Metacarpophalangeal Joint Arthroplasty: Swanson Technique
Key Takeaway
Metacarpophalangeal (MCP) joint arthroplasty utilizing the Swanson silicone implant remains the gold standard for advanced rheumatoid arthritis with joint destruction and instability. This procedure acts as a dynamic spacer, relying on encapsulation for stability. Key steps include metacarpal head resection, comprehensive synovectomy, intramedullary canal preparation, soft tissue balancing via ulnar intrinsic release, and meticulous extensor mechanism centralization to restore functional alignment and alleviate pain.
INTRODUCTION TO METACARPOPHALANGEAL JOINT ARTHROPLASTY
Metacarpophalangeal (MCP) joint arthroplasty is a cornerstone procedure in the surgical rehabilitation of the severely arthritic hand. Originally pioneered by Alfred Swanson in the 1960s, the silicone elastomer implant was designed not as a rigid joint replacement, but as a flexible, dynamic spacer. The fundamental biomechanical principle of the Swanson implant relies on the concept of "encapsulation." The implant maintains joint alignment and provides a scaffold around which a new, functional fibrous capsule forms.
Unlike rigid kinematic prostheses, the silicone stems are designed to glide slightly within the medullary canals of the metacarpal and proximal phalanx—a phenomenon known as "pistoning." This controlled micromotion distributes mechanical stress across the implant, significantly reducing the risk of hinge fracture and preserving the integrity of the surrounding bone stock.
Pathoanatomy of the Rheumatoid MCP Joint
Understanding the pathoanatomy of the rheumatoid hand is critical for successful surgical reconstruction. Chronic synovitis leads to the distension of the joint capsule and attenuation of the collateral ligaments and sagittal bands. As the radial sagittal band stretches, the extensor digitorum communis (EDC) tendon subluxates into the ulnar valleys between the metacarpal heads.
Once the extensor tendon subluxates ulnarly, it loses its mechanical advantage for extending the proximal phalanx and instead becomes a deforming force, exacerbating ulnar deviation. Concurrently, volar plate laxity and the unopposed pull of the intrinsic muscles lead to volar subluxation of the proximal phalanx. The surgical objective of MCP joint arthroplasty is not merely to insert an implant, but to comprehensively correct these complex soft-tissue imbalances.
Clinical Pearl: Surface replacement arthroplasty is strictly reserved for patients with stable metacarpal joints, such as those with osteoarthritis or posttraumatic arthritis where the collateral ligaments and volar plates remain intact. Because rheumatoid arthritis inherently involves severe joint instability and dislocation, surface replacement is contraindicated. The Swanson silicone arthroplasty remains the gold standard for the rheumatoid hand.
PREOPERATIVE PLANNING AND INDICATIONS
Indications
- Rheumatoid Arthritis: Severe pain, fixed volar subluxation, and uncorrectable ulnar drift of the MCP joints.
- Systemic Lupus Erythematosus (SLE): Advanced joint destruction with fixed deformities.
- Posttraumatic Arthritis: Cases where severe bone loss or ligamentous destruction precludes surface replacement or arthrodesis.
- Osteoarthritis: Advanced cases with significant deformity where arthrodesis is undesirable.
Contraindications
- Active local or systemic infection.
- Inadequate bone stock to support the implant stems.
- Irreparable rupture of the extensor mechanism (unless concurrent tendon transfers are planned).
- Lack of patient compliance for the rigorous postoperative rehabilitation protocol.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Patient Positioning and Anesthesia
The procedure is typically performed under regional anesthesia (brachial plexus block) or general anesthesia. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
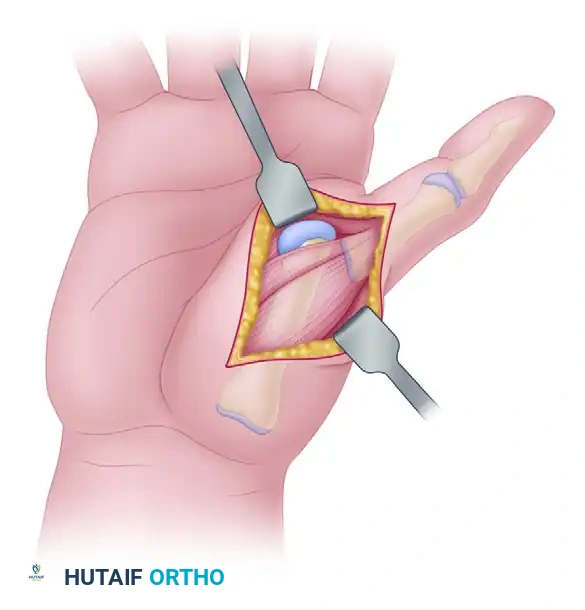
2. Surgical Approach and Incision
- Transverse Incision: Make a transverse incision on the dorsum of the hand, beginning on the radial aspect of the second MCP joint and extending ulnarward to the ulnar aspect of the fifth MCP joint. This approach provides excellent cosmetic results and comprehensive access to all four joints.
