A 2-week-old infant with idiopathic bilateral clubfoot is undergoing serial casting using the Ponseti method. After correcting the cavus, adductus, and varus deformities, the foot demonstrates 15 degrees of residual equinus. What is the next most appropriate step?
Explanation
Question 82
A 14-year-old male basketball player presents after feeling a 'pop' in his right knee while jumping. Radiographs reveal a displaced Ogden Type III tibial tubercle avulsion fracture with intra-articular extension. He has significant tense swelling over the anterior aspect of the leg. Which of the following complications is most critically associated with this specific injury pattern?
Explanation
Question 83
A 12-year-old premenarchal female (Risser stage 0) presents with adolescent idiopathic scoliosis. Standing posteroanterior radiographs reveal a primary right thoracic curve measuring 32 degrees and a compensatory left lumbar curve of 20 degrees. What is the most appropriate management recommendation?
Explanation
Question 84
A 4-year-old boy presents with right hip pain, an acute limp, and refusal to bear weight for the past 24 hours. His oral temperature is 38.6°C (101.5°F). Laboratory tests show a WBC count of 13,500/mm3, an ESR of 45 mm/hr, and a CRP of 2.5 mg/dL. He has no history of recent trauma. Based on the Kocher criteria, what is the approximate predicted probability that this child has a septic arthritis of the hip?
Explanation
Question 85
A 3-year-old obese female presents with progressive bilateral bowing of her legs. Radiographs reveal an abrupt varus deformity at the proximal tibial metaphyses with a metaphyseal-diaphyseal angle (Drennan's angle) of 20 degrees bilaterally. Beaking of the medial metaphysis is also noted. What is the most appropriate initial management for this patient?
Explanation
Question 86
A 3-year-old boy, previously treated with serial casting and Achilles tenotomy for idiopathic clubfoot, presents with a relapsed deformity. On examination, he exhibits dynamic supination of the foot during the swing phase of gait. Passive dorsiflexion is 15 degrees past neutral. What is the most appropriate next step in management?
Explanation
Question 87
A 5-year-old girl with spastic quadriplegic cerebral palsy (GMFCS level V) undergoes routine hip surveillance. Radiographs demonstrate a migration percentage of 45% in the right hip. Clinical examination reveals 20 degrees of hip abduction bilaterally with a positive Thomas test. Which of the following is the most appropriate management?
Explanation
Question 88
A 6-week-old female infant is placed in a Pavlik harness for treatment of developmental dysplasia of the hip. At the 1-week follow-up, the parents note that she is no longer kicking her left leg. On examination, the infant lacks active knee extension on the left and the patellar reflex is absent. Which of the following harness configurations is the most likely cause of this complication?
Explanation
Question 89
A 12-year-old boy with a BMI in the 99th percentile undergoes in situ pinning of a severe left slipped capital femoral epiphysis (SCFE). Which of the following factors most strongly indicates the need for prophylactic pinning of the contralateral, asymptomatic right hip?
Explanation
Question 90
A 3-year-old girl is evaluated for bilateral bowlegs. Clinical examination reveals a lateral thrust during gait and a prominent medial metaphyseal beak of the proximal tibia. Radiographs demonstrate a metaphyseal-diaphyseal angle of 20 degrees bilaterally. Based on her age and radiographic findings, what is the most appropriate initial management?
Explanation
Question 91
A 14-year-old boy presents with a 6-month history of frequent right ankle sprains and lateral foot pain. Examination reveals a rigid flatfoot with restricted subtalar motion. Radiographs show a prominent 'C sign' on the lateral view. A CT scan confirms a talocalcaneal coalition involving 65% of the posterior facet with early degenerative changes. He has failed a 6-month trial of casting and orthotics. What is the most appropriate surgical treatment?
Explanation
Question 92
A 6-year-old boy sustains a widely displaced, extension-type supracondylar humerus fracture. In the emergency department, his hand is pale, pulseless, and cool. Following urgent closed reduction and percutaneous pinning, the hand becomes pink and warm with brisk capillary refill (<2 seconds), but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 93
An 8-year-old boy presents with a limp and right hip pain for 3 months. Radiographs reveal fragmentation of the right capital femoral epiphysis consistent with Legg-Calvé-Perthes disease. The lateral pillar height is evaluated and found to be 40% of the normal contralateral side. Based on the Herring Lateral Pillar Classification, what is the prognosis and recommended treatment?
Explanation
Question 94
A 10-year-old girl is evaluated for worsening mid-thigh pain that awakens her at night. Radiographs show a permeative, destructive diaphyseal lesion of the femur with a prominent 'onion skin' periosteal reaction. Core needle biopsy confirms a dense proliferation of uniform, small, round blue cells. Which of the following chromosomal translocations is most characteristic of this malignancy?
Explanation
Question 95
A 9-month-old male infant with a known mutation in the FGFR3 gene presents for routine evaluation. The parents report increased irritability, poor head control, and recent episodes of apnea during sleep. On physical examination, the child has generalized hypotonia but demonstrates hyperreflexia and sustained ankle clonus. Which of the following is the most critical diagnostic study to perform next?
Explanation
Question 96
A 12-year-old boy with a body mass index (BMI) in the 99th percentile undergoes uneventful in situ single-screw fixation for a stable right slipped capital femoral epiphysis (SCFE). The parents inquire about the necessity of prophylactic fixation for the asymptomatic left hip. Which of the following patient factors most strongly supports proceeding with prophylactic pinning of the contralateral hip?
Explanation
Question 97
A 5-year-old boy sustains a completely displaced, extension-type supracondylar fracture of the humerus. On initial evaluation, his hand is pink and warm, but the radial pulse is not palpable. Neurologic examination reveals an inability to actively flex the interphalangeal joint of the thumb. The patient undergoes urgent closed reduction and percutaneous pinning in the operating room. Postoperatively, the hand remains well-perfused, pink, and warm, with a capillary refill time of less than 2 seconds, but the radial pulse remains non-palpable by Doppler. What is the most appropriate next step in management?
Explanation
Question 98
An infant is undergoing treatment with a Pavlik harness for developmental dysplasia of the hip (DDH). During a routine follow-up evaluation, the parents report that the child has stopped kicking the affected leg. On physical examination, the affected knee is held in extension and there is an absence of active quadriceps contraction. This specific complication is most directly caused by which of the following positioning errors within the harness?
Explanation
Question 99
A 9-year-old boy presents to the emergency department with acute right arm pain after throwing a baseball. Radiographs demonstrate a centrally located, expansile, purely lytic lesion in the proximal humeral metaphysis that involves the entire medullary canal. A cortical fragment is seen resting in the dependent portion of the cystic cavity. There is a minimally displaced pathologic fracture through the lesion. What is the most appropriate initial management?
Explanation
Question 100
An 8.5-year-old boy presents with a 4-month history of a painless limp. Radiographs demonstrate Legg-Calvé-Perthes disease in the fragmentation stage. Analysis of the anteroposterior pelvis radiograph shows that the lateral pillar of the affected capital femoral epiphysis maintains 60% of its normal height. Based on the Herring lateral pillar classification and prospective multicenter data, which of the following statements most accurately reflects the current consensus on his management and prognosis?
Explanation
None
