Full Question & Answer Text (for Search Engines)
Question 1:
A 12-year-old boy presents with thigh pain and a periosteal 'onion skin' reaction on X-ray. Biopsy shows small round blue cells. Which of the following chromosomal translocations is most characteristic of this lesion?
Options:
- t(9;22)
- t(11;22)
- t(X;18)
- t(12;16)
- t(2;13)
Correct Answer: t(11;22)
Explanation:
Ewing sarcoma is characterized by the t(11;22) translocation, which results in the EWS-FLI1 fusion protein. t(9;22) is seen in CML or extraskeletal myxoid chondrosarcoma, t(X;18) in synovial sarcoma, t(12;16) in myxoid liposarcoma, and t(2;13) in alveolar rhabdomyosarcoma.
Question 2:
In the acute resuscitation of a hemodynamically unstable patient with an anteroposterior compression (APC) type III pelvic ring injury, what is the most appropriate anatomical landmark for the application of a pelvic circumferential compression device (binder)?
Options:
- Anterior superior iliac spines
- Iliac crests
- Greater trochanters
- Pubic symphysis
- Sacral promontory
Correct Answer: Greater trochanters
Explanation:
Pelvic binders must be placed at the level of the greater trochanters to effectively reduce pelvic volume by applying appropriate compressive forces across the pubic symphysis. Placement over the iliac crests or ASIS can paradoxically open the pelvis further in certain fracture patterns.
Question 3:
A 13-year-old boy with a BMI of 32 presents with acute-on-chronic left hip pain and an inability to bear weight. Radiographs confirm a severe Slipped Capital Femoral Epiphysis (SCFE). Which of the following is a recognized indication for prophylactic in situ pinning of the contralateral asymptomatic hip?
Options:
- Patient age > 14 years
- Endocrine disorder such as hypothyroidism
- Male sex
- Acute presentation < 3 weeks
- Unilateral slip angle > 50 degrees
Correct Answer: Endocrine disorder such as hypothyroidism
Explanation:
Prophylactic pinning of the contralateral hip in SCFE is generally recommended for patients with underlying metabolic or endocrine disorders (e.g., hypothyroidism, renal osteodystrophy), prior radiation therapy, or an age outside the typical range (e.g., < 10 years).
Question 4:
Bone Morphogenetic Proteins (BMPs) act primarily by binding to which type of cellular receptor?
Options:
- G-protein coupled receptor
- Tyrosine kinase receptor
- Serine/threonine kinase receptor
- Intracellular nuclear receptor
- Ligand-gated ion channel
Correct Answer: Serine/threonine kinase receptor
Explanation:
BMPs are part of the TGF-beta superfamily. They bind to transmembrane serine/threonine kinase receptors, leading to phosphorylation of intracellular Smad proteins, which then translocate to the nucleus to regulate gene transcription for osteoblastic differentiation.
Question 5:
During anterior cruciate ligament (ACL) reconstruction, what is the primary biomechanical advantage of using a bone-patellar tendon-bone (BTB) autograft compared to a hamstring autograft?
Options:
- Higher ultimate tensile load
- Greater cross-sectional area
- Faster graft incorporation via bone-to-bone healing
- Decreased donor site morbidity
- Lower rate of contralateral ACL rupture
Correct Answer: Faster graft incorporation via bone-to-bone healing
Explanation:
The primary advantage of BTB autografts is the rapid bone-to-bone healing within the osseous tunnels (typically 6 weeks), compared to the slower soft-tissue-to-bone healing of hamstring grafts (8-12 weeks). Hamstring grafts have a higher ultimate tensile load and lower donor site morbidity (less anterior knee pain).
Question 6:
A 65-year-old man presents with progressive clumsiness in his hands and broad-based gait. Examination reveals hyperreflexia and a positive Hoffman's sign. MRI shows cervical spondylotic myelopathy. Which of the following sagittal canal diameters is generally considered the absolute threshold for critical cervical stenosis?
Options:
- 10 mm
- 13 mm
- 15 mm
- 17 mm
- 20 mm
Correct Answer: 10 mm
Explanation:
A sagittal cervical canal diameter of less than 10 mm is highly correlated with critical cervical stenosis and myelopathy. The normal sagittal diameter is 17-18 mm. A diameter of less than 13 mm defines congenital cervical stenosis.
