Masterclass in Open Reduction of Hand Dislocations: MCP and CMC Joints
Key Takeaway
Complex dislocations of the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints often resist closed reduction due to soft tissue interposition. The Kaplan volar approach systematically releases the constricting anatomical "noose" around the metacarpal head. For CMC fracture-dislocations, precise restoration of articular congruity via percutaneous pinning or open reduction is paramount to preserve grip strength and prevent post-traumatic arthrosis.
INTRODUCTION TO COMPLEX HAND DISLOCATIONS
The intricate biomechanics of the human hand rely on the precise anatomical alignment of the metacarpophalangeal (MCP) and carpometacarpal (CMC) joints. While many dislocations in the hand can be managed with prompt closed reduction, specific injury patterns are notoriously irreducible due to complex soft tissue interposition. In these scenarios, repeated forceful attempts at closed reduction are not only futile but actively deleterious, risking iatrogenic cartilage damage and neurovascular compromise.
This comprehensive guide details the advanced surgical management of irreducible hand dislocations, focusing heavily on the classic Kaplan volar approach for complex MCP joint dislocations and the systematic management of unstable CMC fracture-dislocations. Mastery of these techniques is an absolute prerequisite for orthopedic residents, hand fellows, and practicing consultants.
PART I: COMPLEX METACARPOPHALANGEAL (MCP) JOINT DISLOCATIONS
Complex dislocations of the MCP joint most frequently involve the index finger, followed by the small finger. Unlike simple subluxations, a "complex" dislocation implies that the volar plate has ruptured distally and become interposed between the base of the proximal phalanx and the metacarpal head, rendering closed reduction impossible.
Pathoanatomy and the "Anatomical Noose"
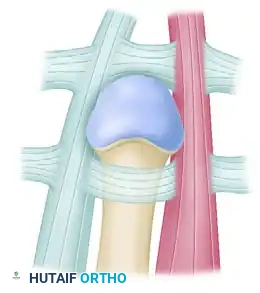
Understanding the pathoanatomy is critical. When the index finger MCP joint dislocates dorsally, the metacarpal head is driven volarly through the weakest point of the joint capsule. It becomes trapped in an anatomical "noose" composed of four distinct structures:
1. Volar Plate: Displaced dorsally over the metacarpal head, blocking reduction.
2. Natatory Ligament: Tightens distally across the metacarpal neck.
3. Superficial Transverse Metacarpal Ligament: Constricts proximally.
4. Lumbrical Muscle and Flexor Tendons: The lumbrical displaces radially, and the flexor tendons displace ulnarly, tightly flanking the metacarpal neck.
🚨 SURGICAL WARNING: In a complex MCP dislocation, the metacarpal head lies immediately deep to the palmar skin. The digital neurovascular bundle is stretched tightly over the prominent metacarpal head, making it highly susceptible to iatrogenic injury during the initial skin incision.
The Kaplan Volar Approach: Step-by-Step Surgical Technique
Emanuel Kaplan originally described the volar approach to systematically release the constricting elements of this noose. While a dorsal approach is advocated by some modern surgeons to avoid neurovascular injury and easily split the volar plate, the Kaplan volar approach remains a fundamental technique that directly addresses the primary pathology.
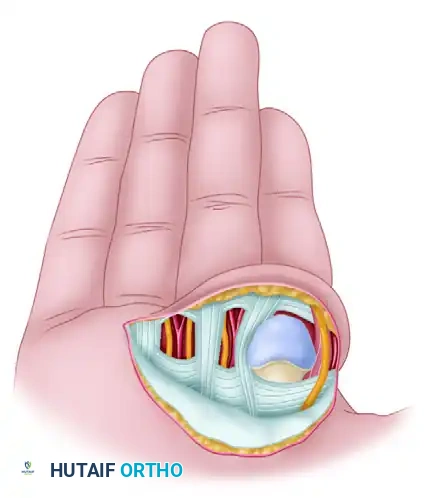
FIGURE 67-33: Kaplan open reduction of dislocation of the second metacarpophalangeal joint. The diagram illustrates the four structures that surround and constrict the metacarpal head: the volar plate, natatory ligament, superficial transverse metacarpal ligament, and the lumbrical/flexor tendon complex.
Step 1: Incision and Exposure
* Begin the incision in the thenar crease at the radial base of the index finger.
* Continue the incision proximally into the proximal palmar crease.
* Dissect bluntly through the subcutaneous tissues. Identify and protect the digital neurovascular bundles immediately, as they are displaced superficially by the prominent metacarpal head.
Step 2: Release of the Constricting Bands
To achieve reduction, the constricting bands must be systematically divided:
* First Incision (Volar Plate): Make the first incision to free the constriction of the cartilaginous volar plate. You must incise the free edge of the torn ligament down to the junction of the periosteum with the proximal phalanx. Clinical Pearl: The incision must penetrate the entire thickness of the plate; division of the plate alone is often insufficient.
* Second Incision (Natatory Ligament): Divide completely the transverse fibers of the taut natatory ligament.
* Third Incision (Superficial Transverse Metacarpal Ligament): Make another longitudinal incision through the transverse fibers of the superficial transverse metacarpal ligament. This incision should extend to the ulnar side of the first lumbrical muscle, effectively releasing the constriction below the metacarpal head.
Step 3: Joint Reduction
* Once the three primary releases are performed, the anatomical noose is decompressed.
* Apply gentle longitudinal traction and volar pressure to the dorsal aspect of the proximal phalanx.
* The proximal phalangeal base should return smoothly to its normal place over the metacarpal head.
* This permits the immediate replacement of the second metacarpal head in line with the other metacarpal heads. Following this, the flexor tendons, the volar plate, and the nerves and vessels will spontaneously restore to their normal anatomical positions.
Step 4: Closure and Postoperative Protocol
* Irrigate the joint thoroughly.
* Close the skin wound in a routine manner. Do not attempt to repair the volar plate, as this can lead to severe flexion contractures.
* Immobilize the finger in a functional position (MCP joint in 30-40 degrees of flexion) using a dorsal blocking splint for about 1 week.
* Initiate early active range of motion (ROM) within the constraints of the dorsal block to prevent stiffness.
PART II: CARPOMETACARPAL (CMC) JOINT FRACTURE-DISLOCATIONS
Dislocations and fracture-dislocations of the carpometacarpal joints—particularly the 4th and 5th digits—are high-energy injuries often resulting from axial loading (e.g., a punch). Because the 4th and 5th CMC joints are highly mobile compared to the rigid 2nd and 3rd CMC joints, they are uniquely susceptible to dorsal subluxation and fracture.
Clinical Evaluation and Imaging
Patients present with significant dorsoulnar hand swelling, shortening of the affected metacarpals, and loss of the normal knuckle contour.

