Medial Open Reduction of Developmental Hip Dislocation: An Intraoperative Masterclass

Key Takeaway
This masterclass details the medial open reduction for developmental hip dislocation (DDH) in infants. We cover essential surgical anatomy, meticulous step-by-step intraoperative technique, crucial neurovascular protection, and strategies for achieving stable reduction. Fellows will gain insights into managing potential pitfalls and ensuring optimal postoperative outcomes, including spica cast application and long-term follow-up.
Comprehensive Introduction and Patho-Epidemiology
Developmental Dysplasia of the Hip (DDH) represents a complex spectrum of anatomical abnormalities, ranging from mild acetabular dysplasia to frank, irreducible dislocation of the femoral head. As orthopedic surgeons, our fundamental objective in managing DDH is the achievement and maintenance of a concentric, stable reduction to provide the optimal mechanical environment for normal hip development. The incidence of DDH is generally reported as 1.5 to 20 per 1,000 live births, heavily dependent on the screening modalities utilized and the geographic population. While early conservative management utilizing dynamic splinting (e.g., the Pavlik harness) demonstrates remarkable efficacy—often exceeding 90% in dysplastic hips and 80% in dislocated hips—a subset of patients will present with refractory instability or late-diagnosed fixed dislocations. It is in this specific cohort that the medial open reduction becomes an indispensable weapon in the pediatric orthopedic armamentarium.
The pathogenesis of DDH is multifactorial, intertwining mechanical, genetic, and hormonal variables. Mechanical factors such as breech presentation, oligohydramnios, and primiparity create a restrictive intrauterine environment that forces the fetal hips into sustained adduction and extension, predisposing the joint to instability. Hormonally, maternal relaxin crosses the placenta, inducing transient ligamentous laxity in the infant, which is particularly pronounced in females—accounting for the significant female-to-male predilection (approximately 4:1). Genetically, familial hyperlaxity syndromes and a positive family history strongly correlate with an increased risk profile. It remains imperative to clinically differentiate idiopathic DDH from teratologic dislocations, such as those observed in arthrogryposis multiplex congenita, Larsen syndrome, or myelomeningocele, as teratologic hips harbor severe, rigid contractures that often necessitate more aggressive, alternative surgical strategies.
Clinical evaluation of the infant hip requires a meticulous and nuanced physical examination. The Ortolani maneuver (elevation and abduction) evaluates for the reduction of a dislocated hip, yielding a palpable "clunk" as the femoral head traverses the posterior acetabular rim. Conversely, the Barlow maneuver (adduction and posterior force) assesses for the dislocatability of a reduced hip. As the infant ages and the dislocation becomes fixed, these classic signs fade, replaced by secondary indicators of pathology. Restricted passive abduction becomes the most reliable clinical hallmark, driven by progressive adductor contracture. The Galeazzi sign reveals apparent femoral shortening on the affected side due to proximal migration of the femoral head, though it is notoriously absent in bilateral presentations. Additional findings, such as asymmetric thigh or gluteal folds and a positive Klisic test, further corroborate the diagnosis.
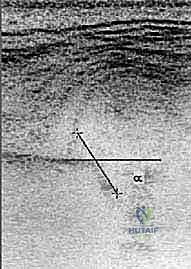
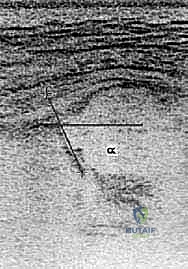
Imaging serves as the definitive cornerstone for both diagnosis and pre-operative surgical planning. In infants under 4 to 6 months of age, before the capital femoral epiphysis ossifies, dynamic ultrasound is the gold standard. The Graf classification system utilizes the alpha angle (quantifying the bony acetabular roof, normal >60 degrees) and the beta angle (quantifying the cartilaginous roof, normal <55 degrees) to stratify dysplasia severity. Beyond 6 months, the anteroposterior (AP) pelvic radiograph becomes paramount. We meticulously analyze the disruption of Shenton’s line, the lateralization of the proximal femoral metaphysis relative to Perkins' line, and the elevation of the acetabular index (Hilgenreiner’s angle). The presence and symmetry of the ossific nucleus must be scrutinized; while delayed ossification was historically considered a contraindication to early surgery due to theoretical avascular necrosis (AVN) risks, contemporary consensus favors proceeding with timely reduction to optimize acetabular remodeling potential.

Detailed Surgical Anatomy and Biomechanics
The medial approach to the pediatric hip, initially popularized by Ludloff and later modified by Ferguson, Weinstein, and Ponseti, offers a direct, anatomic trajectory to the primary impediments of hip reduction. Unlike the anterior Smith-Petersen approach, the medial approach avoids splitting the iliac apophysis, spares the abductor musculature, and provides unparalleled access to the inferior capsule and iliopsoas tendon. Understanding the intricate three-dimensional anatomy of the medial thigh is non-negotiable for executing this procedure safely and effectively. The surgical corridor is defined by the adductor musculature, specifically navigating the intervals between the adductor longus, adductor brevis, and pectineus.
