

AAOS & ABOS Upper Extremity MCQs (Set 4): Shoulder, Elbow, Wrist, Hand & Nerve Review | 2025-2026 Boards
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 52-year-old man has shoulder pain and stiffness after undergoing a "mini-lateral" rotator cuff repair 6 months ago. Examination reveals that he is afebrile with normal vital signs. There is slight erythema but no drainage from the incision. Range of motion is limited in all planes, and there is weakness with resisted external rotation and abduction. Radiographs show a well-positioned metal implant within the greater tuberosity. Laboratory studies reveal a WBC count of 8,400/mm3 (normal 3,500 to 10,500/mm3) and an erythrocyte sedimentation rate of 63 mm/h (normal up to 20 mm/h). What is the next most appropriate step in management?
Explanation
Question 2
A 21-year-old pitcher reports shoulder pain with hard throwing. He notes that the pain occurs in the early acceleration phase of his throw. Given his history, what structures are at greatest risk for injury?
Explanation
Question 3
A 30-year-old man landed on his shoulder in a fall off his mountain bike. An AP radiograph and CT scan are shown in Figures 34a and 34b. Management should consist of

Explanation
Question 4
A 22-year-old professional baseball pitcher has had pain in the axillary region of his dominant shoulder for the past several weeks. While throwing a pitch during a game, he notes a sharp pulling sensation with a "pop" in his shoulder. Examination the following day reveals tenderness along the posterior axillary fold and pain and weakness with resisted extension of the shoulder. What is the most likely cause of his symptoms?
Explanation
Question 5
When comparing the addition of a trough at the greater tuberosity to direct repair of cortical bone, simulated rotator cuff repair in animal models has shown what type of change in the strength of the repair?
Explanation
Question 6
Figures 35a and 35b show the radiographs of a 20-year-old man who is unable to rotate his dominant forearm. Examination reveals that the arm is fixed in supination. To regain motion, management should consist of

Explanation
Question 7
A 20-year-old-man sustained a scapular fracture after attempting to grab a beam as he fell through a ceiling at a job site 3 months ago. A clinical photograph is shown in Figure 36. He now reports pain in the anterior shoulder and difficulty with overhead activities. What nerve roots make up the involved peripheral nerve?

Explanation
Question 8
A 20-year-old collegiate baseball pitcher has persistent deep shoulder pain. Examination reveals normal strength, 130 degrees of external rotation in abduction, 10 degrees of internal rotation in abduction, mild dynamic scapular winging, and equivocal findings on provocative tests for labral tears. Management should consist of
Explanation
Question 9
Which of the following best describes the most common anatomic variation seen in the glenoid labrum and the middle glenohumeral ligament in the anterosuperior quadrant of the shoulder??
Explanation
Question 10
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
Question 11
A 10-year-old boy has had a prominent scapula for the past year. He reports crepitus and aching over the area, but only when he is active. A radiograph and CT scans are shown in Figures 37a through 37c. What is the most likely diagnosis?
Explanation
Question 12
In patients who have undergone nonsurgical management for idiopathic adhesive capsulitis, long-term follow-up studies have shown which of the following results?
Explanation
Question 13
Which of the following statements best describes the relationship between tissue response to thermal capsulorrhaphy and the type of device used?
Explanation
Question 14
A 35-year-old man has profound deltoid weakness after sustaining a traumatic anterior shoulder dislocation 6 weeks ago. Electromyographic (EMG) studies confirm an axillary nerve injury. Follow-up examination at 3 months reveals no recovery of function. What is the best course of action?
Explanation
Question 15
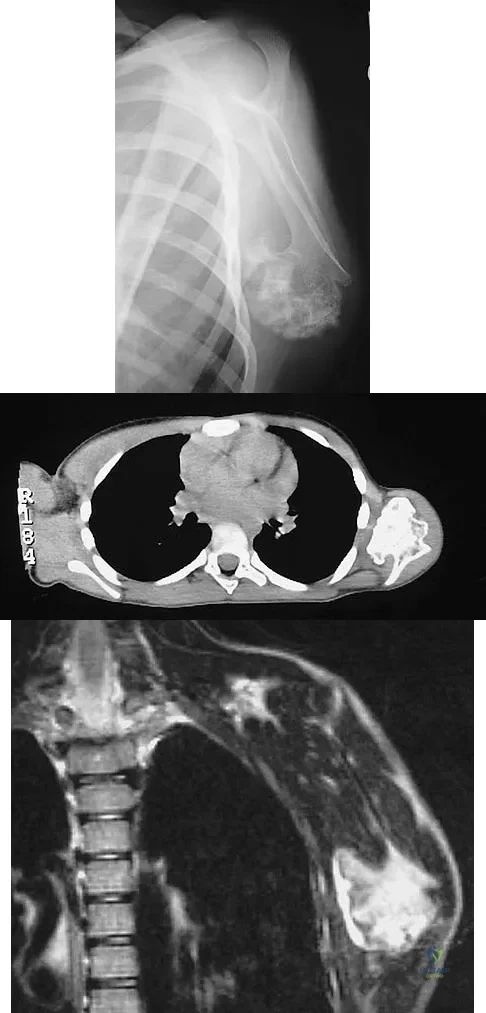
A 65-year-old woman has had chronic aching discomfort involving her elbow for the past 6 months. Radiographs and a biopsy specimen are shown in Figures 38a through 38c. What is the most likely diagnosis?

