Operative Management of Lisfranc and Fifth Metatarsal Fractures: A Masterclass in Midfoot Trauma

Key Takeaway
The operative management of tarsometatarsal (Lisfranc) fracture-dislocations and fifth metatarsal base fractures requires meticulous surgical technique and rigid fixation. This guide details the anatomic approaches, neurovascular protection, and step-by-step reduction strategies for Lisfranc injuries, alongside evidence-based intramedullary screw fixation protocols for Jones fractures. Mastery of these techniques ensures optimal biomechanical restoration, minimizes post-traumatic arthrosis, and accelerates return to function in both standard and high-demand athletic populations.
Comprehensive Introduction and Patho-Epidemiology
The midfoot serves as the critical biomechanical transition zone between the rigid hindfoot and the flexible, accommodating forefoot. It is the architectural keystone of both the longitudinal and transverse arches of the foot, responsible for transmitting immense ground reaction forces during the stance phase of gait. Injuries to this region, particularly tarsometatarsal (Lisfranc) fracture-dislocations and proximal fifth metatarsal fractures, present profound diagnostic and therapeutic challenges to the orthopaedic surgeon. Missed diagnoses, delayed interventions, or inadequate anatomic reductions inevitably lead to catastrophic post-traumatic arthrosis, midfoot collapse (planovalgus deformity), and debilitating functional impairment that can permanently alter a patient's quality of life.
Epidemiologically, Lisfranc injuries are relatively uncommon, accounting for approximately 0.2% of all orthopaedic fractures, translating to an incidence of 1 in 55,000 persons per year. However, this statistic is notoriously deceptive due to a historically high rate of missed diagnoses. Up to 20% to 30% of these injuries are overlooked during initial emergency department evaluations, often mischaracterized as simple midfoot sprains. These injuries present a bimodal distribution: high-energy trauma (such as motor vehicle collisions or crush injuries) causing dramatic, multidirectional instability, and low-energy sports-related injuries (axial loading on a plantarflexed foot) resulting in subtle, purely ligamentous diastasis that demands a high index of clinical suspicion.


Concurrently, proximal fifth metatarsal fractures represent a distinct but equally perilous subset of midfoot trauma. These fractures are ubiquitous in athletic populations and are anatomically divided into three distinct zones, each with unique vascularity and healing potential. Zone 2 (Jones fractures) and Zone 3 (diaphyseal stress fractures) are particularly notorious for their propensity toward delayed union and nonunion due to a tenuous vascular watershed area. The operative management of both Lisfranc and fifth metatarsal injuries requires a masterful understanding of local pathoanatomy, precise surgical execution, and rigid adherence to biomechanical principles.
This comprehensive guide delineates the textbook-level, evidence-based operative management of these complex midfoot injuries. It provides a step-by-step architectural blueprint for surgical approaches, neurovascular protection, reduction sequencing, and rigid internal fixation, tailored specifically for orthopaedic residents, trauma fellows, and practicing consultants aiming to optimize patient outcomes in the face of devastating midfoot trauma.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Tarsometatarsal Articulation
The stability of the tarsometatarsal (TMT) joint complex relies heavily on its intrinsic bony architecture. The articulation forms a Roman arch in the coronal plane, with the base of the second metatarsal recessed proximally between the medial and lateral cuneiforms. This creates a highly constrained "keystone" configuration that effectively locks the midfoot and prevents medial-lateral translation during weight-bearing. The first three metatarsals articulate with the three cuneiforms, forming the relatively rigid medial and central columns, while the fourth and fifth metatarsals articulate with the cuboid, forming the more mobile lateral column that accommodates uneven terrain.
Crucially, the ligamentous network supporting this bony architecture is asymmetrical. The plantar ligaments are significantly thicker and stronger than their dorsal counterparts, explaining why dorsal displacement of the metatarsals is the most common pattern in TMT dislocations. Furthermore, there is a distinct absence of a transverse intermetatarsal ligament connecting the bases of the first and second metatarsals. Instead, the primary stabilizing structure is the Lisfranc ligament, a robust, oblique interosseous band originating from the lateral aspect of the medial cuneiform and inserting onto the medial base of the second metatarsal. Disruption of this ligament, either through direct crush or indirect axial loading, leads to decoupling of the medial and central columns.