FIGURE 67-30 A: Clinical appearance of the hand before reduction. Note the profound dorsoulnar hand swelling and loss of the normal metacarpal arch consistent with a 4th and 5th CMC dislocation.
Standard posteroanterior (PA), lateral, and oblique radiographs are mandatory. However, the overlapping anatomy of the carpus can obscure subtle subluxations.



FIGURE 67-30 B-D: Posteroanterior, Lateral, and Oblique radiographic views demonstrating the dorsal dislocation of the fourth and fifth carpometacarpal joints.
> CLINICAL PEARL: Always obtain a true lateral radiograph of the hand. The metacarpal shafts should align perfectly parallel. Any dorsal divergence of the 4th or 5th metacarpal shafts relative to the 3rd metacarpal is highly indicative of a CMC dislocation. If plain films are equivocal, a CT scan is the gold standard for evaluating articular comminution and subluxation.
Management of 4th and 5th CMC Dislocations
The primary goal of treatment is the anatomical restoration of the CMC articular surface to preserve grip strength and prevent early post-traumatic osteoarthritis.
Closed Reduction and Percutaneous Pinning (CRPP)
Many acute CMC dislocations can be reduced closed. Reduction is achieved via longitudinal traction combined with direct volar pressure over the dorsally displaced metacarpal bases.