The primary biomechanical obstacles to a concentric reduction in DDH are predominantly soft-tissue constraints that have adapted to the chronically dislocated state. The iliopsoas tendon, acting as a powerful hip flexor, becomes tautly stretched across the anterior and inferior aspects of the joint capsule as the femoral head migrates superiorly. This creates a severe "hourglass" constriction of the capsule, physically blocking the reentry of the femoral head. Within the acetabulum itself, the fibrofatty pulvinar hypertrophies, occupying the true joint space. The transverse acetabular ligament (TAL), which normally spans the inferior acetabular notch, becomes contracted and hypertrophied, acting as a rigid sling that prevents the femoral head from seating deeply. Furthermore, the ligamentum teres elongates and thickens, while the acetabular labrum may invert, acting as a mechanical doorstop.
Navigating the medial anatomy requires profound respect for the regional neurovascular structures, most notably the Medial Femoral Circumflex Artery (MFCA). The MFCA is the dominant, and often sole, blood supply to the developing capital femoral epiphysis. It originates from the deep femoral artery (profunda femoris) and courses posteriorly, passing precisely between the pectineus and the iliopsoas tendon—the exact interval we operate within. Iatrogenic injury to the MFCA or its retinacular branches during capsulotomy or psoas release is the primary etiology of postoperative avascular necrosis (AVN). The surgeon must maintain a meticulous plane, staying strictly on the anterior capsule and avoiding blind dissection posteriorly or laterally where the extracapsular arterial ring resides.
The muscular topography serves as our roadmap. The adductor longus, originating from the anterior body of the pubis, is the most superficial and easily palpable landmark. Deep and slightly superior to the adductor longus lies the pectineus, while the adductor brevis lies directly deep to the longus. The femoral neurovascular bundle (femoral vein, artery, and nerve, from medial to lateral) lies anterior and lateral to the pectineus. The medial approach strategically passes posterior to the pectineus and the neurovascular bundle, utilizing the internervous plane between the obturator nerve (supplying the adductors) and the femoral nerve (supplying the pectineus and anterior compartment).
Exhaustive Indications and Contraindications
The decision to proceed with a medial open reduction requires a judicious evaluation of the patient's age, prior treatment history, and the specific pathoanatomy of the dislocation. The medial approach is widely considered the procedure of choice for children between the ages of 6 and 18 months who have failed conservative management (e.g., Pavlik harness, rigid abduction orthoses) or who have failed a previous attempt at closed reduction and spica casting. In this age demographic, the primary barriers to reduction are soft-tissue contractures rather than severe bony dysplasia. The medial approach allows for direct release of the psoas and inferior capsule with minimal blood loss and excellent cosmetic outcomes.
However, the medial approach has distinct limitations that dictate its contraindications. Because the approach accesses the hip inferiorly, it does not allow for a formal capsulorrhaphy (capsular plication) to eliminate redundant superior capsular volume. Therefore, in children older than 18 to 24 months, where the capsule is excessively capacious and bony remodeling potential is waning, an anterior approach is generally preferred. The anterior approach permits a robust capsulorrhaphy and provides the necessary exposure if a concomitant pelvic osteotomy (e.g., Salter or Pemberton) is required to address severe acetabular dysplasia.
Teratologic dislocations present a unique challenge. While the medial approach can be utilized in certain syndromic patients, the severe, rigid nature of teratologic contractures often necessitates a more extensile anterior or anterolateral approach to achieve adequate release and reduction. Furthermore, if pre-operative imaging suggests the need for femoral shortening osteotomy to decompress the joint and mitigate AVN risk, the medial approach is insufficient, and a combined anterior and lateral approach is mandated.
| Parameter | Indications for Medial Open Reduction | Contraindications for Medial Open Reduction |
|---|---|---|
| Patient Age | Typically 6 to 18 months (up to 24 months in select cases). | Generally > 24 months (due to need for capsulorrhaphy/osteotomy). |
| Previous Treatment | Failed Pavlik harness; failed closed reduction. | Need for concurrent pelvic or femoral osteotomy. |
| Pathoanatomy | Idiopathic DDH with primary soft-tissue barriers (psoas, TAL, pulvinar). | Severe superior capsular redundancy requiring plication. |
| Syndromic Status | Typical (idiopathic) developmental dislocation. | Severe teratologic dislocations (relative contraindication). |
| Surgical Goals | Concentric reduction, psoas release, clearing of acetabulum. | Requirement for open reduction and bony reconstruction. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the bedrock of a successful medial open reduction. The surgeon must comprehensively review all available imaging, transitioning from early ultrasounds to recent AP and frog-leg lateral pelvic radiographs. The degree of superior and lateral migration of the femoral head dictates the anticipated tension on the neurovascular structures during reduction. We must assess the acetabular index to gauge the severity of bony dysplasia; while the medial approach relies on spontaneous remodeling post-reduction, severe dysplasia may prompt a discussion with the family regarding the potential need for future pelvic osteotomies if remodeling is insufficient. The presence, absence, or asymmetry of the capital femoral ossific nucleus should be documented, as it serves as a baseline for postoperative AVN monitoring.