Vascular and Neural Topography of the Midfoot
Surgical navigation of the midfoot requires meticulous respect for its neurovascular topography. The dorsalis pedis artery, a continuation of the anterior tibial artery, courses distally over the anterior aspect of the ankle and passes directly over the dorsal aspect of the middle cuneiform and the base of the second metatarsal. It plunges headlong into the proximal first intermetatarsal space to join the deep plantar arch. The deep peroneal nerve accompanies the dorsalis pedis artery, supplying sensation to the first web space. Both structures are at extreme risk during the standard dorsomedial surgical approach to the Lisfranc complex and must be identified and gently retracted.
The vascular anatomy of the fifth metatarsal is equally critical, particularly regarding fracture healing. The proximal diaphysis relies on a retrograde intramedullary blood supply from a nutrient artery entering the medial cortex in the middle third of the bone. The metaphyseal-diaphyseal junction (Zone 2) and the proximal diaphysis (Zone 3) represent a vascular watershed area, rendering fractures in this region highly susceptible to avascularity and nonunion. Additionally, the insertion of the peroneus brevis tendon on the dorsal-lateral tuberosity and the lateral band of the plantar fascia on the plantar aspect exert powerful deforming forces that necessitate robust internal fixation.


Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in midfoot trauma hinges on the degree of displacement, the specific anatomical zone of injury, and the functional demands of the patient. Non-operative management of Lisfranc injuries is strictly reserved for truly non-displaced injuries (less than 2 mm of displacement on weight-bearing views) with absolutely no evidence of dynamic instability on stress fluoroscopy. For fifth metatarsal fractures, non-operative management is typically reserved for Zone 1 (pseudo-Jones) avulsion fractures, which heal predictably with symptomatic immobilization.
Absolute indications for Open Reduction and Internal Fixation (ORIF) or primary arthrodesis in Lisfranc injuries include any displacement greater than 2 mm at any TMT joint, a talar-first metatarsal angle exceeding 15 degrees, or radiographic evidence of a bony avulsion of the Lisfranc ligament (the pathognomonic "fleck sign"). Open fractures, impending compartment syndrome of the foot, and irreducible dislocations due to soft tissue interposition (commonly the anterior tibial tendon or peroneus longus) are surgical emergencies.
For proximal fifth metatarsal fractures, operative intervention with intramedullary screw fixation is highly indicated for acute Zone 2 (Jones) fractures in elite athletes or highly active individuals to minimize the risk of nonunion and accelerate return to play. Zone 3 diaphyseal stress fractures, particularly those with sclerosis or obliteration of the medullary canal, almost universally require operative intervention, often augmented with bone grafting.
| Indication / Contraindication | Lisfranc (TMT) Fracture-Dislocations | Proximal 5th Metatarsal Fractures |
|---|---|---|
| Absolute Indications | Displacement >2mm on WB views; Open fractures; Compartment syndrome; "Fleck sign" | Acute Zone 2 in athletes; Zone 3 stress fractures; Symptomatic nonunions |
| Relative Indications | Purely ligamentous injuries (Primary Arthrodesis vs ORIF); Polytrauma | Acute Zone 2 in sedentary patients (shared decision making) |
| Absolute Contraindications | Active deep infection; Severe peripheral arterial disease (PAD) | Active deep infection; Severe PAD precluding wound healing |
| Relative Contraindications | Severe peripheral neuropathy (Charcot arthropathy); Non-ambulatory status | Charcot neuroarthropathy; Poor soft tissue envelope |


Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Pre-Operative Templating
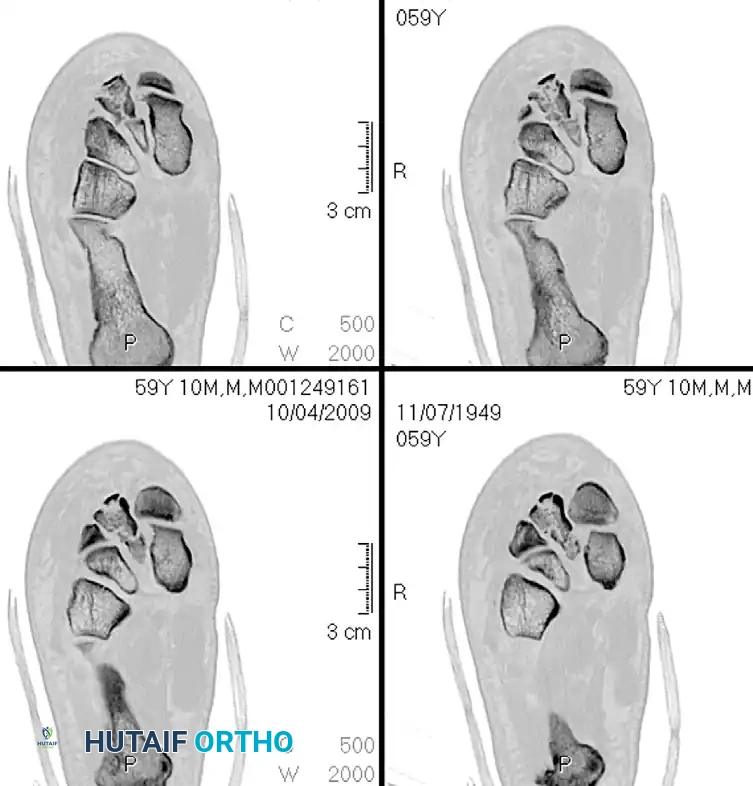
Meticulous pre-operative planning is the cornerstone of successful midfoot reconstruction. While standard non-weight-bearing radiographs (AP, lateral, and 30-degree internal oblique) are the initial screening tools, they frequently underestimate the severity of the injury. If clinical suspicion remains high despite negative static films, weight-bearing radiographs or intraoperative stress fluoroscopy (abduction and pronation stress) are mandatory. Computed Tomography (CT) is the gold standard for delineating complex fracture patterns, identifying occult intra-articular comminution, and mapping the exact trajectory of dislocated fragments. Magnetic Resonance Imaging (MRI) is invaluable for diagnosing purely ligamentous Lisfranc injuries when CT and radiographs are equivocal.
Templating must account for the specific fracture morphology. For Lisfranc injuries, the surgeon must decide between transarticular screw fixation and dorsal bridge plating. Solid or cannulated 3.5 mm or 4.0 mm cortical screws are typically templated for the medial and central columns. If severe comminution is present on the CT scan, low-profile dorsal spanning plates should be selected to avoid joint foreshortening and iatrogenic cartilage damage. For fifth metatarsal fractures, templating the intramedullary canal diameter on the AP and lateral radiographs is critical to select the appropriate solid or cannulated partially threaded screw (typically 4.5 mm to 5.5 mm in diameter).

Patient Positioning and Operating Room Setup
The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, perfectly vertical position. This is particularly crucial for fifth metatarsal fixation, where access to the lateral border of the foot is required. A thigh tourniquet is applied and padded meticulously.
The fluoroscopy unit (C-arm) is brought in from the contralateral side of the table, allowing the surgeon unimpeded access to the operative field. The monitor should be positioned directly in the surgeon's line of sight. Prior to prepping and draping, a fluoroscopic "time-out" is performed to ensure that perfect AP, lateral, and oblique views of the midfoot can be obtained without obstruction from the table pedestal or the contralateral leg. Prophylactic intravenous antibiotics are administered 30 minutes prior to tourniquet inflation.


Step-by-Step Surgical Approach and Fixation Technique
The Dual Incision Approach for Lisfranc Reconstruction
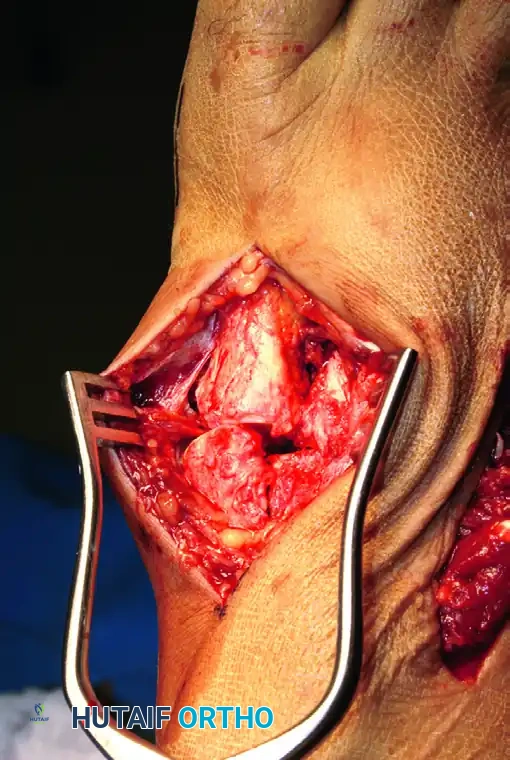
Proper exposure of the TMT complex is paramount; closed reduction and percutaneous pinning are unequivocally discouraged due to the high likelihood of interposed soft tissue blocking anatomic reduction. The gold standard is a dual dorsal incision technique. The dorsomedial incision is centered over the first intermetatarsal space, extending from the naviculocuneiform joint to the mid-diaphysis of the first and second metatarsals. Deep dissection involves incising the extensor retinaculum and mobilizing the extensor hallucis brevis (EHB) muscle belly laterally. The dorsalis pedis artery and deep peroneal nerve are meticulously isolated and protected with a vessel loop.
If access to the lateral column is required, a dorsolateral incision is placed over the third intermetatarsal space, in line with the fourth metatarsal. It is an absolute surgical imperative to maintain a wide skin bridge—minimum 5 to 7 centimeters—between these two incisions. Narrow skin bridges in the watershed area of the dorsal foot are at extreme risk for full-thickness necrosis, a complication that frequently necessitates free tissue transfer and severely compromises the functional outcome.