Explanation
Question 16
Which of the following clinical findings is commonly associated with symptomatic partial-thickness rotator cuff tears?
Explanation
Question 17
A 65-year-old woman landed on her nondominant left shoulder in a fall. An AP radiograph is shown in Figure 39. Management should consist of

Explanation
Question 18
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
Question 19
An otherwise healthy 13-year-old boy sustains the fracture shown in Figure 40 while throwing a fastball. Management should consist of

Explanation
Question 20
A 24-year-old man sustains an injury to his right elbow after falling 10 feet. Radiographs are shown in Figures 41a and 41b. Treatment should consist of

Explanation
Question 21
After closed reduction of the dislocation shown in Figure 42, it is essential to avoid placing the upper extremity in what position for the first 4 to 6 weeks?

Explanation
Question 22
A baseball player has had diffuse scapular soreness for the past 8 weeks. He reports that it began insidiously over several days and gradually has become worse. He denies any history of trauma. Examination reveals drooping of the shoulder, with lateral winging of the scapula at rest. He is otherwise neurologically intact. What is the best course of action?
Explanation
Question 23
Which of the following best describes the mechanical response of the inferior glenohumeral ligament to repetitive subfailure strains?
Explanation
Question 24
A 38-year-old woman who tripped and fell on her outstretched arm reports pain with movement. Examination reveals swelling. AP and lateral radiographs are shown in Figures 43a and 43b. Management should consist of