FIGURE 67-30 E and F: In this case, longitudinal traction was adequate to reduce the joints, and a well-molded splint was satisfactory to maintain the reductions.
However, due to the deforming pull of the Extensor Carpi Ulnaris (ECU) tendon, these injuries are notoriously unstable. If the reduction is tenuous, percutaneous pinning is required.



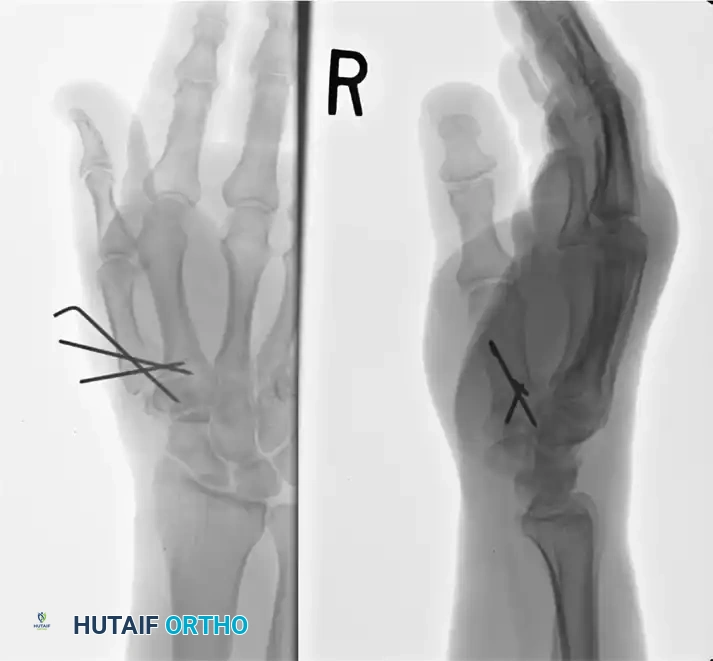
FIGURE 67-29 A-C: Preoperative radiographs of a small finger carpometacarpal fracture-subluxation in a 34-year-old man, demonstrating dorsal displacement and articular incongruity.
Surgical Technique for CRPP:
1. Perform closed reduction under fluoroscopic guidance.
2. Once anatomical alignment is confirmed, drive two 0.045-inch Kirschner wires (K-wires) percutaneously.
3. The wires are typically driven from the 5th metacarpal into the 4th metacarpal, and/or directly into the carpus (hamate) to provide rigid stabilization.



FIGURE 67-29 D-F: Postoperative radiographs showing the ring and small finger carpometacarpal joints reduced closed and stabilized with two 0.045-inch Kirschner wires.
The "Bennett-Like" Fracture of the 5th Metacarpal Base
A specific and highly unstable variant of the CMC fracture-dislocation is the intra-articular fracture of the base of the 5th metacarpal. This injury is biomechanically analogous to the Bennett fracture of the thumb.
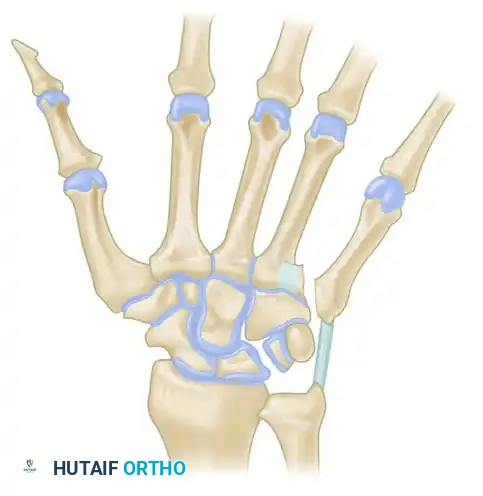
FIGURE 67-31: Unstable fracture of the base of the fifth metacarpal. The deforming forces permit proximal displacement of the shaft, similar to a Bennett fracture.
Biomechanics of Displacement:
* The strong volar ligaments retain the small anteromedial articular fragment in its anatomical position against the hamate.
* The Extensor Carpi Ulnaris (ECU) tendon, which inserts on the dorsoulnar base of the 5th metacarpal, exerts a powerful proximal and dorsal pull on the main metacarpal shaft.
* This results in proximal migration and dorsal subluxation of the metacarpal shaft.
Treatment Strategy:
Because of the continuous pull of the ECU, closed reduction alone is almost universally destined to fail. These fractures require CRPP or Open Reduction and Internal Fixation (ORIF). If the articular fragment is large enough, open reduction via a dorsal longitudinal incision and fixation with mini-fragment screws (1.5mm or 2.0mm) or K-wires is indicated to restore the articular congruity of the hamatometacarpal joint.
Management of Malunited CMC Fractures
Failure to recognize or adequately stabilize a 5th CMC fracture-dislocation leads to malunion. Patients present with chronic pain, weakness in grip strength, and a prominent dorsal bossing at the base of the hand.

