Comprehensive Introduction and Patho-Epidemiology
Neuromuscular scoliosis (NMS) represents a profoundly complex and heterogeneous spectrum of spinal deformities arising secondary to underlying myopathic or neuropathic systemic diseases. Unlike adolescent idiopathic scoliosis (AIS), which typically develops in otherwise healthy individuals during the adolescent growth spurt, neuromuscular curves frequently present much earlier in life, progress at an aggressively rapid rate, and relentlessly continue to deteriorate long after skeletal maturity is achieved. The underlying etiology of the spinal deformity in these patients is fundamentally multifactorial. However, the primary biomechanical failure cascade is invariably driven by a catastrophic loss of truncal muscle strength, the absence of voluntary motor control, and profound deficits in critical sensory feedback mechanisms, such as spatial proprioception. In the flexible, rapidly growing spinal column of a juvenile patient, these severe neuromuscular deficits lead to unremitting asymmetric loading.

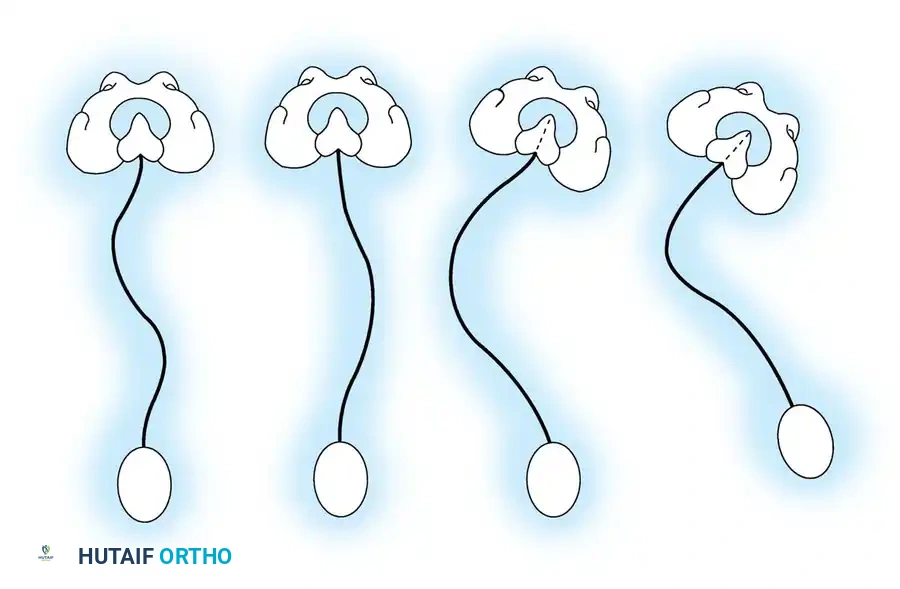
As the spine collapses under the constant force of gravity, increased pressure on the concave side of the curve directly inhibits physeal growth—a classic manifestation of the Hueter-Volkmann principle. This asymmetric growth arrest results in structural wedging of the vertebral bodies, transforming a flexible, postural deformity into a rigid, structural one. Furthermore, the osseous anatomy in these patients is frequently compromised by severe disuse osteopenia, chronic malnutrition, and the adverse effects of long-term antiepileptic medications. These factors coalesce to create a highly unfavorable environment for surgical instrumentation and arthrodesis, demanding specialized techniques for fixation. The morphological presentation of NMS typically involves long, sweeping, C-shaped deformities that extend distally to encompass the sacrum and pelvis, making severe pelvic obliquity a hallmark of the disease process.
The Scoliosis Research Society (SRS) classification for neuromuscular scoliosis divides the etiology into two primary pathophysiological categories: Neuropathic and Myopathic. Neuropathic deformities are further subdivided into Upper Motor Neuron (UMN) lesions and Lower Motor Neuron (LMN) lesions. UMN lesions include cerebral palsy (CP), spinocerebellar degenerations (such as Friedreich ataxia and Charcot-Marie-Tooth disease), syringomyelia, and spinal cord tumors or trauma. LMN lesions encompass conditions like poliomyelitis, traumatic paraplegia or quadriplegia, spinal muscular atrophy (SMA), and dysautonomia. Myopathic deformities arise from intrinsic muscle pathology, including arthrogryposis multiplex congenita, various muscular dystrophies (Duchenne, Limb-girdle, Facioscapulohumeral), congenital hypotonia, and myotonia dystrophica.
Differentiating between a neuropathic and myopathic etiology is not merely an academic exercise; it is absolutely critical for comprehensive preoperative planning and risk stratification. For instance, patients presenting with Duchenne muscular dystrophy exhibit a notoriously high incidence of intrinsic cardiomyopathy and are highly susceptible to malignant hyperthermia, demanding specialized, meticulously planned anesthetic protocols. Conversely, patients with spastic quadriplegic cerebral palsy often present with severe, rigid joint contractures and profound gastrointestinal dysfunction, requiring a completely different set of preoperative optimizations. The overarching goal of operative treatment in this patient population is never cosmetic. Rather, the definitive objective is to achieve a solid arthrodesis that maintains a balanced spine in the coronal and sagittal planes over a level pelvis, thereby optimizing sitting balance, maximizing pulmonary function, preventing decubitus ulceration, and improving the overall quality of life and ease of nursing care.