Explanation
Question 25
A 15-year-old girl reports popping and clicking at the sternoclavicular joint and an intermittent asymmetrical prominence of the medial head of the clavicle. She denies any history of trauma or other symptoms. Management should consist of
Explanation
Question 26
A 45-year-old manual laborer presents with chronic right wrist pain. Radiographs demonstrate a scaphoid nonunion with radioscaphoid arthritic changes, but the capitolunate joint is preserved. Which of the following is the most appropriate surgical treatment to relieve pain while best preserving his grip strength?
Explanation
Question 27
A 35-year-old male falls from a ladder and sustains a 'terrible triad' injury of the elbow. Operative fixation is planned. What is the most widely accepted sequence of surgical reconstruction to restore elbow stability?
Explanation
Question 28
A 65-year-old woman is scheduled to undergo a reverse total shoulder arthroplasty for cuff tear arthropathy. To minimize the risk of scapular notching, how should the glenosphere baseplate optimally be positioned?
Explanation
Question 29
During surgical fasciectomy for Dupuytren's contracture, the neurovascular bundle is at risk of iatrogenic injury. The spiral cord is known to displace the neurovascular bundle in which of the following directions?
Explanation
Question 30
A 28-year-old male sustained a closed midshaft humerus fracture and was placed in a coaptation splint in the emergency department. Two weeks later in clinic, he presents with a complete inability to extend his wrist or fingers, a deficit that was strictly documented as absent during his initial ED exam. What is the most appropriate next step in management?
Explanation
Question 31
A 22-year-old collision athlete presents with recurrent anterior shoulder instability. A 3D CT scan reveals 30% anterior glenoid bone loss. What is the most appropriate surgical intervention to minimize the risk of recurrent instability?
Explanation
Question 32
A surgeon is performing a single-incision anterior approach to repair an acute distal biceps tendon rupture. Which of the following nerves is at the greatest risk of iatrogenic injury during this specific approach?
Explanation
Question 33
A 45-year-old female presents with severe basilar thumb pain and a positive grind test. In primary osteoarthritis of the thumb carpometacarpal (CMC) joint, which muscle acts as the primary deforming force leading to proximal, radial, and dorsal subluxation of the first metacarpal base?
Explanation
Question 34
A 55-year-old man presents with advanced scapholunate advanced collapse (SLAC) wrist. During surgical planning, the surgeon relies on the fact that a specific carpal articulation is characteristically spared from degenerative changes due to its concentric spherical anatomy. Which joint is this?
Explanation
Question 35
A 30-year-old carpenter sustains a sharp volar laceration to his right index finger, resulting in a zone II flexor tendon injury. Following a 4-strand repair, a dynamic early active motion protocol is initiated. What is the primary biological and mechanical benefit of this protocol compared to prolonged static splinting?
Explanation
Question 36
A 70-year-old man presents with chronic, massive, irreparable rotator cuff tears of the supraspinatus and infraspinatus. Physical examination reveals pseudoparalysis of the shoulder with active forward elevation limited to 40 degrees. MRI demonstrates Goutallier stage 4 fatty infiltration of the torn tendons, but the teres minor and subscapularis remain intact. Which of the following is the most appropriate surgical management?
Explanation
Question 37
A 24-year-old gymnast falls from a height onto an extended, ulnar-deviated wrist. A lateral radiograph demonstrates the 'spilled teacup' sign with volar displacement of the lunate. She complains of severe pain and tingling in her thumb, index, and middle fingers. What is the most critical initial step in management?
Explanation
Question 38
A 60-year-old mechanic presents with intrinsic muscle wasting of the hand, a positive Froment sign, and numbness in the small and ulnar half of the ring fingers. He is diagnosed with severe cubital tunnel syndrome. Which structure typically forms the anatomical roof of the cubital tunnel?
Explanation
Question 39
A 40-year-old man presents with a volar shear fracture of the distal radius (Barton's fracture). The surgeon elects to perform open reduction and internal fixation utilizing the standard volar Henry approach. The internervous plane for this approach is found between which two muscles?
Explanation
Question 40
A 21-year-old collegiate baseball pitcher reports sudden medial elbow pain and an audible pop during the acceleration phase of throwing. Valgus stress testing reveals gross laxity. In surgical reconstruction of the ulnar collateral ligament (UCL), which specific anatomic bundle is the primary restraint to valgus stress from 30 to 120 degrees of elbow flexion?
Explanation
Question 41