- Longitudinal Incision Alternative: Alternatively, two longitudinal incisions may be utilized—one placed between the index and middle fingers, and the second between the ring and small fingers.
- Vein Preservation: Carefully observe the pattern of the superficial dorsal venous network. Preserve the longitudinal veins and the dorsal sensory branches of the radial and ulnar nerves whenever possible to prevent postoperative edema and neuromas.
- Flap Elevation: The transverse incision permits the creation of a slight dorsal flap. Dissect this flap proximally and fold it back to expose the metacarpal heads and the extensor mechanism.
3. Extensor Mechanism Management and Arthrotomy
Through the exposure, identify the extensor mechanism. In the rheumatoid hand, the extensor tendons are typically subluxated ulnarly.
* Incise the shroud ligament (sagittal band) of the extensor mechanism on the radial aspect of each joint. If severe contracture is present, an ulnar incision may also be necessary.
* Reflect the extensor tendon ulnarly to permit entry into the joint capsule.
* Note that in advanced rheumatoid disease, the dorsal capsule may already be ruptured, presenting with herniation of hypertrophied, invasive synovium.
4. Synovectomy and Bone Resection
- Capsulotomy: Incise the capsule longitudinally.
- Synovectomy: Perform a meticulous synovectomy using small rongeurs. It is critical to perform synovectomy both before and after metacarpal head resection to ensure all invasive pannus is removed from the volar recesses.
- Metacarpal Head Resection: Utilizing a thin oscillating saw or a sharp bone-biting instrument, resect each metacarpal head.
- Crucial Angle: The metacarpal head-neck region must be cut precisely at a 90-degree angle relative to the longitudinal axis of the metacarpal shaft.
- Shortening: Resect sufficient bone to permit easy, tension-free reduction of the dislocated joint.
- Ligament Considerations: Adequate shortening may require resection proximal to the origin of the collateral ligaments. If this occurs, radial collateral ligament repair or reconstruction becomes mandatory to ensure postoperative stability.
Surgical Warning: Inadequate bone resection is a primary cause of implant failure. If the joint remains tight, the silicone hinge will be subjected to excessive compressive forces during flexion, leading to premature buckling, hinge fracture, and restricted range of motion.
5. Intramedullary Canal Preparation
- Metacarpal Preparation: Introduce a sharp awl into the metacarpal medullary canal to establish the entry point. Follow this with sequential manual reamers or broaches to create adequate space for the proximal stem of the prosthesis.
- Proximal Phalanx Preparation: Do not resect the base of the proximal phalanx. Resection removes dense subchondral bone necessary for stem support. However, if severe deformity from the arthritic process exists, minor recontouring may be required to ensure the base is perpendicular to the phalangeal shaft.
- Volar Perforation Avoidance: Perform sufficient soft tissue dissection from the proximal phalangeal base to clearly visualize the articular surface. The entry point for the awl must be perfectly centered medial-to-lateral, but positioned more dorsal than volar. The proximal phalanx has a natural volar bow; a centralized or volar starting point frequently results in iatrogenic perforation of the volar cortex.
- Prepare the phalangeal base using appropriate drilling, reaming, and broaching to accept the distal stem.
6. Soft Tissue Balancing and Ligament Reconstruction
Soft tissue balancing is as critical as the bony preparation.
* Ulnar Intrinsic Release: Evaluate the joint for intrinsic tightness. If the MCP joint deviates ulnarly when held in full extension, an ulnar intrinsic release is mandatory. This is commonly required in rheumatoid arthritis patients, particularly for the ring and small fingers.
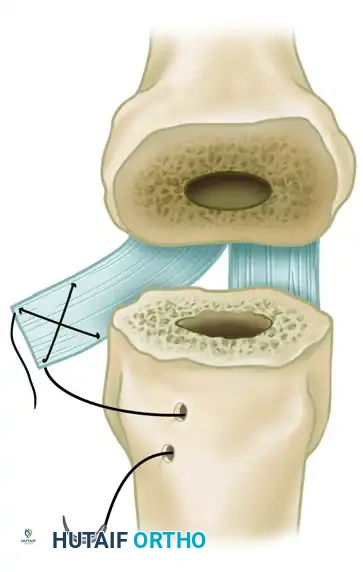
* Index Finger Radial Collateral Ligament Reconstruction (Swanson Technique): The index finger is uniquely susceptible to pronation deformity and ulnar drift due to pinch kinematics. To correct or prevent index finger pronation, Swanson recommended reconstructing the radial collateral ligament using a slip of the volar plate.
* Split a radial slip of the proximal phalangeal volar plate proximally.
* Reattach this slip to the radial aspect of the metacarpal neck to act as a robust tether against ulnar deviation and pronation.