Detailed Surgical Anatomy and Biomechanics
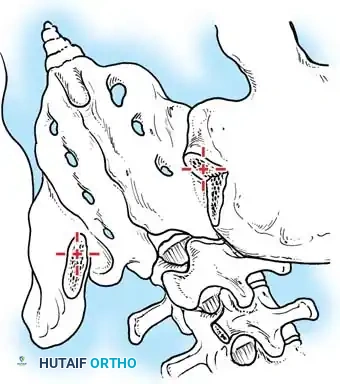
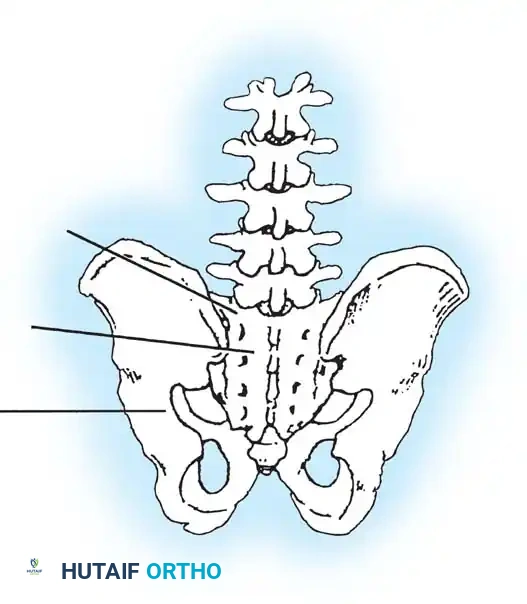
The surgical anatomy of the neuromuscular spine is markedly distorted compared to the normative anatomy encountered in idiopathic deformities, presenting unique intraoperative challenges for the orthopedic surgeon. The osteology is typically characterized by profound disuse osteopenia, rendering the vertebral bodies and posterior elements structurally deficient. Pedicle morphology is frequently dysplastic, with extreme narrowing on the concavity of the curve and rotational distortion that alters standard anatomical landmarks for screw trajectory. Facet joints may exhibit severe hypertrophy due to chronic asymmetric loading or, conversely, hypoplasia in non-ambulatory patients. The sacropelvic junction—the foundation of the neuromuscular construct—is of paramount importance. The anatomy of the iliac crests, the S1 and S2 pedicles, and the sacral ala must be meticulously evaluated on preoperative imaging, as these structures will bear the immense cantilever forces required to correct pelvic obliquity and maintain sagittal balance.
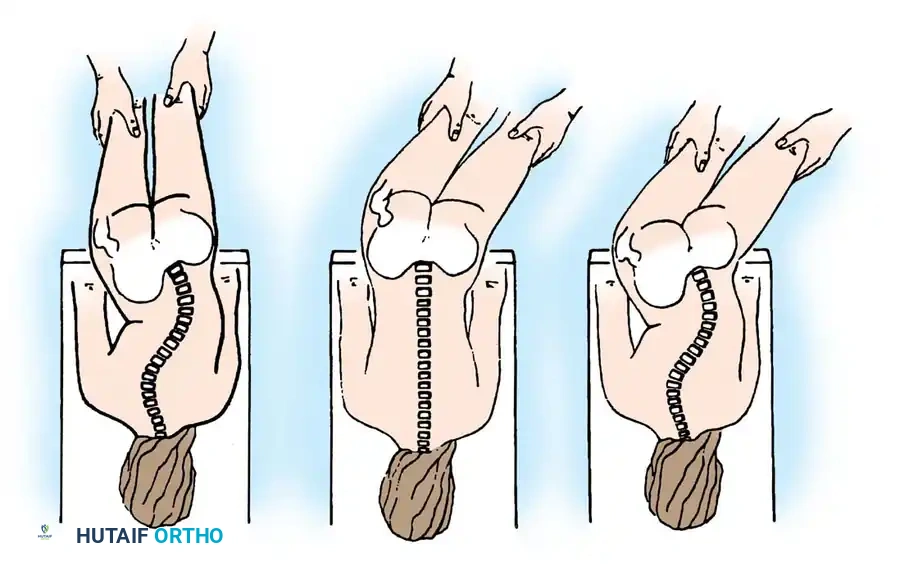
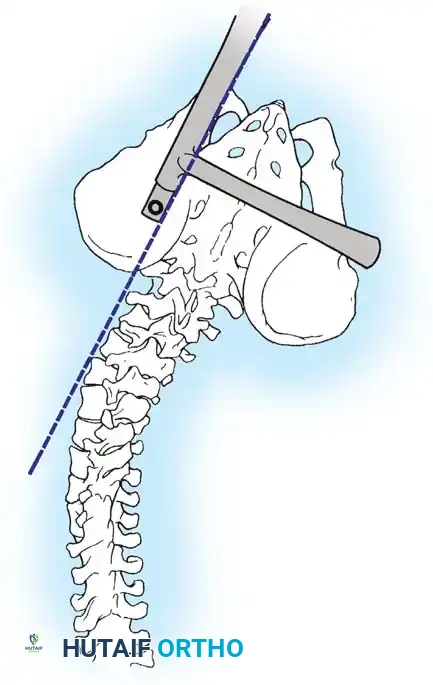
The musculoligamentous anatomy in neuromuscular patients is equally pathological. Spasticity or flaccidity of the paraspinal musculature directly dictates the progression and rigidity of the curve. Furthermore, extra-spinal contractures play a critical role in the biomechanics of the deformity. Severe contractures of the hip flexors, hamstrings, and adductors are ubiquitous in conditions like cerebral palsy. The surgeon must astutely differentiate between a fixed spinopelvic deformity (supra-pelvic obliquity) and obliquity driven by hip contractures (infra-pelvic obliquity). If pelvic obliquity resolves with abduction or adduction of the hips during clinical examination, the primary driver is infra-pelvic, and soft tissue releases must precede or accompany spinal fusion. Failure to recognize and address severe hip contractures will result in persistent seating imbalance and transmit immense, unsustainable stress to the distal spinopelvic instrumentation, invariably leading to catastrophic hardware failure.
From a biomechanical perspective, the neuromuscular spine functions as a collapsing column under the relentless force of gravity. Devoid of the dynamic stabilizing forces normally provided by the erector spinae and abdominal musculature, the spine succumbs to a combination of axial loading and shear forces. This results in global sagittal plane decompensation, typically manifesting as severe hyperkyphosis and complete loss of physiological lumbar lordosis. In the coronal plane, the long, sweeping C-curve translates the center of gravity laterally, shifting the patient's weight disproportionately onto a single ischial tuberosity. This asymmetric seating pressure is the primary etiology of recalcitrant decubitus ulcers, which can rapidly progress to deep tissue infection and osteomyelitis of the pelvis.