A 35-year-old cyclist sustains a comminuted midshaft clavicle fracture. Open reduction and internal fixation with superior plating is performed. Postoperatively, the patient notes a well-demarcated area of numbness over the anterior chest wall just inferior to the incision. Which nerve was most likely injured during the surgical exposure?
Explanation
Question 42
A 25-year-old male sustains a Type III acromioclavicular (AC) joint separation and opts for nonoperative management after thorough counseling. According to long-term outcome studies, what is the most common persistent patient complaint following nonoperative management of this injury?
Explanation
Question 43
A 19-year-old motorcyclist sustains a traction injury to his right shoulder. On examination, his arm hangs at his side with the shoulder adducted, internally rotated, and the forearm pronated (waiter's tip posture). Hand and wrist flexion remain intact. This presentation is most consistent with an injury to which anatomic region of the brachial plexus?
Explanation
Question 44
A 45-year-old male is struck on the forearm with a heavy pipe. Radiographs reveal an isolated fracture of the proximal third of the ulnar shaft combined with an anterior dislocation of the radial head. What is the appropriate eponymous designation for this specific injury pattern?
Explanation
Question 45
A 35-year-old woman sustains a "terrible triad" injury of the elbow after a fall from a ladder. She is scheduled for operative fixation. To optimally restore elbow stability, what is the generally accepted sequence of surgical reconstruction?
Explanation
Question 46
A 28-year-old carpenter lacerates his index finger flexor tendons in Zone II. During surgical repair, strict adherence to the flexor pulley system anatomy is required. Preservation or reconstruction of which of the following pulleys is most critical to prevent significant tendon bowstringing?
Explanation
Question 47
A 45-year-old man presents with chronic wrist pain and is diagnosed with scaphoid nonunion advanced collapse (SNAC). Radiographs reveal arthritis sparing the radiolunate joint but involving the midcarpal joint. According to the SNAC staging system, Stage II disease is characterized by degenerative changes specifically involving which of the following joints?
Explanation
Question 48
A 70-year-old woman is 3 years out from a reverse total shoulder arthroplasty. Radiographs demonstrate significant inferior scapular notching. Which of the following technical errors during the index procedure is most strongly associated with this complication?
Explanation
Question 49
During a carpal tunnel release, the surgeon encounters an aberrant transligamentous recurrent motor branch of the median nerve (Lanz variation) and inadvertently injures it. Weakness in which of the following muscles will most likely be observed?
Explanation
Question 50
A 22-year-old man has a symptomatic scaphoid nonunion. MRI demonstrates avascular necrosis (AVN) of the proximal pole, and CT shows structural collapse (humpback deformity). Which of the following is the most appropriate surgical option to achieve union?
Explanation
Question 51
A 34-year-old female hairdresser presents with paresthesias in her medial forearm and hand, worsening when she works with her arms elevated. She is diagnosed with neurogenic thoracic outlet syndrome. Compression of the brachial plexus most commonly occurs at which of the following anatomical locations?
Explanation
Question 52
A 32-year-old laborer is diagnosed with Kienbock's disease. Radiographs reveal sclerosis and early collapse of the lunate, but normal carpal alignment (Stage IIIA). His ulnar variance is negative 2 mm. Which of the following is the most appropriate operative treatment?
Explanation
Question 53
A 40-year-old bodybuilder sustains an acute distal biceps tendon rupture. He elects to undergo surgical repair. A two-incision (modified Boyd-Anderson) approach is chosen over a single anterior incision. The two-incision approach carries a higher historical risk of which of the following complications?
Explanation
Question 54
An 18-year-old football player sustains a high-energy impact to his medial shoulder. He presents to the emergency department in extreme pain, with dysphagia, a sensation of choking, and a clinically absent medial clavicle prominence. What is the most appropriate next step in management?
Explanation
Question 55
A 65-year-old woman sustains a 4-part proximal humerus fracture. Understanding the vascular anatomy is critical for predicting avascular necrosis. According to recent quantitative anatomical studies, which vessel provides the dominant blood supply to the articular segment of the humeral head?
Explanation
Question 56
A 24-year-old baseball pitcher complains of deep shoulder pain during the late cocking phase of throwing. MRI arthrogram reveals a Type II SLAP tear. Which of the following physical examination findings is most specific for identifying a SLAP lesion in this patient?
Explanation
Question 57
A 45-year-old man presents with a claw-hand deformity and profound intrinsic muscle weakness. When asked to pinch a piece of paper between his thumb and index finger, his thumb interphalangeal joint strongly flexes (Froment's sign). This sign represents a compensatory mechanism for weakness in which muscle, and what is its primary innervation?