Reduction Sequencing and the "Homerun" Screw
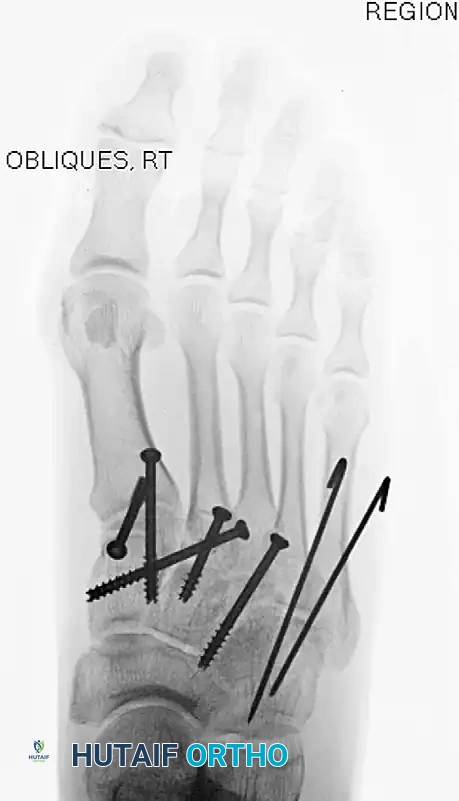
The midfoot must be reconstructed systematically from medial to lateral. The first TMT joint is debrided of all osteochondral debris and hematoma. It is anatomically reduced and provisionally stabilized with a pointed reduction clamp. A 4.0-mm solid cortical screw is placed from the dorsal aspect of the first metatarsal base, aiming proximally and plantarward into the medial cuneiform.
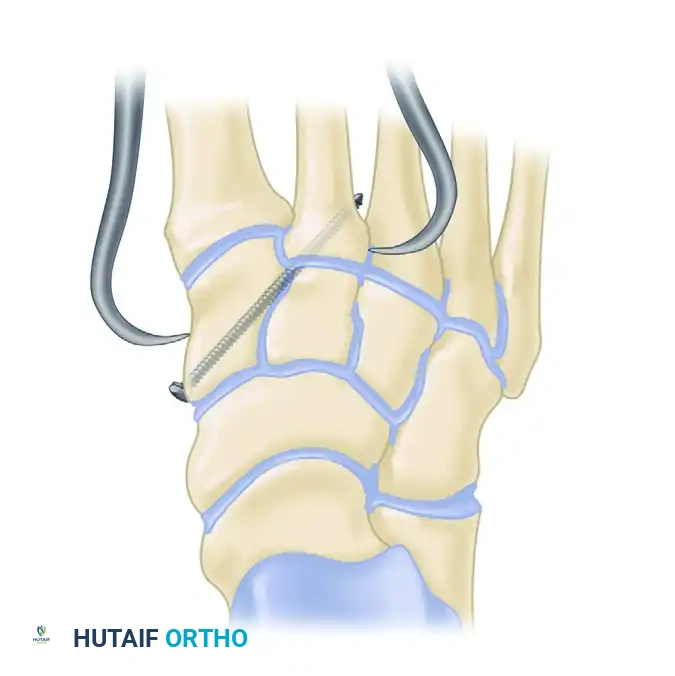
The cornerstone of the reconstruction is the "Homerun" screw, which recreates the stabilizing force of the ruptured Lisfranc ligament. The second metatarsal base is reduced into its keystone slot between the medial and lateral cuneiforms. A guidewire is introduced from the medial aspect of the medial cuneiform, aiming laterally and distally into the base of the second metatarsal. Following overdrilling of the near cortex, a 4.0-mm or 4.5-mm cannulated screw is inserted to compress the interval. The third TMT joint is subsequently reduced and fixed with a single dorsal-to-plantar transarticular screw.