Question 7:
A 25-year-old carpenter sustains a laceration over the volar aspect of the proximal phalanx of his index finger, cutting both the FDS and FDP tendons. According to Verdan's classification, which zone of flexor tendon injury does this represent?
Options:
- Zone I
- Zone II
- Zone III
- Zone IV
- Zone V
Correct Answer: Zone II
Explanation:
Zone II (historically known as 'No Man/'s Land') extends from the A1 pulley (distal palmar crease) to the FDS insertion on the middle phalanx. Injuries here involve both FDS and FDP within the fibro-osseous sheath, complicating repair due to adhesion risk.
Question 8:
In the evaluation of a suspected Lisfranc injury, the 'fleck sign' on a standard AP radiograph of the foot represents an avulsion fracture originating from which anatomical structure?
Options:
- Plantar aspect of the first cuneiform
- Base of the second metatarsal
- Base of the first metatarsal
- Dorsal aspect of the navicular
- Cuboid
Correct Answer: Base of the second metatarsal
Explanation:
The 'fleck sign' is a pathognomonic avulsion fracture occurring at the attachment of the Lisfranc ligament at the medial base of the second metatarsal. The ligament courses from the medial cuneiform to the base of the second metatarsal.
Question 9:
A 30-year-old male sustains a high-energy Pauwels type III femoral neck fracture. Which of the following internal fixation constructs provides the greatest biomechanical stability against vertical shear forces?
Options:
- Three parallel cancellous screws placed in an inverted triangle
- Dynamic hip screw (DHS) with an anti-rotation screw
- Two parallel cancellous screws
- Cephalomedullary nail
- Unipolar hemiarthroplasty
Correct Answer: Dynamic hip screw (DHS) with an anti-rotation screw
Explanation:
Pauwels type III fractures have a high vertical fracture angle (>50 degrees), subjecting the fracture to significant vertical shear forces. A fixed-angle device like a DHS, often supplemented with a derotational screw, provides superior biomechanical stability against shear forces compared to multiple cancellous screws.
Question 10:
Which of the following total hip arthroplasty bearing surfaces is associated with the lowest volumetric wear rate but carries the specific complication risk of stripe wear and squeaking?
Options:
- Cobalt-chrome on highly cross-linked polyethylene
- Ceramic on highly cross-linked polyethylene
- Ceramic on ceramic
- Metal on metal
- Oxinium on highly cross-linked polyethylene
Correct Answer: Ceramic on ceramic
Explanation:
Ceramic-on-ceramic bearings have the lowest volumetric wear rates of all modern bearing surfaces and produce biologically inert wear debris. However, they carry unique risks including catastrophic brittle fracture, squeaking (due to edge loading or loss of fluid film lubrication), and stripe wear.
Question 11:
In biomechanics, the phenomenon where a tissue maintains a constant deformation (strain) over time while the applied force (stress) gradually decreases is known as:
Options:
- Creep
- Stress relaxation
- Hysteresis
- Fatigue failure
- Anisotropy
Correct Answer: Stress relaxation
Explanation:
Stress relaxation is a viscoelastic property defined as the decrease in stress over time when a material is held at a constant strain. Creep is the opposite: increasing strain over time under a constant stress.
Question 12:
When applying the Ponseti method for the treatment of idiopathic clubfoot, what is the first deformity that must be corrected?
Options:
- Equinus
- Varus
- Adductus
- Cavus
- Internal tibial torsion
Correct Answer: Cavus
Explanation:
The sequence of correction in the Ponseti method follows the acronym CAVE: Cavus, Adductus, Varus, Equinus. The cavus deformity is corrected first by elevating the first ray to align the forefoot with the hindfoot.
Question 13:
A 55-year-old patient has a large, aggressive-appearing lytic lesion in the proximal femur with endosteal scalloping and 'popcorn' calcifications. Biopsy confirms grade II conventional chondrosarcoma. What is the preferred primary treatment?