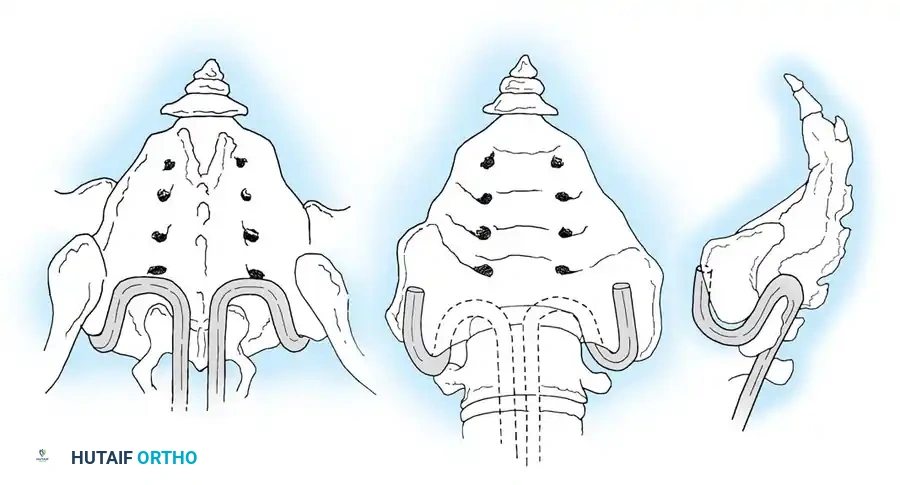
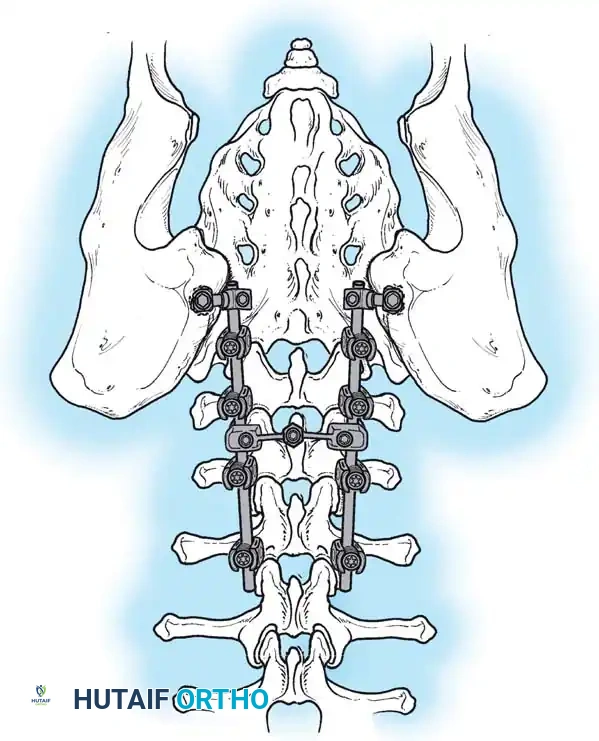
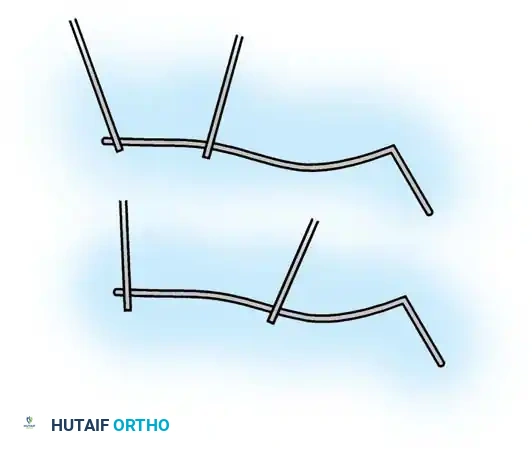
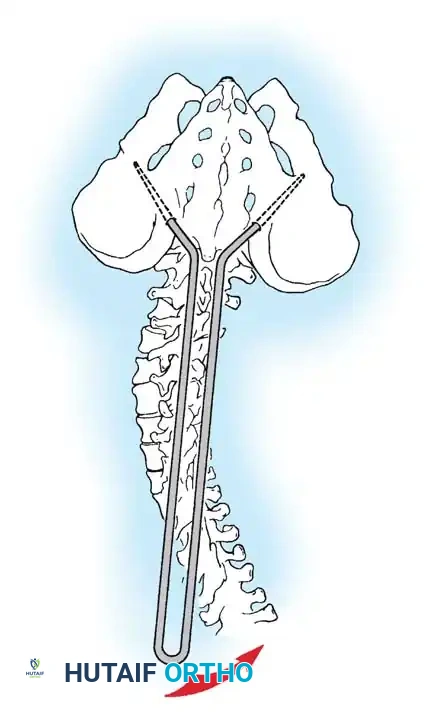
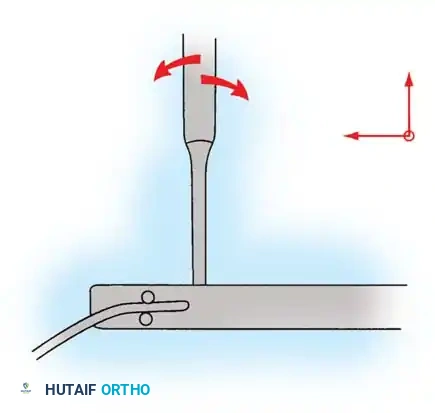
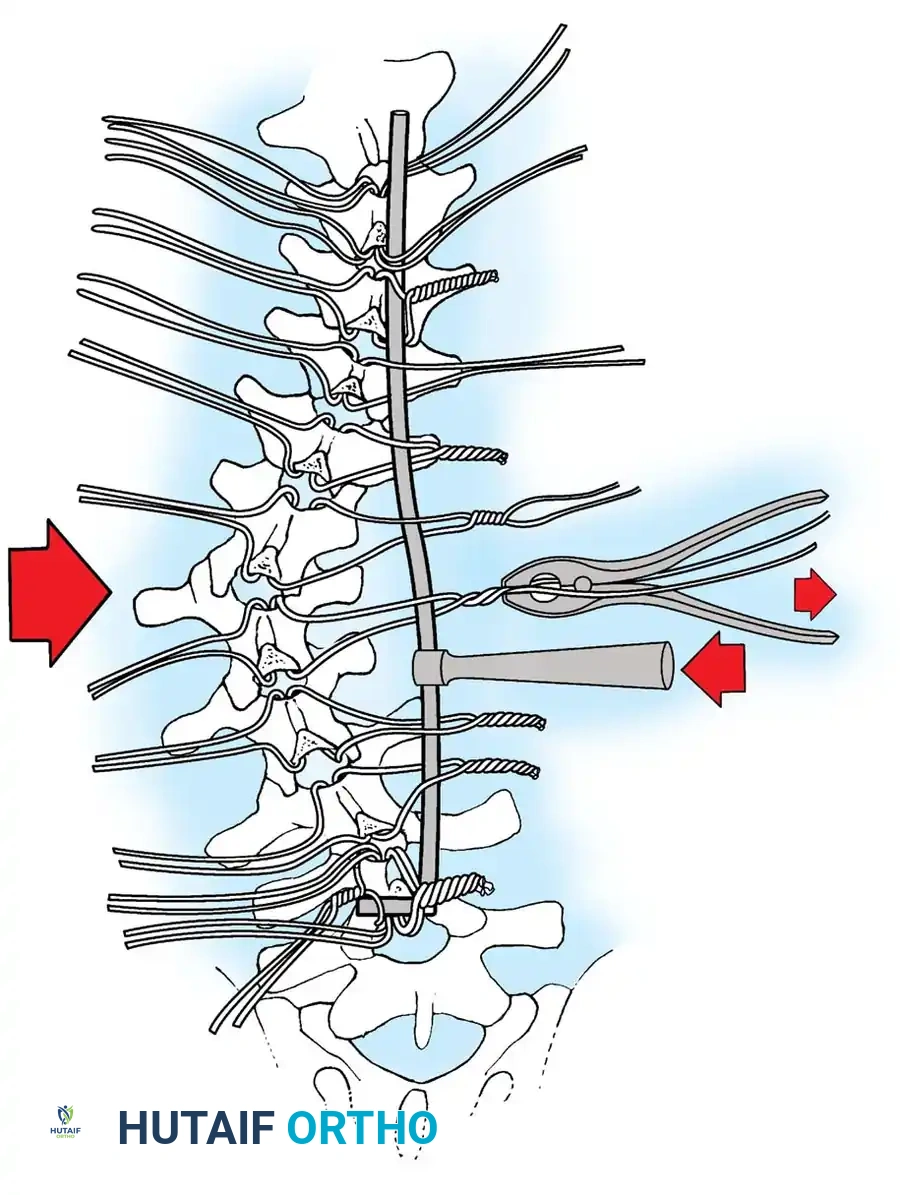
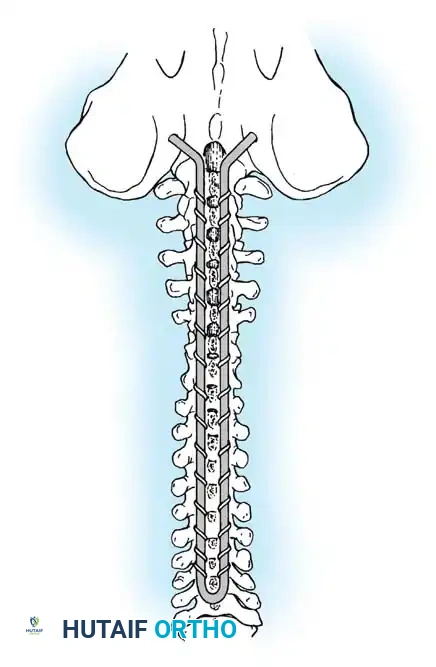
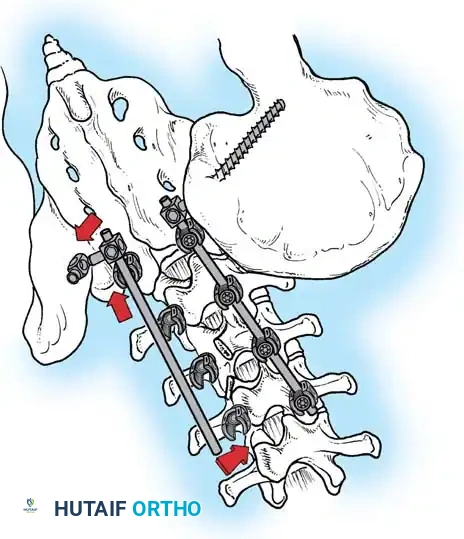
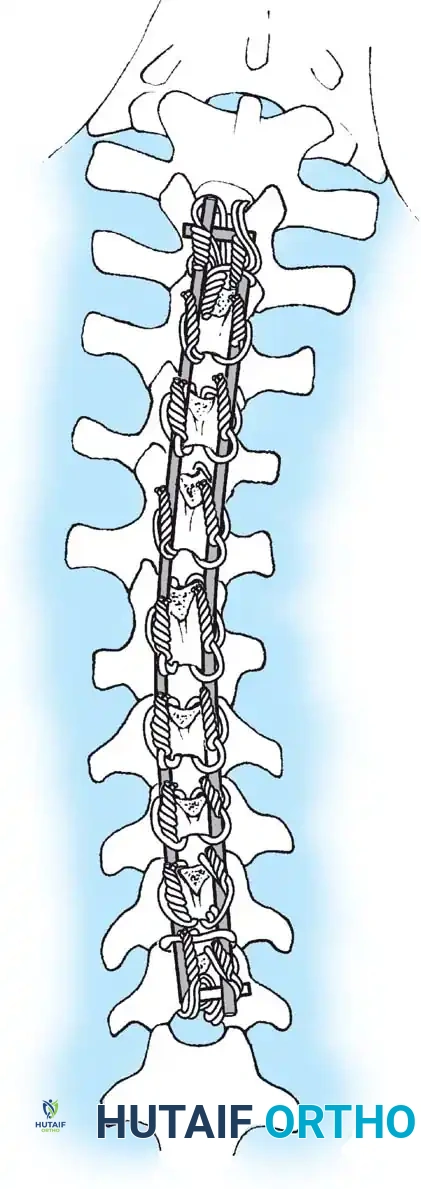
The biomechanics of surgical instrumentation in the neuromuscular spine must account for these extreme forces acting upon osteopenic bone. Modern constructs rely on the principle of load-sharing and multi-point fixation. To achieve adequate pull-out strength, the surgeon must utilize a high density of anchors. While pedicle screws provide superior three-dimensional control, their purchase in severely osteopenic bone may be tenuous. Consequently, sublaminar wires or modern ultra-high-molecular-weight polyethylene (UHMWPE) sublaminar bands remain highly relevant, as they distribute translational forces evenly across the laminae and provide excellent resistance to pull-out at the apex of the deformity. At the distal foundation, the evolution of pelvic fixation—from the historical Galveston technique to traditional iliac screws, and currently to S2 Alar-Iliac (S2AI) screws—reflects a continuous effort to optimize the biomechanical anchor point, minimizing implant prominence while maximizing resistance to the massive cantilever forces exerted by the long spinal lever arm.