Managing Comminution and Lateral Column Stabilization
In scenarios involving severe articular comminution or purely ligamentous injuries, transarticular screw fixation is contraindicated. Compression across a comminuted joint leads to architectural shortening and profound deformity, while screws placed through intact cartilage in purely ligamentous injuries cause iatrogenic arthrosis. In these instances, dorsal bridge plating is the technique of choice. Low-profile titanium plates are contoured to span the TMT joints, securing the metatarsal diaphysis to the cuneiforms without violating the articular surface.
The lateral column (fourth and fifth TMT joints) is highly mobile and essential for gait mechanics. Rigid screw fixation here leads to catastrophic stiffness and hardware failure. Instead, lateral metatarsocuboid disruptions are reduced and stabilized provisionally with smooth 1.5-mm or 2.0-mm K-wires (Steinmann pins) driven from the metatarsals into the cuboid. These pins are left protruding through the skin or buried superficially for routine removal in the clinic at 6 to 8 weeks post-operatively.

Intramedullary Fixation of the Fifth Metatarsal
For Zone 2 and Zone 3 proximal fifth metatarsal fractures, precise intramedullary screw fixation is required. A 2-3 cm longitudinal incision is made slightly dorsal to the lateral border of the foot, centered over the base of the fifth metatarsal. The sural nerve must be identified and protected. The peroneus brevis tendon is retracted plantarward.
The entry point is critical: it must be "high and tight" on the proximal tip of the tuberosity to ensure the guidewire passes directly down the anatomical axis of the medullary canal. A starting point that is too lateral or plantar will result in medial cortical blowout or eccentric reaming. A guidewire is passed under fluoroscopic guidance, confirming intraosseous placement on AP, lateral, and oblique views. The canal is tapped, and a solid or cannulated partially threaded screw (typically 4.5 mm, 5.0 mm, or 5.5 mm) is inserted. The screw threads must bypass the fracture site entirely to achieve adequate interfragmentary compression.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, midfoot trauma is fraught with complications. The energy absorbed by the osteochondral surfaces during the initial injury frequently leads to post-traumatic osteoarthritis, even in the setting of a perfect radiographic reduction. Post-traumatic arthrosis of the TMT joints occurs in up to 25% to 50% of operatively managed Lisfranc injuries, typically presenting as midfoot pain, dorsal osteophyte formation, and progressive arch collapse.
Hardware complications are also prevalent. Transarticular screws placed across the medial and central columns are subjected to immense cyclical loading during weight-bearing and frequently break if not removed prior to unrestricted activity. For fifth metatarsal fractures, nonunion remains a significant risk, particularly in Zone 3 stress fractures where the biologic healing potential is compromised by the watershed blood supply.
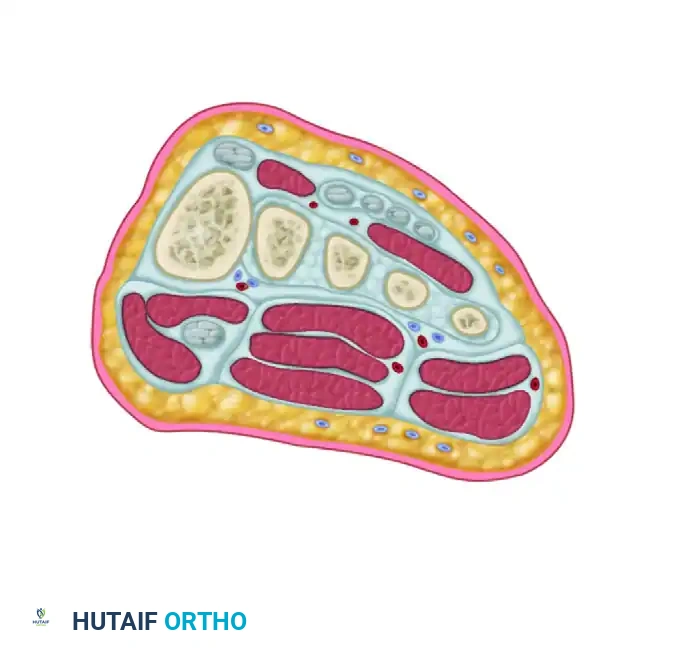
Compartment syndrome of the foot is a devastating early complication of high-energy midfoot crush injuries. The foot contains nine discrete fascial compartments. Prophylactic release of the interosseous compartments via dual dorsal incisions is mandatory if compartmental pressures are elevated or if the clinical exam demonstrates pain out of proportion, tense swelling, and pain with passive toe stretch.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Post-Traumatic Arthrosis | 25% - 50% (Lisfranc) | Prevention: Anatomic reduction, dorsal plating for comminution. Salvage: Midfoot arthrodesis (TMT fusion) with rigid plating and bone grafting. |
| Hardware Failure / Breakage | 10% - 15% | Prevention: Routine removal of transarticular screws at 4-5 months. Salvage: Retention of asymptomatic broken hardware; removal if symptomatic. |
| Nonunion (5th Metatarsal) | 5% - 10% (Zone 2/3) | Prevention: Large diameter solid screws, meticulous canal preparation. Salvage: Revision ORIF with exchange nailing, autologous bone grafting, orthobiologics. |
| Foot Compartment Syndrome | < 5% (High-energy crush) | Prevention: High clinical suspicion, serial exams. Salvage: Emergent dorsal dual-incision fasciotomies; delayed primary closure or skin grafting. |
| Dorsal Skin Necrosis | 2% - 5% | Prevention: Maintain >5cm skin bridge, meticulous soft tissue handling. Salvage: Vacuum-assisted closure, local rotational flaps, or free tissue transfer. |