Options:
- Neoadjuvant chemotherapy followed by wide surgical resection
- Radiation therapy alone
- Intralesional curettage and bone grafting
- Wide surgical resection
- Amputation
Correct Answer: Wide surgical resection
Explanation:
Conventional chondrosarcomas (Grades II and III) are highly resistant to both chemotherapy and radiation therapy. The gold standard for treatment is wide surgical resection. Intralesional curettage is only appropriate for benign lesions (enchondromas) or very select low-grade (Grade I) tumors in appendicular locations.
Question 14:
In a patient with a closed tibial shaft fracture and suspected acute compartment syndrome, which of the following pressure measurements is generally accepted as an absolute indication for fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 25 mmHg
- Delta P (Diastolic blood pressure minus compartment pressure) < 30 mmHg
- Delta P (Systolic blood pressure minus compartment pressure) < 40 mmHg
- Mean arterial pressure minus compartment pressure < 20 mmHg
Correct Answer: Delta P (Diastolic blood pressure minus compartment pressure) < 30 mmHg
Explanation:
The delta P measurement is the most reliable indicator for fasciotomy. It is calculated by subtracting the intracompartmental pressure from the diastolic blood pressure. A delta P of less than 30 mmHg strongly indicates inadequate tissue perfusion and is the standard threshold for surgical intervention.
Question 15:
A 22-year-old athlete sustains a recurrent anterior shoulder dislocation. Preoperative imaging demonstrates an 'engaging' Hill-Sachs lesion. What specific adjunctive surgical procedure is most commonly performed alongside a Bankart repair to address this lesion?
Options:
- Latarjet procedure
- Remplissage procedure
- Putti-Platt procedure
- Eden-Hybinette procedure
- Weaver-Dunn procedure
Correct Answer: Remplissage procedure
Explanation:
An engaging Hill-Sachs lesion can lever the humeral head out of the glenoid during abduction and external rotation. The Remplissage procedure addresses this by tenodesing the infraspinatus tendon and posterior capsule into the defect, preventing it from engaging the anterior glenoid rim. Latarjet addresses glenoid bone loss.
Question 16:
According to the Thoracolumbar Injury Classification and Severity (TLICS) score, which of the following posterior ligamentous complex (PLC) statuses contributes the highest number of points to the total score?
Options:
- Intact
- Indeterminate/suspected injury
- Disrupted
- Ossified
- Attenuated
Correct Answer: Disrupted
Explanation:
In the TLICS scoring system, the Posterior Ligamentous Complex (PLC) status is scored as follows: Intact = 0 points, Suspected/Indeterminate = 2 points, Disrupted = 3 points. A total score of >4 generally indicates surgical management.
Question 17:
The predominant blood supply to the proximal pole of the scaphoid is derived from which of the following vessels?
Options:
- Superficial palmar branch of the radial artery
- Dorsal carpal branch of the radial artery
- Anterior interosseous artery
- Deep palmar arch
- Ulnar artery
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The scaphoid receives its primary vascular supply (70-80%) from the dorsal carpal branch of the radial artery, which enters at the distal third of the scaphoid and flows retrograde. This retrograde blood flow is why proximal pole fractures are at a high risk for avascular necrosis (AVN).
Question 18:
A 55-year-old diabetic patient presents with a warm, swollen, erythematous foot without ulceration. Radiographs show extensive fragmentation, periarticular debris, and subluxation of the midfoot joints. According to the Eichenholtz classification, what stage of Charcot arthropathy does this represent?
Options:
- Stage 0 (High risk)
- Stage 1 (Development/Fragmentation)
- Stage 2 (Coalescence)
- Stage 3 (Reconstruction/Consolidation)
- Stage 4 (Ulceration)
Correct Answer: Stage 1 (Development/Fragmentation)
Explanation:
Eichenholtz Stage 1 (Development/Fragmentation) is characterized clinically by a warm, red, swollen foot and radiographically by joint subluxation/dislocation, bone fragmentation, and debris. Stage 2 (Coalescence) shows absorption of fine debris and early fusion. Stage 3 (Reconstruction) shows rounding of bone ends and solid arthrodesis.
Question 19:
In mechanical alignment principles for total knee arthroplasty (TKA), the femoral component should typically be placed in what degree of external rotation relative to the posterior condylar axis to ensure symmetric flexion gaps?