Exhaustive Indications and Contraindications
The decision to proceed with major spinal reconstruction in a profoundly impaired neuromuscular patient is one of the most complex clinical judgments in orthopedic surgery, requiring a careful balancing of surgical morbidity against the natural history of the disease. The primary indication for operative intervention is a progressive spinal deformity that compromises the patient's functional status, sitting balance, or physiological well-being. Specifically, curves exceeding 50 degrees that are progressing despite maximal orthotic management are generally considered for surgery. In non-ambulatory patients, the loss of independent sitting balance is a critical threshold; when a patient requires the use of their upper extremities merely to prop themselves up (the "tripod" sign), their ability to interact with their environment is severely curtailed. Furthermore, progressive pelvic obliquity exceeding 15 degrees, the development of pressure sores over the ischial tuberosities, and documented deterioration in pulmonary function directly attributable to the collapsing thoracic cage are absolute indications for surgical stabilization.
Non-operative management, primarily in the form of custom-molded Thoracolumbosacral Orthoses (TLSO) or specialized wheelchair seating matrices, serves a strictly temporizing role. While bracing is completely ineffective at permanently halting curve progression in neuromuscular scoliosis, it is judiciously utilized in very young patients to slow the rate of deterioration, thereby allowing for further spinal and thoracic growth before definitive fusion becomes mandatory. However, once the curve magnitude and rigidity surpass the control of an orthosis, or if the brace causes unacceptable skin maceration and respiratory restriction, surgical intervention must be instituted promptly to prevent the deformity from becoming rigid and inoperable.
Contraindications to neuromuscular spinal surgery are largely driven by the patient's medical fragility and the unacceptably high risk of perioperative mortality. Severe, uncorrectable malnutrition (e.g., serum albumin < 3.0 g/dL, total lymphocyte count < 1500 cells/mm³) is an absolute contraindication until nutritional status is optimized, typically via a gastrostomy tube. End-stage cardiomyopathy, frequently seen in advanced Duchenne muscular dystrophy, precludes safe anesthetic induction. From a pulmonary standpoint, a Forced Vital Capacity (FVC) of less than 20-30% of predicted normal is a strong relative contraindication unless the family and surgical team have explicitly planned for a postoperative tracheostomy and long-term mechanical ventilation.

Ethical considerations also play a profound role in determining contraindications. In profoundly cognitively impaired patients with a limited life expectancy, where a large spinal curve does not hinder nursing care, hygiene, or their baseline level of comfort, observation may be the most humane and medically appropriate course of action. The surgeon must engage in extensive, frank discussions with the patient's family regarding the goals of care, ensuring that the immense physiological trauma of a major spinal reconstruction aligns with the overall palliative or functional objectives for the patient.
Indications and Contraindications Summary
| Category | Specific Criteria | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Curve >50° with documented progression | High risk of continued collapse and cardiopulmonary compromise. |
| Loss of sitting balance / "Tripod" sitting | Loss of upper extremity function due to need for truncal support. | |
| Pelvic obliquity >15° with ischial pressure sores | Imminent risk of deep tissue infection, osteomyelitis, and sepsis. | |
| Relative Indications | Pulmonary decline directly linked to deformity | Stabilization may prevent further restrictive lung disease progression. |
| Intractable truncal or costopelvic impingement pain | Palliative relief of pain caused by ribs resting on the iliac crests. | |
| Absolute Contraindications | Severe, unoptimized malnutrition (Albumin <3.0) | Unacceptable risk of catastrophic wound dehiscence and deep SSI. |
| End-stage cardiomyopathy (LVEF <30%) | Prohibitive risk of intraoperative cardiac arrest during induction/surgery. | |
| Active systemic infection or untreated osteomyelitis | Guaranteed seeding of the massive spinal hardware construct. | |
| Relative Contraindications | FVC < 20-30% of predicted without trach plan | High likelihood of failure to extubate and postoperative ARDS. |
| Profound cognitive impairment with no care difficulties | The morbidity of surgery outweighs the negligible functional benefit. |
Pre-Operative Planning, Templating, and Patient Positioning
The physiological toll of a major posterior spinal fusion extending to the pelvis in a neuromuscular patient cannot be overstated; it is a massive physiological insult. Therefore, a rigorous, multidisciplinary preoperative optimization protocol is absolutely mandatory. Pulmonary evaluation is the cornerstone of this process. Most NMS patients exhibit restrictive lung disease secondary to the collapsing thoracic cage and intercostal muscle weakness. Preoperative pulmonary function tests (PFTs), specifically Forced Vital Capacity (FVC) and Forced Expiratory Volume in 1 second (FEV1), must be obtained if the patient is cognitively capable of cooperating. Historical data demonstrates that patients with an FVC of less than 30% of predicted normal are at a critically high risk for prolonged postoperative respiratory failure. In patients with severe bulbar dysfunction and an absent voluntary cough reflex, a planned postoperative tracheostomy or prolonged nasotracheal intubation must be coordinated with the pediatric intensive care unit (PICU) well in advance.

Nutritional and gastrointestinal optimization is equally critical. Malnutrition is rampant in this population due to uncoordinated swallowing, severe gastroesophageal reflux disease (GERD), and chronic constipation. Because surgery exponentially increases metabolic demand, preoperative hyperalimentation is frequently required. The placement of a preoperative gastrostomy tube (G-tube) combined with a Nissen fundoplication should be strongly considered in malnourished patients to improve serum albumin and prealbumin levels, enhance postoperative wound healing, and prevent catastrophic postoperative aspiration pneumonia. Hematologically, blood conservation strategies must be meticulously planned. Neuromuscular spinal surgery is notoriously bloody due to the extensive subperiosteal exposures required, the highly vascular osteopenic bone, and altered vasomotor tone. Intraoperative strategies must include the use of a cell saver, meticulous bipolar electrocautery, hypotensive anesthesia (if tolerated neurologically), and the administration of modern antifibrinolytics, specifically high-dose Tranexamic Acid (TXA).
