Master Orthopedic Board Exams: Interactive MCQ Practice Engine
Key Takeaway
An interactive MCQ engine significantly enhances orthopedic board exam preparation by providing realistic clinical scenarios and immediate feedback. It allows candidates to practice critical decision-making under timed conditions, simulate exam environments, and identify knowledge gaps. Detailed explanations for each question deepen understanding, optimizing study efficiency for successful board certification.
A 45-year-old male presents following a high-speed motor vehicle collision. He is hemodynamically unstable, with a heart rate of 120 bpm and blood pressure of 80/50 mmHg. Physical examination reveals a widely abducted lower extremity, perineal ecchymosis, and scrotal swelling. A Foley catheter insertion is attempted but meets resistance. A CT scan confirms an open-book pelvic fracture (APC-III) with significant symphyseal diastasis and sacral fractures. Which of the following is the most appropriate immediate next step in management after initial ATLS protocol?
Candidate: I would immediately apply a circumferential pelvic binder at the level of the greater trochanters to reduce the pelvic volume and assist in hemodynamic stabilization. I would also manage the urethral injury by requesting a urology consult for suprapubic catheterization and avoid further Foley attempts.
Candidates often confuse the location of the pelvic binder, applying it too high (at the level of the iliac crests), or prioritize the urethral injury investigation (retrograde urethrogram) while the patient is still hemodynamically unstable. They may also incorrectly jump to external fixation as the "next step," failing to realize that external fixation is a definitive stabilization measure that occurs after, not before, initial resuscitation.
The gold standard is to state: "This is a hemodynamically unstable patient with a suspected pelvic ring disruption. My priority is resuscitation according to ATLS principles. I would immediately apply a circumferential pelvic binder at the level of the greater trochanters to reduce pelvic volume and tamponade hemorrhage. Regarding the suspected urethral injury, I would stop any further Foley attempts to prevent conversion of a partial to a complete tear and consult urology for a suprapubic catheter. Hemodynamic stability should be reassessed; if unstable despite volume replacement and the binder, I would trigger the massive transfusion protocol and prepare for pelvic angiography/embolization or pre-peritoneal packing."
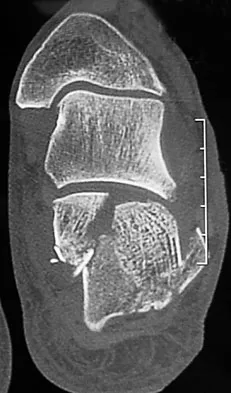
Look at this radiograph of a 32-year-old male who presents with chronic wrist pain and snuffbox tenderness after a fall onto an outstretched hand 6 months ago. What is your diagnosis and management plan?
Candidate: This appears to be a scaphoid waist nonunion with sclerotic edges. I would suspect this is a symptomatic nonunion and would plan for surgical stabilization using a bone graft and internal fixation, as conservative measures are unlikely to succeed at this stage.
Failure to categorize the stage of the nonunion or acknowledge the presence of degenerative changes (SNAC wrist). Some candidates suggest prolonged immobilization (e.g., bone stimulators or cast for 3 more months) despite clear radiographic evidence of nonunion and sclerosis, which is ineffective.
A high-scoring answer systematically classifies the injury: "This is an established scaphoid waist nonunion. Given the patient's age, symptoms, and radiographic sclerosis, union is unlikely with immobilization. I would discuss operative intervention. My management plan would be to: 1) Obtain a CT scan to assess the extent of sclerosis and any humpback deformity. 2) If the joint is preserved (no SNAC wrist), I would offer a non-vascularized bone graft (e.g., Russe technique) or a vascularized bone graft (e.g., 1,2 ICSRA) if the pole is avascular. 3) If there is a humpback deformity, an opening wedge graft is required. If degenerative changes were present, salvage options like proximal row carpectomy or midcarpal arthrodesis would be discussed."