Options:
- 0 degrees
- 3 degrees
- 5 degrees
- 7 degrees
- 10 degrees
Correct Answer: 3 degrees
Explanation:
In standard mechanical alignment for TKA, the femoral component is typically externally rotated 3 degrees relative to the posterior condylar axis. This compensates for the natural 3-degree varus angle of the proximal tibia (which is cut perpendicularly in mechanical alignment), helping to create a rectangular, balanced flexion gap.
Question 20:
A 40-year-old farmer sustains an open tibial shaft fracture after his leg is caught in agricultural machinery. The wound is 12 cm long with extensive muscle stripping and gross soil contamination. According to evidence-based guidelines, what is the most appropriate initial empirical antibiotic regimen?
Options:
- First-generation cephalosporin alone
- First-generation cephalosporin + aminoglycoside
- First-generation cephalosporin + fluoroquinolone
- First-generation cephalosporin + aminoglycoside + high-dose penicillin
- Vancomycin + Piperacillin/Tazobactam
Correct Answer: First-generation cephalosporin + aminoglycoside + high-dose penicillin
Explanation:
This is a Gustilo-Anderson Type IIIA open fracture with gross agricultural contamination, putting the patient at high risk for Clostridium perfringens infection. The standard antibiotic protocol for type III open fractures is a first-generation cephalosporin and an aminoglycoside. High-dose penicillin (or ampicillin) is added specifically for severe agricultural, fecal, or standing-water contamination to provide anaerobic coverage.
Question 21:
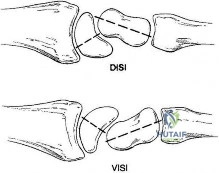
A 13-year-old obese male presents with right hip pain, an antalgic gait, and an obligate external rotation of the hip upon flexion. Radiographs demonstrate a slipped capital femoral epiphysis (SCFE). Relative to the femoral neck, in which anatomical direction does the epiphysis translate in a typical SCFE?
Options:
- Anterior and superior
- Anterior and inferior
- Posterior and superior
- Posterior and inferior
- Directly posterior
Correct Answer: Posterior and inferior
Explanation:
In a slipped capital femoral epiphysis (SCFE), the epiphysis typically remains within the acetabulum while the femoral neck displaces anteriorly and superiorly. Therefore, relative to the femoral neck, the epiphysis displaces posteriorly and inferiorly. This creates the classic 'ice cream slipping off the cone' radiographic appearance on the lateral view.
Question 22:
A 32-year-old female presents with a destructive, eccentrically located lytic lesion in the distal femur epiphysis extending to the subchondral bone. Histology reveals neoplastic mononuclear cells and abundant reactive multinucleated giant cells. Which of the following is an appropriate targeted medical therapy for advanced or unresectable cases of this tumor?
Options:
- Imatinib
- Denosumab
- Zoledronic acid
- Rituximab
- Methotrexate
Correct Answer: Denosumab
Explanation:
The clinical and histologic description is classic for a Giant Cell Tumor (GCT) of bone. The neoplastic mononuclear cells express RANKL, which recruits and activates the multinucleated giant cells (osteoclast-like cells) responsible for bone destruction. Denosumab is a monoclonal antibody that targets and binds RANKL, inhibiting this process, and is an FDA-approved treatment for advanced or unresectable GCTs.
Question 23:
Which zone of articular cartilage contains the largest diameter collagen fibrils, the highest concentration of proteoglycans, and chondrocytes arranged in vertical columns?
Options:
- Superficial (tangential) zone
- Transitional (middle) zone
- Deep (radial) zone
- Calcified zone
- Tidemark
Correct Answer: Deep (radial) zone
Explanation:
The deep (radial) zone of articular cartilage is characterized by chondrocytes arranged in vertical columns parallel to the collagen fibers, which are themselves oriented vertically (perpendicular to the joint surface). This zone has the largest diameter collagen fibrils and the highest concentration of proteoglycans, providing maximal resistance to compressive forces.
Question 24:
A 28-year-old male is brought to the ED after a motorcycle collision. He has an open-book pelvic fracture (APC III) with a symphyseal diastasis of 4 cm and is hemodynamically unstable despite initial fluid resuscitation (BP 80/40 mmHg, HR 130 bpm). A FAST scan of the abdomen is negative. What is the most appropriate next step in management?