Radiographic evaluation and surgical templating dictate the biomechanical success of the operation. Standard imaging includes standing or sitting full-length posteroanterior (PA) and lateral radiographs. Supine traction films or bending films are critical to assess the flexibility of the curve and to differentiate between fixed and flexible pelvic obliquity. Determining the Upper Instrumented Vertebra (UIV) and Lower Instrumented Vertebra (LIV) requires careful calculation. In neuromuscular curves, fusions must routinely extend proximally to T4 or higher; stopping in the mid-thoracic spine carries an unacceptably high risk of cephalad progression ("adding on") and the development of severe proximal junctional kyphosis (PJK). Distally, if bending or traction films reveal more than 10 to 15 degrees of L4 or L5 tilt relative to the interiliac crest line, or if the patient is a non-ambulator with fixed spinopelvic obliquity, the fusion must definitively extend to the pelvis.
Patient positioning in the operating room is a highly orchestrated procedure that directly impacts surgical exposure and complication rates. Patients are typically positioned prone on a specialized spinal frame, such as a Jackson table, which allows the abdomen to hang completely free. This is vital to reduce intra-abdominal pressure, which in turn decreases epidural venous engorgement and minimizes intraoperative blood loss. All bony prominences must be meticulously padded to prevent iatrogenic pressure necrosis, a task made exceedingly difficult by the severe joint contractures common in spastic quadriplegia. Intraoperative neuromonitoring, utilizing Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs), is standard of care. However, the surgeon must be aware that baseline signals may be severely degraded or entirely absent due to the underlying neuromuscular pathology, occasionally necessitating reliance on a Stagnara wake-up test, provided the patient is cognitively capable of following commands.
Step-by-Step Surgical Approach and Fixation Technique
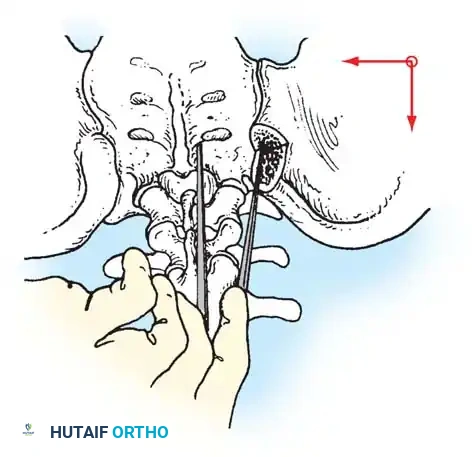
The surgical approach for neuromuscular scoliosis reconstruction demands meticulous technique and an acute awareness of the patient's physiological fragility. A standard midline longitudinal incision is made, extending from the predetermined UIV down to the sacrum. Meticulous, segmental subperiosteal dissection is performed to expose the posterior elements, utilizing a combination of Cobb elevators and electrocautery. In neuromuscular patients, the paraspinal soft tissues are often heavily fibrotic and interspersed with fatty infiltration, while the underlying bone is profoundly osteopenic. Hemostasis must be rigorously maintained at every step using bipolar cautery, bone wax, and topical hemostatic agents (e.g., thrombin-soaked Gelfoam) to mitigate the massive blood loss characteristic of these procedures. Complete, radical facetectomies are performed at every level within the fusion construct. This serves a dual purpose: it significantly mobilizes the rigid spine to facilitate deformity correction, and it provides a highly vascularized, decorticated bed essential for achieving a robust posterior fusion mass.
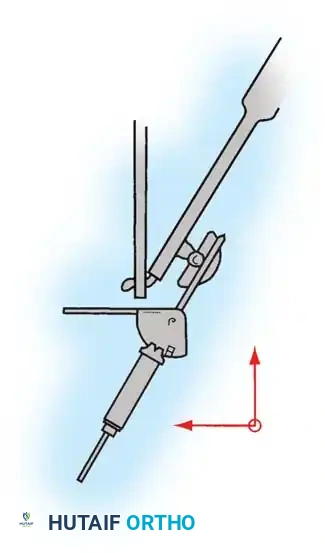
Instrumentation strategies in the neuromuscular spine must overcome the inherent poor bone stock. The modern gold standard involves rigid, dual-rod constructs utilizing a high density of pedicle screws, supplemented by hooks and sublaminar fixation where appropriate. Pedicle screw insertion in dysplastic, osteopenic vertebrae requires precise trajectory planning, often aided by intraoperative fluoroscopy or advanced robotic navigation. To maximize pull-out strength, surgeons may employ techniques such as under-tapping the pedicle, utilizing larger diameter screws, or employing polymethylmethacrylate (PMMA) cement augmentation in severely osteoporotic levels. In cases where pedicle anatomy precludes safe screw placement, sublaminar wires or modern UHMWPE sublaminar bands (following the principles pioneered by Luque) remain highly effective. These bands provide exceptional pull-out resistance and distribute translational corrective forces evenly across the apical laminae, minimizing the risk of iatrogenic laminar fracture during reduction.