Anesthesia for this procedure requires a highly coordinated effort with a specialized pediatric anesthesiologist. General endotracheal anesthesia with profound neuromuscular blockade is mandatory. Muscle relaxation is critical not only for the surgical exposure but also for minimizing the force required to reduce the hip, thereby decreasing the mechanical pressure on the proximal femoral epiphysis and mitigating the risk of ischemic necrosis.
Patient positioning must facilitate unhindered access, dynamic intraoperative examination, and pristine fluoroscopic imaging. The infant is placed supine on a fully radiolucent operating table. A small gel bump may be placed beneath the ipsilateral hemipelvis to slightly elevate the operative side. Meticulous perineal isolation is achieved using sterile adhesive drapes (e.g., Ioban or equivalent) to seal off the genitalia and anal region, drastically reducing the risk of surgical site infection. The entire lower extremity, from the iliac crest to the toes, is prepped and draped free.
Crucially, the drapes must be secured using sutures or adhesive strips rather than penetrating towel clips. Towel clips placed in the groin or pelvic region create severe radiopaque artifacts that obscure the delicate pediatric bony landmarks during intraoperative fluoroscopy. The C-arm fluoroscopy unit is positioned on the contralateral side of the table, draped sterilely, and brought in for baseline AP and lateral views before the incision is made. The surgeon must confirm that the C-arm can freely rotate to obtain orthogonal views without compromising the sterile field.

Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The procedure commences with the identification of precise anatomic landmarks. The surgeon palpates the origin of the adductor longus tendon at the pubis and locates the femoral arterial pulse laterally. A transverse incision, approximately 3 to 4 centimeters in length, is made just distal to the inguinal crease, centered directly over the palpable adductor longus tendon. This transverse orientation aligns perfectly with Langer’s lines, ensuring an aesthetically superior scar. The subcutaneous tissue is sharply divided to expose the deep fascia overlying the adductor compartment.
The fascia is incised longitudinally, directly over the adductor longus muscle belly. Using blunt retractors, the adductor longus is isolated from the underlying adductor brevis. A right-angle clamp is carefully passed deep to the adductor longus tendon near its pubic origin. A complete tenotomy of the adductor longus is performed using electrocautery or a scalpel. This initial release is a critical first step in overcoming the adductor contracture that frequently accompanies DDH.
Deep Dissection and Interval Identification
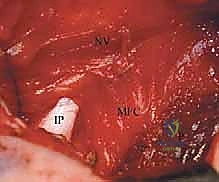
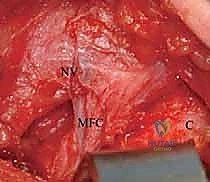
With the adductor longus released and retracted inferiorly, the underlying anatomy comes into view. The key interval in the Weinstein modification of the medial approach lies between the pectineus muscle anteriorly and the adductor brevis muscle posteriorly. The surgeon uses blunt finger dissection or a peanut sponge to develop this areolar plane. It is imperative to stay posterior to the pectineus, as the femoral neurovascular bundle lies directly anterior to it.
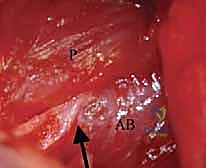
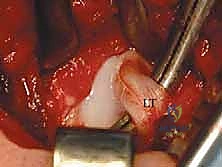
As the dissection deepens toward the lesser trochanter, the iliopsoas tendon is identified. The hip is flexed, abducted, and externally rotated to bring the lesser trochanter into the surgical field. The iliopsoas tendon, which is often severely contracted and indenting the inferior capsule, is isolated. A right-angle clamp is passed deep to the tendinous portion of the iliopsoas, and a fractional lengthening or complete tenotomy is performed at its insertion on the lesser trochanter. Extreme caution is exercised here to protect the Medial Femoral Circumflex Artery (MFCA), which courses in the immediate vicinity, traversing between the pectineus and the psoas.