Options:
- Immediate transfer for pelvic arterial embolization
- Immediate open reduction and internal fixation of the anterior ring
- Application of a pelvic binder and preperitoneal pelvic packing
- Retrograde urethrogram to rule out associated injuries
- Exploratory laparotomy
Correct Answer: Application of a pelvic binder and preperitoneal pelvic packing
Explanation:
In a hemodynamically unstable patient with an unstable pelvic ring injury and a negative FAST scan, the source of bleeding is presumed to be the pelvis (mostly venous from the presacral plexus or cancellous bone). The immediate priority is closing the pelvic volume (using a binder or sheet) to induce a tamponade effect, often followed promptly by preperitoneal pelvic packing or angiography if packing fails or arterial bleeding is strongly suspected. Stabilization and packing take precedence over definitive ORIF or urological workup in the acute resuscitation phase.
Question 25:
A 4-year-old boy presents with a 2-day history of right hip pain, a limp, and a tactile fever. Which of the following is NOT a parameter included in the classic Kocher criteria used to differentiate septic arthritis from transient synovitis of the pediatric hip?
Options:
- Non-weight-bearing on the affected side
- Erythrocyte sedimentation rate (ESR) > 40 mm/hr
- Serum white blood cell (WBC) count > 12,000/mm3
- Temperature > 38.5 degrees C
- Presence of a joint effusion on ultrasound
Correct Answer: Presence of a joint effusion on ultrasound
Explanation:
The classic Kocher criteria for predicting septic arthritis of the hip in children include four parameters: Non-weight-bearing status, ESR > 40 mm/hr, WBC count > 12,000/mm3, and Temperature > 38.5°C. C-reactive protein (CRP) > 20 mg/L was later identified by Caird et al. as an excellent independent predictor. The presence of a joint effusion on ultrasound confirms fluid but does not differentiate between transient synovitis and septic arthritis, and is not a Kocher criterion.
Question 26:
A 68-year-old man presents with progressive aching pain in his right thigh and diminished hearing over the past year. Radiographs of his femur show cortical thickening, coarse trabeculae, and anterior bowing. Alkaline phosphatase is markedly elevated, but serum calcium and phosphate are normal. What is the primary cellular defect initiating this disease process?
Options:
- Defective mineralization of osteoid by osteoblasts
- Excessive, uncoordinated osteoclastic bone resorption
- Impaired synthesis of type I collagen
- Overproduction of parathyroid hormone
- Deficient osteoprotegerin (OPG) production
Correct Answer: Excessive, uncoordinated osteoclastic bone resorption
Explanation:
The patient has Paget's disease of bone, characterized by elevated alkaline phosphatase, normal calcium/phosphate, and classic radiographic findings (cortical thickening, coarse trabeculae). The disease is initiated by an initial phase of excessive, uncoordinated bone resorption by abnormal, large, multinucleated osteoclasts. This is followed by a mixed phase and eventually a sclerotic phase of disorganized, woven bone formation by osteoblasts.
Question 27:
When optimizing a screw for fixation in poor-quality osteoporotic bone, which of the following structural alterations will yield the greatest increase in the screw's pullout strength?
Options:
- Increasing the outer diameter
- Increasing the inner (root) diameter
- Increasing the thread pitch
- Decreasing the length of screw engagement
- Utilizing a core-tapered screw design
Correct Answer: Increasing the outer diameter
Explanation:
Pullout strength of a screw is primarily determined by the volume of bone caught between the threads. The formula for pullout strength is proportional to the outer diameter, the length of engagement, and the shear strength of the bone material. Increasing the outer diameter increases the thread volume and has the most significant impact on pullout strength. Conversely, increasing the inner (root) diameter decreases the thread depth, which would lower pullout strength.
Question 28:
A 24-year-old athlete sustains a traction injury to his shoulder and subsequently presents with medial scapular winging that is accentuated when pushing against a wall. The affected nerve is formed by the confluence of which of the following nerve roots?