Phased Post-Operative Rehabilitation Protocols
Phase I: Immediate Post-Operative Period (Weeks 0-2)
The immediate post-operative goal is strict protection of the osteosynthesis and aggressive mitigation of soft tissue edema. Following closure, the foot is placed in a bulky, well-padded Jones dressing reinforced with a rigid posterior plaster splint. The ankle is immobilized in neutral dorsiflexion. The patient is instructed to remain strictly non-weight-bearing (NWB) on the operative extremity. Elevation of the limb above the level of the heart is mandatory for the first 48 to 72 hours to prevent wound dehiscence and blistering. Deep vein thrombosis (DVT) prophylaxis is initiated based on patient-specific risk factors.
At the 10 to 14-day mark, the patient returns to the clinic for the first post-operative evaluation. The splint and bulky dressing are removed, and the surgical incisions are inspected for healing. Sutures or staples are removed if the skin edges are fully coapted. The patient is then transitioned into a short-leg fiberglass cast or a rigid controlled ankle motion (CAM) boot, continuing strict NWB precautions.


Phase II: Intermediate Healing and Hardware Management (Weeks 6-12)
At 6 to 8 weeks post-operatively, radiographs are obtained out of the cast or boot to assess for early callus formation and maintenance of reduction. For Lisfranc injuries, any laterally placed smooth K-wires stabilizing the fourth and fifth TMT joints are removed in the clinic. If radiographic healing is progressing satisfactorily, the patient is permitted to begin progressive partial weight-bearing in the CAM boot, starting at 25% body weight and advancing slowly over the next 4 weeks.
Physical therapy is initiated during this phase, focusing on active and active-assisted range of motion of the ankle, subtalar, and metatarsophalangeal joints. Intrinsic foot strengthening exercises (e.g., towel scrunches, marble pickups) are introduced to combat disuse atrophy. For fifth metatarsal fractures, full weight-bearing in a stiff-soled shoe or boot is often permitted earlier (around 6 weeks) if robust radiographic union is evident.


Phase III: Advanced Rehabilitation and Return to Function (Months 3-6+)
By 12 weeks, patients are typically transitioned out of the CAM boot and into a supportive athletic shoe equipped with a custom-molded, rigid carbon-fiber orthotic. This orthotic is crucial for providing structural support to the longitudinal arch and minimizing stress across the healing TMT joints. Weight-bearing is advanced to full, unassisted ambulation as tolerated.
For Lisfranc injuries managed with transarticular screws, hardware removal is strongly considered at 4 to 5 months post-operatively. Removing the rigid medial and central column screws prevents fatigue failure of the hardware once the patient returns to high-impact activities. Dorsal spanning plates, however, are often left in place indefinitely unless they become symptomatic due to soft tissue irritation. Return to competitive sports or heavy manual labor is a highly individualized decision, typically occurring between 6 and 9 months, contingent upon symmetrical strength, absence of pain with dynamic loading, and complete radiographic consolidation.
Summary of Landmark Literature and Clinical Guidelines
The operative management of midfoot trauma has evolved significantly, guided by several landmark biomechanical and clinical studies. For Lisfranc injuries, the seminal work by Kuo et al. established that the long-term functional outcome is directly correlated with the anatomic reduction of the TMT joints. A residual displacement of even 2
Clinical & Radiographic Imaging Archive