Joint Access and Obstacle Clearance
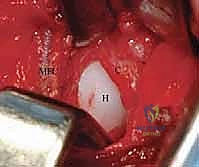
Following the psoas release, the inferior and medial aspects of the hip capsule are widely exposed. The capsule in a dislocated hip is typically thickened and exhibits an hourglass constriction. A crucial step is clearing the pericapsular fat to definitively identify the capsular margins. An arthrotomy is performed; I prefer a T-shaped or cruciate incision centered over the inferior capsule. The initial incision is made parallel to the acetabular rim, followed by a perpendicular limb extending toward the femur.
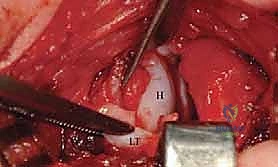
Upon entering the joint, the ligamentum teres is immediately visualized. It is invariably hypertrophied. The ligamentum teres is traced to its origin in the acetabular fossa and sharply excised. The true acetabulum is then inspected. The fibrofatty pulvinar, which occupies the depth of the acetabulum, is meticulously removed using a pituitary rongeur or a small curette. The transverse acetabular ligament (TAL) is identified spanning the inferior notch. If the TAL is contracted and prevents the femoral head from seating deeply, it is radially incised. The acetabular labrum is inspected; if inverted, it is gently everted, but it must never be excised, as it is a critical growth center for the acetabular rim.
Reduction and Spica Cast Application
With all intra-articular obstacles cleared, the femoral head is gently manipulated into the acetabulum. The reduction should be smooth and concentric, achieved with minimal force. The hip is placed in the "human position"—approximately 90 to 100 degrees of flexion and 40 to 50 degrees of abduction. Extreme abduction (the classic frog-leg position) must be strictly avoided, as it drastically increases the pressure on the MFCA against the acetabular rim, precipitating avascular necrosis.
Once reduction is achieved, stability is assessed. The capsule is loosely reapproximated with absorbable suture; a tight capsulorrhaphy is neither possible nor desired via this approach. The wound is irrigated and closed in layers, utilizing a subcuticular closure for the skin.
The patient is then transferred to a spica table. A 1.5-inch spica cast is applied, carefully maintaining the hip in the safe zone of flexion and moderate abduction. Meticulous padding is placed over all bony prominences. Post-reduction fluoroscopy, or occasionally a post-operative MRI or CT scan, is mandatory to confirm that the reduction remains perfectly concentric within the cast.
Complications, Incidence Rates, and Salvage Management
The medial open reduction, while highly effective, carries a specific complication profile that the orthopedic surgeon must be prepared to manage. The most devastating complication is Avascular Necrosis (AVN) of the capital femoral epiphysis. AVN results from iatrogenic vascular insult, either through direct injury to the MFCA during dissection or via mechanical occlusion caused by excessive pressure on the epiphyseal vessels when the hip is casted in extreme abduction. The Kalamchi-MacEwen classification is utilized to grade the severity of AVN, ranging from transient ossific nucleus changes (Type I) to severe damage of the entire epiphysis and physis leading to coxa magna, coxa breva, and premature physeal closure (Type IV).
Re-dislocation or subluxation is another significant risk. This typically occurs due to inadequate surgical clearance of intra-articular obstacles (e.g., failure to release a contracted TAL or remove a massive pulvinar), failure to recognize a highly deficient acetabulum that requires an osteotomy, or loss of reduction during the delicate process of spica cast application.
Infection, while rare given the robust vascularity of the pediatric groin, can be catastrophic if it enters the hip joint, leading to septic arthritis and rapid joint destruction. Neurovascular injuries are exceptionally rare if meticulous surgical technique is maintained, but the femoral nerve, femoral artery, and obturator nerve are all within the surgical vicinity.
| Complication | Estimated Incidence Rate | Pathoetiology | Salvage Management & Mitigation |
|---|---|---|---|
| Avascular Necrosis (AVN) | 5% - 15% | Vascular injury to MFCA; mechanical compression from extreme abduction in cast. | Mitigation: Avoid frog-leg casting; meticulous dissection. Salvage: Observation for mild cases; valgus producing osteotomies for severe hinge abduction. |
| Re-dislocation / Subluxation | 2% - 8% | Inadequate obstacle clearance; unaddressed severe dysplasia; poor casting technique. | Salvage: Immediate re-operation. Often requires conversion to an anterior approach with capsulorrhaphy and potential pelvic osteotomy. |
| Surgical Site Infection | < 1% | Proximity to perineum; prolonged operative time. | Mitigation: Ioban perineal isolation. Salvage: Prompt irrigation and debridement; intravenous antibiotics. |
| Neurovascular Injury | < 0.5% | Errant dissection anterior to pectineus (femoral bundle) or deep to adductors (obturator). | Mitigation: Strict adherence to the pectineus/brevis interval. Salvage: Intraoperative vascular repair if recognized; physical therapy for neuropraxia. |