Options:
- C5 only
- C5 and C6
- C5, C6, and C7
- C7, C8, and T1
- C8 and T1
Correct Answer: C5, C6, and C7
Explanation:
Medial scapular winging is caused by paralysis of the serratus anterior muscle, which is innervated by the long thoracic nerve. The long thoracic nerve arises directly from the ventral rami of the C5, C6, and C7 nerve roots.
Question 29:
A 14-year-old boy presents with severe thigh pain and intermittent low-grade fevers. Radiographs show a permeative diaphyseal lesion of the femur with an 'onion-skin' periosteal reaction. A core biopsy confirms a small round blue cell tumor. Which of the following translocations and resulting fusion genes is most characteristic of this diagnosis?
Options:
- t(X;18) SYT-SSX
- t(11;22) EWS-FLI1
- t(2;13) PAX3-FKHR
- t(12;16) FUS-CHOP
- t(9;22) BCR-ABL
Correct Answer: t(11;22) EWS-FLI1
Explanation:
The clinical and radiographic presentation is classic for Ewing sarcoma. Over 85% of Ewing sarcomas are driven by a balanced translocation between chromosomes 11 and 22, t(11;22)(q24;q12), which results in the EWS-FLI1 fusion protein. t(X;18) is seen in synovial sarcoma; t(2;13) in alveolar rhabdomyosarcoma; t(12;16) in myxoid liposarcoma.
Question 30:
Bone morphogenetic proteins (BMPs) play a crucial role in bone healing by stimulating the differentiation of mesenchymal stem cells into osteoblasts. Which of the following BMPs is an FDA-approved osteoinductive agent commonly used in spinal fusion and the treatment of open tibia fractures?
Options:
- BMP-1
- BMP-2
- BMP-3
- BMP-6
- BMP-13
Correct Answer: BMP-2
Explanation:
Recombinant human BMP-2 (rhBMP-2) is heavily utilized and FDA-approved for anterior lumbar interbody fusion (ALIF) and acute open tibial shaft fractures. BMP-7 (also known as Osteogenic Protein-1 or OP-1) was previously approved for recalcitrant tibial nonunions. Notably, BMP-1 is not actually a member of the TGF-beta superfamily (it is a metalloproteinase), and BMP-3 has an inhibitory effect on bone formation.
Question 31:
In the Ponseti method for the non-operative treatment of congenital talipes equinovarus (clubfoot), what is the correct anatomical sequence of deformity correction during serial casting?
Options:
- Cavus, Adductus, Varus, Equinus
- Adductus, Varus, Cavus, Equinus
- Cavus, Varus, Adductus, Equinus
- Equinus, Cavus, Adductus, Varus
- Varus, Cavus, Adductus, Equinus
Correct Answer: Cavus, Adductus, Varus, Equinus
Explanation:
The Ponseti method corrects the clubfoot deformities in a specific, sequential order remembered by the mnemonic CAVE: Cavus (corrected first by supinating the forefoot to align with the hindfoot), Adductus, Varus, and finally Equinus (which often requires a percutaneous Achilles tenotomy as the final step).
Question 32:
A 35-year-old man sustains a closed comminuted fracture of the tibial diaphysis. He reports severe pain out of proportion to his injury, exacerbated by passive extension of his toes. The clinical suspicion for acute compartment syndrome is high, and compartment pressures are measured. Which of the following measurements is the most reliable threshold for indicating fasciotomy?
Options:
- Absolute compartment pressure > 20 mmHg
- Absolute compartment pressure > 25 mmHg
- Diastolic blood pressure minus compartment pressure < 30 mmHg
- Mean arterial pressure minus compartment pressure < 40 mmHg
- Systolic blood pressure minus compartment pressure < 30 mmHg
Correct Answer: Diastolic blood pressure minus compartment pressure < 30 mmHg
Explanation:
The 'Delta P' (Diastolic Blood Pressure minus the intracompartmental pressure) is the most reliable objective measurement for diagnosing acute compartment syndrome. A Delta P of less than 30 mmHg indicates inadequate tissue perfusion and is a strong indication for emergent fasciotomy. Absolute pressures are less reliable because perfusion pressure varies significantly between patients (e.g., hypotensive trauma patients vs. hypertensive individuals).