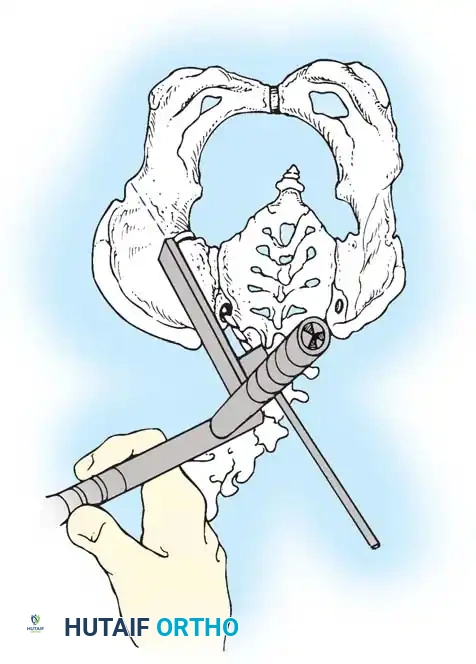
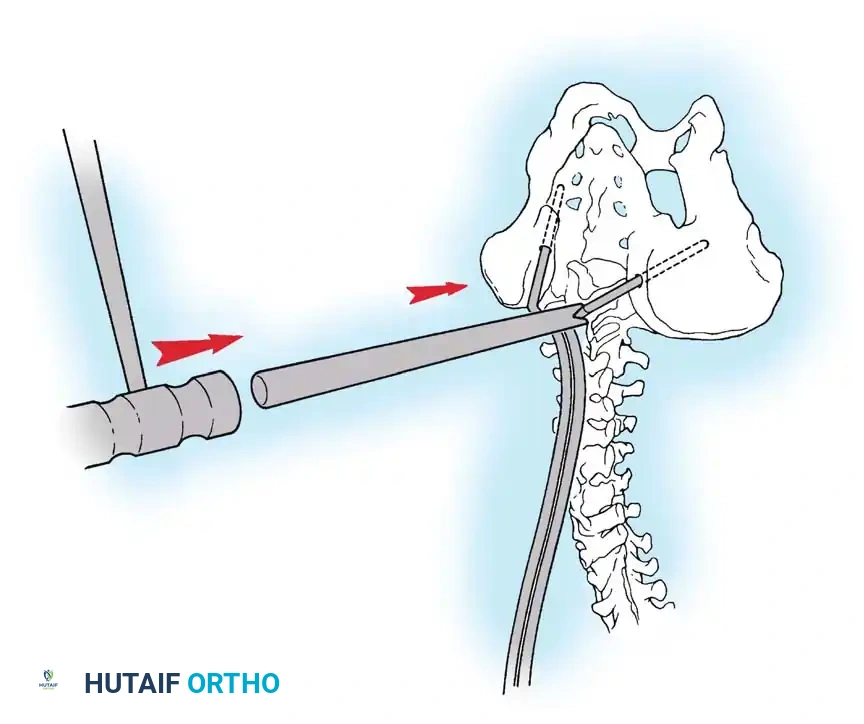
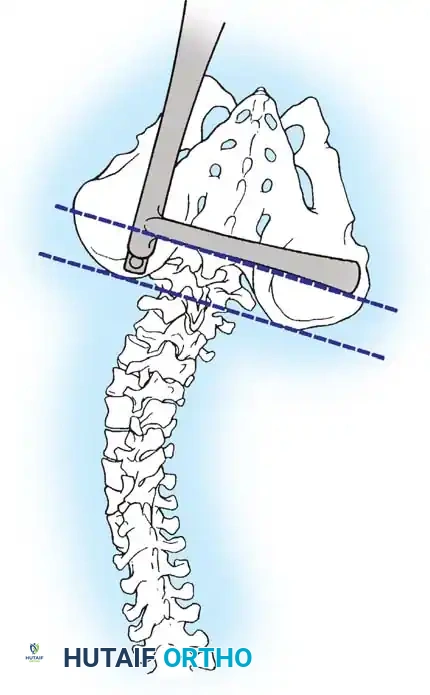
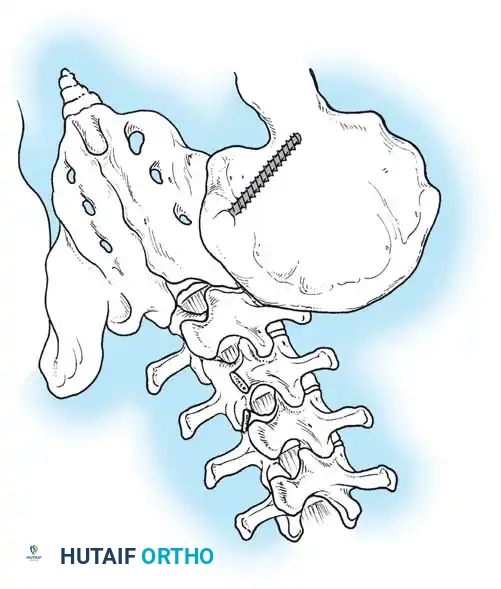
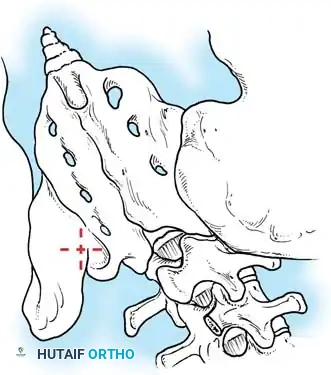
Achieving rigid pelvic fixation is arguably the most critical step in non-ambulatory patients with severe pelvic obliquity. The historical Galveston technique, which involved driving the primary rod directly into the ilium, has largely been superseded by modular systems. Traditional iliac screws provide excellent biomechanical purchase but require extensive lateral dissection and are prone to symptomatic prominence over the iliac crest. Currently, the S2 Alar-Iliac (S2AI) screw technique is widely favored. S2AI screws traverse the S2 pedicle, cross the sacroiliac joint, and anchor deep within the iliac wing. This trajectory offers immense biomechanical strength, requires less lateral soft tissue dissection, and perfectly aligns the screw head with the proximal spinal construct, eliminating the need for complex offset connectors and significantly reducing implant prominence.

Deformity correction maneuvers in neuromuscular scoliosis prioritize global coronal and sagittal balance over absolute curve eradication. The surgeon typically employs a combination of cantilever reduction, rod derotation, and direct translation techniques. The pre-contoured rods are sequentially seated into the anchors, utilizing the immense lever arm of the long construct to slowly correct the pelvic obliquity and restore physiological lumbar lordosis. Maintaining lumbar lordosis is paramount; it ensures that the patient's body weight is distributed equally beneath the ischial tuberosities and posterior thighs when seated, drastically reducing the risk of sacral pressure sores. Once correction is achieved and the construct is definitively tightened, meticulous decortication of the posterior elements is performed. Copious amounts of bone graft—comprising local autograft from the facetectomies, structural allograft, and often osteoinductive agents such as Bone Morphogenetic Protein-2 (BMP-2)—are packed into the facet joints and along the decorticated laminae to ensure a solid, durable arthrodesis.