FIGURE 67-32 A: Preoperative radiograph demonstrating a painful, malunited fracture of the base of the fifth metacarpal with significant dorsal subluxation.
While corrective osteotomy can be attempted in younger patients with preserved cartilage, post-traumatic arthrosis often dictates a salvage procedure. In these chronic, painful malunions, resection arthroplasty is the preferred surgical intervention.

FIGURE 67-32 B: Postoperative radiograph following resection arthroplasty. This is preferred over osteotomy in cases of severe arthrosis. Note that the tendon of the extensor carpi ulnaris (ECU) must be meticulously reattached to maintain wrist biomechanics.
Resection Arthroplasty Principles:
1. Expose the 5th CMC joint via a dorsal longitudinal incision.
2. Protect the dorsal sensory branch of the ulnar nerve.
3. Resect the malunited, arthritic base of the 5th metacarpal.
4. Crucial Step: The ECU tendon must be identified and securely reattached to the remaining metacarpal shaft or transferred to the 4th metacarpal base to prevent loss of ulnar deviation power and to stabilize the ulnar border of the hand.
5. Interposition of local soft tissue (such as a slip of the ECU or local capsule) can be utilized to prevent bony impingement against the hamate.
POSTOPERATIVE REHABILITATION PROTOCOLS
Whether managing an MCP dislocation via the Kaplan approach or a CMC fracture-dislocation via percutaneous pinning, postoperative rehabilitation is the final, critical phase of treatment.
For MCP Open Reductions:
* Days 1-7: Dorsal blocking splint maintaining the MCP joint in 30-40 degrees of flexion. The interphalangeal (IP) joints are left free to encourage immediate active motion, preventing extensor mechanism adhesions.
* Weeks 2-4: Transition to a dynamic extension splint if flexion contractures begin to develop, though active flexion is prioritized.
* Weeks 4-6: Wean from splinting. Begin passive stretching and strengthening.
For CMC Pinning/ORIF:
* Weeks 0-4: The hand is immobilized in a short-arm cast or rigid orthosis incorporating the 4th and 5th digits in an intrinsic-plus position. K-wires are left in place.
* Week 4-6: K-wires are removed in the clinic. The patient is transitioned to a removable splint and begins active range of motion of the wrist and digits.
* Weeks 6-8: Progressive strengthening is initiated. Heavy lifting and contact sports are restricted until 10-12 weeks postoperatively to ensure complete ligamentous and bony healing.
CONCLUSION
The open reduction of hand dislocations requires a profound understanding of the complex, three-dimensional anatomy of the hand. The Kaplan volar approach remains a masterclass in anatomical dissection, safely navigating the displaced neurovascular bundles to release the constricting noose of a complex MCP dislocation. Similarly, the vigilant identification and rigid stabilization of CMC fracture-dislocations—particularly the Bennett-like variants of the 5th metacarpal—are essential to prevent debilitating malunions. Adherence to these strict, evidence-based surgical principles ensures optimal functional recovery for the patient.
You Might Also Like