Question 33:
In conventional metal-on-polyethylene total hip arthroplasty, osteolysis and aseptic loosening are primarily driven by a macrophage-mediated response to particulate debris. What is the size range of polyethylene wear particles that is most biologically active in stimulating this macrophage-mediated osteolytic response?
Options:
- 0.1 to 1.0 micrometers
- 5 to 10 micrometers
- 15 to 25 micrometers
- 50 to 100 micrometers
- 100 to 500 micrometers
Correct Answer: 0.1 to 1.0 micrometers
Explanation:
Submicron polyethylene particles, specifically in the size range of 0.1 to 1.0 micrometers (often averaging ~0.5 microns), are the most biologically active. Macrophages readily phagocytose particles of this size but cannot digest them, leading to cellular activation and the release of pro-inflammatory cytokines (TNF-alpha, IL-1, IL-6), which subsequently stimulate osteoclastogenesis and periprosthetic osteolysis.
Question 34:
A 55-year-old female with long-standing, untreated carpal tunnel syndrome presents with severe thenar atrophy. Which of the following thumb muscles is typically spared in this condition because of its different innervation?
Options:
- Abductor pollicis brevis
- Opponens pollicis
- Superficial head of the flexor pollicis brevis
- Adductor pollicis
- First lumbrical
Correct Answer: Adductor pollicis
Explanation:
The recurrent motor branch of the median nerve innervates the thenar muscles: Abductor Pollicis Brevis (APB), Opponens Pollicis (OP), and the superficial head of the Flexor Pollicis Brevis (FPB). Severe median nerve compression in the carpal tunnel leads to atrophy of these muscles. The Adductor Pollicis is innervated by the deep branch of the ulnar nerve and is therefore spared in carpal tunnel syndrome.
Question 35:
A 22-year-old soccer player sustains a non-contact twisting injury to the knee. Radiographs reveal an elliptic avulsion fracture of the lateral tibial plateau (Segond fracture). This radiographic finding is virtually pathognomonic for an anterior cruciate ligament (ACL) tear. Which specific structure is primarily responsible for generating this avulsion fracture?
Options:
- Iliotibial band
- Biceps femoris tendon
- Anterolateral ligament (ALL) and lateral capsular complex
- Fibular collateral ligament
- Popliteus tendon
Correct Answer: Anterolateral ligament (ALL) and lateral capsular complex
Explanation:
A Segond fracture is an avulsion fracture of the lateral tibial plateau that occurs with internal rotation and varus stress. It is strongly associated with ACL tears. Anatomical and biomechanical studies have demonstrated that this bony avulsion is produced by tension from the anterolateral ligament (ALL) and the associated lateral capsular complex.
Question 36:
A 40-year-old man falls from a height of 20 feet and sustains a burst fracture of T12. On examination in the trauma bay, he has flaccid paralysis of his lower extremities, absent lower extremity reflexes, and an absent bulbocavernosus reflex. His vital signs are stable (HR 85 bpm, BP 120/80 mmHg). The absence of the bulbocavernosus reflex in this setting most accurately signifies which of the following?
Options:
- Complete spinal cord injury
- Incomplete spinal cord injury
- Spinal shock
- Neurogenic shock
- Cauda equina syndrome
Correct Answer: Spinal shock
Explanation:
The bulbocavernosus reflex is a polysynaptic reflex mediated by the S2-S4 segments of the spinal cord. Its absence in the acute phase of a severe spinal injury indicates a state of 'spinal shock'—a temporary physiologic disruption of spinal cord function and reflexes below the level of injury. A spinal cord injury cannot be officially classified as complete or incomplete until the patient emerges from spinal shock (indicated by the return of the bulbocavernosus reflex). Neurogenic shock refers to hemodynamic instability (bradycardia and hypotension) due to loss of sympathetic tone, which this patient does not have.
Question 37:
Which of the following internal fixation constructs relies predominantly on intramembranous and endochondral ossification (secondary bone healing) to achieve fracture union?