Complications, Incidence Rates, and Salvage Management
The complication profile for surgical intervention in neuromuscular scoliosis is drastically higher than that observed in adolescent idiopathic scoliosis, directly reflecting the profound medical fragility of this patient population. Surgical Site Infection (SSI) is one of the most devastating and frequent complications, with reported incidence rates ranging from 10% to over 15%. The etiology of SSI in NMS is multifactorial, driven by poor nutritional status, extensive soft tissue dissection, and a high rate of fecal incontinence leading to contamination of the distal incision with Gram-negative enteric organisms (e.g., Escherichia coli, Pseudomonas aeruginosa). Prevention strategies are paramount and include optimization of preoperative albumin, rigorous bowel regimens, the application of intrawound vancomycin powder, and utilizing plastic surgery colleagues for complex, multilayered soft tissue closures. When a deep SSI occurs, salvage management mandates immediate, aggressive operative irrigation and debridement, retention of the hardware (unless grossly loose), and prolonged culture-directed intravenous antibiotic therapy, often coordinated with infectious disease specialists.
Pulmonary and medical complications represent the leading cause of perioperative mortality. Pneumonia, acute respiratory distress syndrome (ARDS), and failure to extubate occur in up to 20% of patients, particularly those with a preoperative FVC below 30%. The inability to clear secretions due to an absent cough reflex necessitates aggressive pulmonary toilet, including mechanical insufflation-exsufflation (CoughAssist) devices and frequent bronchoscopies. Venous thromboembolism (VTE) is another significant risk, exacerbated by prolonged operative times and postoperative immobility; thus, mechanical and chemical prophylaxis must be judiciously managed. Gastrointestinal complications, including prolonged ileus and superior mesenteric artery (SMA) syndrome, though less common than in AIS, require vigilant monitoring and prompt management with nasogastric decompression and parenteral nutrition if enteral feeding fails.
Hardware failure and pseudarthrosis are significant long-term risks due to the massive biomechanical forces exerted on the construct and the poor healing potential of osteopenic bone. Rod breakage typically occurs at the lumbosacral junction, the area of maximal biomechanical stress, particularly if a solid anterior column support was not achieved or if the patient has persistent, unaddressed hip contractures. Proximal Junctional Kyphosis (PJK) and distal pull-out are also frequent modes of failure. Salvage management for pseudarthrosis and hardware failure requires complex revision surgery. This involves thorough exploration of the fusion mass, removal of broken implants, extension of the fusion construct proximally or distally to achieve stable fixation, and massive augmentation with structural allograft and BMP-2 to stimulate robust osteogenesis.

Neurologic complications, while less frequent than medical complications, are catastrophic. Ischemic spinal cord injury can result from over-distraction of the spinal column, direct iat
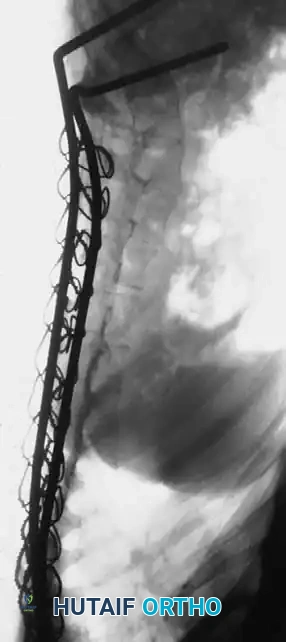
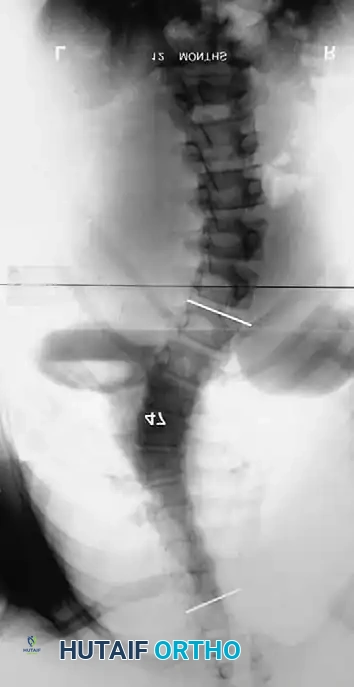
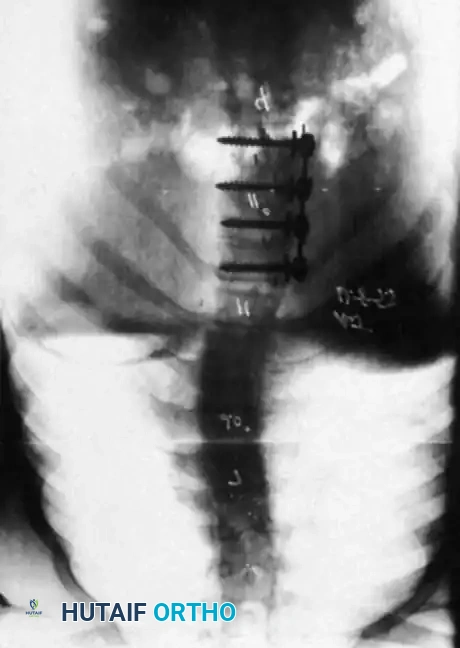
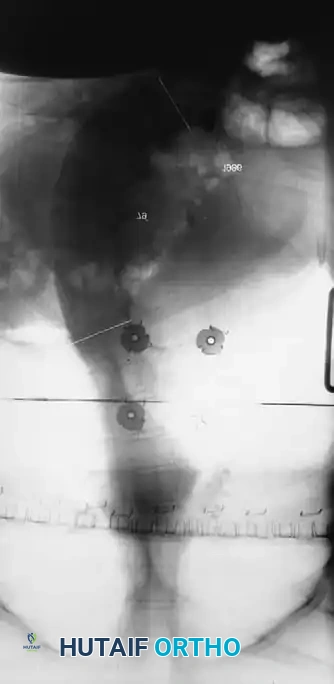
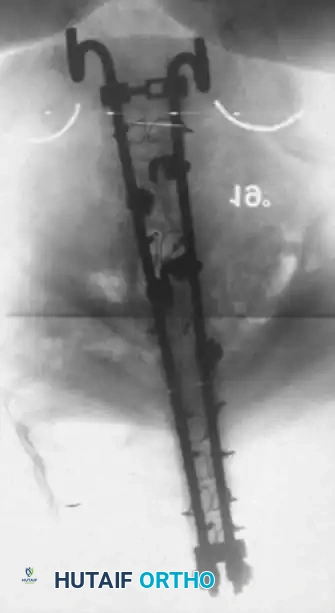
Clinical & Radiographic Imaging Archive