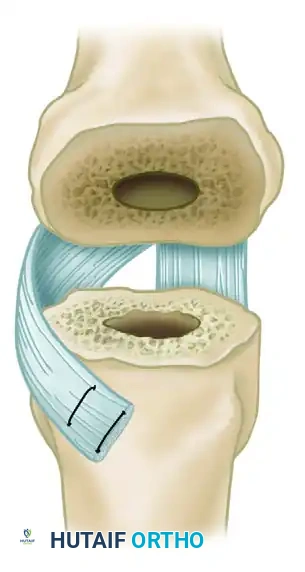
FIGURE 73-25 Swanson technique for reconstruction of radial collateral ligament of index metacarpophalangeal joint by using slip of volar plate.
7. Implant Trialing and Insertion
- Sizing: Select the largest implant that can be inserted comfortably without forcing the stems.
- Trialing: Insert a trial prosthesis. Place gentle traction on the finger with the MCP joint in full extension. Examine the distance between the metacarpal cut surface and the phalangeal base; there must be sufficient space to accommodate the implant's midsection hinge without impingement.
- Kinematic Check: Passively move the joint from full extension to almost 90 degrees of flexion. Ensure there is no prosthesis buckling or bony abutment. Check all fingers simultaneously for overall alignment, cascade, and absence of rotary deformity.
- Implant Handling: Remove the definitive silicone prosthesis from its packaging only after the exact size has been determined. Handle the prosthesis exclusively with blunt instruments. Sharp edges, forceps with teeth, or aggressive handling will score the silicone, creating stress risers that inevitably lead to premature implant fracture.
- Insert the definitive implants using a no-touch technique.
8. Closure and Extensor Centralization
- Capsular Closure: Close any remaining viable dorsal capsule over the prosthesis to provide a tissue barrier between the implant and the extensor tendons.
- Extensor Centralization: Centralize the extensor tendon over the dorsal midline of the MCP joint. This is achieved by reefing (imbricating) the radial sagittal band. If the ulnar sagittal band is excessively tight, it may be released or lengthened to prevent recurrent ulnar subluxation of the tendon.
- Wound Closure: Deflate the tourniquet and achieve meticulous hemostasis. Insert a small closed-suction drain if necessary. Close the skin with non-absorbable sutures.
- Splinting: Apply a bulky, supportive compressive dressing. Splint the hand with the wrist in 20 degrees of extension, the MCP joints in full extension, and the fingers held in slight radial deviation to counteract the natural tendency for recurrent ulnar drift.
POSTOPERATIVE CARE AND REHABILITATION
The success of a Swanson MCP joint arthroplasty is heavily dependent on strict adherence to a specialized postoperative rehabilitation protocol. The goal is to guide the formation of the encapsulating scar tissue while maintaining mobility and preventing recurrent deformity.
Phase 1: Immediate Postoperative (Days 1 to 10)
- The initial bulky splint and dressing remain intact for 5 to 7 days.
- At the first dressing change, the wound is inspected, and a lighter dressing is applied.
- The fingers must be continuously held in extension and slight radial deviation in a static postoperative splint.
- Sutures are typically removed at 10 to 14 days, depending on the progression of wound healing.
Phase 2: Dynamic Splinting and Active Motion (Weeks 2 to 8)
- Following suture removal, the patient is transitioned to a formal therapy program under the direct supervision of a certified hand therapist.
- Daytime Dynamic Splinting: A dynamic extension outrigger splint is fabricated. This splint utilizes elastic bands to assist MCP joint extension and pull the digits into radial deviation, counteracting the deforming forces of the flexors and intrinsics. The patient performs active flexion exercises against the resistance of the elastic bands.
- Nighttime Static Splinting: At night, the dynamic splint is replaced with a static resting splint that holds the volar wrist in extension, the MCP joints in full extension and radial deviation, and the proximal interphalangeal (PIP) joints in extension.
- The daytime dynamic splint is generally discontinued between 6 to 8 weeks postoperatively, once adequate capsular stability and active extension are achieved.
Phase 3: Maturation and Maintenance (Months 3 and Beyond)
- Supervised hand therapy continues to maximize grip strength and fine motor dexterity.
- The nighttime static resting splint must be continued for a minimum of 3 months postoperatively to prevent late recurrent ulnar drift while the fibrous capsule fully matures.
- Patients are educated on joint protection techniques and advised to avoid heavy lifting or repetitive forceful gripping, which can accelerate implant wear and subsidence.
COMPLICATIONS AND PITFALLS
While highly successful for pain relief and functional restoration, silicone MCP arthroplasty carries specific risks:
1. Implant Fracture: The most common long-term radiographic complication. However, due to the robust fibrous encapsulation, many implant fractures remain entirely asymptomatic and do not require revision unless accompanied by severe recurrent deformity or pain.
2. Recurrent Ulnar Drift: Often results from inadequate ulnar intrinsic release, failure to centralize the extensor mechanism, or non-compliance with postoperative radial-pull dynamic splinting.
3. Infection: Deep infection requires immediate aggressive debridement and removal of the silicone implants. The resultant void is managed as a resection arthroplasty, which still provides a functional, albeit shortened, digit.
4. Silicone Synovitis: A rare inflammatory response to silicone particulate debris, presenting with joint swelling, pain, and cystic bone resorption (osteolysis). This necessitates implant removal and thorough synovectomy.
You Might Also Like