Options:
- Compression plating of a transverse radius fracture
- Lag screw fixation of a medial malleolus fracture
- Intramedullary nailing of a comminuted tibial shaft fracture
- Tension band wiring of an olecranon fracture
- Dual plating of a distal humerus fracture achieving absolute stability
Correct Answer: Intramedullary nailing of a comminuted tibial shaft fracture
Explanation:
Fracture healing can be categorized into primary (direct) and secondary (indirect) healing. Primary healing occurs with absolute stability (no micro-motion) and relies on direct Haversian remodeling without a callus (e.g., compression plating, lag screws). Secondary healing occurs under conditions of relative stability and involves callus formation via endochondral and intramembranous ossification. An intramedullary nail provides relative stability and heals via secondary bone healing.
Question 38:
A 42-year-old recreational athlete sustains an acute Achilles tendon rupture. When comparing modern non-operative management (utilizing an early functional rehabilitation protocol) to open surgical repair, which of the following statements regarding outcomes is most accurate based on current high-level evidence?
Options:
- Surgical repair has a significantly higher rate of re-rupture.
- Non-operative management has a significantly higher rate of deep infection.
- Surgical repair and non-operative management with early functional rehab have similar re-rupture rates.
- Non-operative management results in significantly greater plantarflexion strength at 1 year.
- Surgical repair requires a longer period of rigid immobilization.
Correct Answer: Surgical repair and non-operative management with early functional rehab have similar re-rupture rates.
Explanation:
Recent Level 1 evidence (including large randomized controlled trials) demonstrates that when modern, dynamic early functional rehabilitation protocols are employed, the re-rupture rates between non-operative and operative management of acute Achilles tendon ruptures are remarkably similar (and low). Operative management carries a higher risk of wound complications and infection. Plantarflexion strength is generally equivalent or slightly favored in surgical groups depending on the study, but not significantly superior in non-operative groups.
Question 39:
A 26-year-old male is admitted with bilateral closed femoral shaft fractures. On post-injury day 2, he becomes acutely hypoxic, confused, and develops a petechial rash over his axillae and conjunctivae. Which of the following pathophysiological mechanisms is most directly responsible for the development of his condition?
Options:
- Direct pulmonary contusion from the initial trauma
- Release of marrow fat into the venous circulation leading to mechanical occlusion and biochemical endothelial damage
- Deep vein thrombosis embolizing to the pulmonary arterial tree
- Over-resuscitation with crystalloid fluids leading to acute respiratory distress syndrome (ARDS)
- Severe systemic inflammatory response syndrome (SIRS) primarily driven by bowel ischemia
Correct Answer: Release of marrow fat into the venous circulation leading to mechanical occlusion and biochemical endothelial damage
Explanation:
The patient is presenting with the classic triad of Fat Embolism Syndrome (FES): hypoxemia, neurological abnormalities, and a petechial rash. FES typically occurs 24-72 hours after long bone fractures. The pathophysiology is bi-modal: mechanical obstruction of the pulmonary capillaries by marrow fat globules, followed by a biochemical phase where free fatty acids cause direct toxic damage to the pulmonary capillary endothelium, leading to ARDS-like pulmonary edema.
Question 40:
A 45-year-old female with a history of severe celiac disease presents with diffuse, dull bone pain and proximal muscle weakness. Radiographs demonstrate bilateral radiolucent bands perpendicular to the cortex in the medial femoral necks (Looser zones). Which of the following laboratory profiles is most characteristic of her underlying metabolic bone disease?
Options:
- High calcium, low phosphorus, high parathyroid hormone (PTH)
- Normal calcium, normal phosphorus, normal alkaline phosphatase (ALP)
- Low or normal calcium, low phosphorus, high PTH, high ALP
- High calcium, high phosphorus, low PTH, low ALP
- Normal calcium, high phosphorus, normal PTH
Correct Answer: Low or normal calcium, low phosphorus, high PTH, high ALP
Explanation:
The patient has osteomalacia secondary to vitamin D malabsorption (celiac disease). Looser zones (pseudofractures) are pathognomonic radiographic findings. Deficient Vitamin D leads to decreased intestinal calcium absorption, triggering secondary hyperparathyroidism (high PTH). High PTH maintains serum calcium at low-normal or low levels but causes renal phosphate wasting (low phosphorus). Alkaline phosphatase (ALP) is elevated due to increased osteoblast activity attempting to mineralize the abundant unmineralized osteoid.