Explanation
Question 58
A 25-year-old man sustains a closed, displaced distal-third spiral fracture of the humeral shaft (Holstein-Lewis fracture). His neurovascular examination in the emergency department is entirely normal. Following closed reduction and placement of a coaptation splint, he develops a complete, dense wrist drop. What is the most appropriate next step in management?
Explanation
Question 59
A 60-year-old man undergoes subtotal palmar fasciectomy for Dupuytren's contracture. The surgeon carefully identifies the pathologically thickened fascial bands causing a severe proximal interphalangeal (PIP) joint flexion contracture. Which of the following cords is most directly responsible for PIP joint contracture and often displaces the neurovascular bundle centrally?
Explanation
Question 60
A 30-year-old man requires open reduction and internal fixation of a transverse olecranon fracture using tension band wiring. To successfully convert distracting forces at the posterior cortex into compressive forces at the articular surface, the figure-of-eight wire must be placed on which aspect of the olecranon?
Explanation
Question 61
A 28-year-old gymnast presents with chronic dorsal wrist pain and a positive Watson scaphoid shift test. Suspecting a scapholunate ligament tear, the surgeon discusses potential repair. Which anatomical region of the scapholunate interosseous ligament (SLIL) is the thickest and most critical for preventing pathologic diastasis?
Explanation
Question 62
A 29-year-old competitive weightlifter feels a sudden "pop" in his anterior chest while performing a heavy bench press. Examination reveals loss of the anterior axillary fold and weakness with internal rotation. MRI confirms a pectoralis major rupture. What is the most common anatomical location of this tear in this patient population?
Explanation
Question 63
A 36-year-old volleyball player complains of vague posterior shoulder pain and profound weakness in external rotation. MRI reveals a large paralabral cyst located in the spinoglenoid notch. Which of the following muscle denervation patterns is most likely present?
Explanation
Question 64
A 21-year-old skier falls while holding a ski pole, sustaining an acute thumb metacarpophalangeal (MCP) joint ulnar collateral ligament (UCL) tear. Ultrasound reveals a Stener lesion. Which anatomical structure interposes between the torn ends of the UCL, preventing conservative healing?
Explanation
Question 65
A 72-year-old woman presents with severe shoulder pain, poor active elevation, and "pseudoparalysis" of the right arm. Radiographs demonstrate severe glenohumeral osteoarthritis with high-riding of the humeral head. MRI confirms a massive, retracted, and fatty-infiltrated tear of the supraspinatus and infraspinatus. What is the most appropriate definitive surgical management?
Explanation
Question 66
A 35-year-old man presents with a puncture wound on the volar aspect of his index finger. Examination reveals a finger held in slight flexion, fusiform swelling, tenderness along the flexor tendon sheath, and severe pain with passive extension. What is the most appropriate next step in management?
Explanation
Question 67
A 40-year-old woman complains of a "snapping" sensation and apprehension in her elbow when pushing herself up from a chair. She has a history of an elbow dislocation treated nonoperatively 2 years ago. On examination, a pivot-shift test reproduces her symptoms. Which structure is most likely deficient?
Explanation
Question 68
A 25-year-old man falls onto his outstretched hand and presents with severe volar wrist pain and median nerve paresthesias.
A lateral radiograph of the wrist demonstrates the "spilled teacup" sign. What is the most likely diagnosis?

Explanation
Question 69
A 28-year-old weightlifter presents with a dull ache in his right shoulder and noticeable weakness. On examination, performing a wall push-up causes his right scapula to exhibit significant medial winging. Injury to which of the following nerves is the primary cause of this finding?
Explanation
Question 70
When performing a surgical repair of a distal biceps tendon rupture, the choice between a single-incision anterior approach and a two-incision approach affects the complication profile. The single-incision approach carries a significantly higher risk of which of the following complications compared to the two-incision technique?
Explanation
Question 71
A 45-year-old man presents with chronic lateral elbow pain. He reports deep, aching pain in the proximal forearm that worsens with repetitive pronation and supination. Examination reveals maximal tenderness approximately 4 cm distal to the lateral epicondyle and pain elicited by resisted middle finger extension. What is the most likely diagnosis?
Explanation
Question 72
A 22-year-old woman undergoes primary repair of a zone 2 flexor digitorum profundus (FDP) laceration. Postoperatively, she is started on an early active motion protocol. What is the primary benefit of this protocol compared to prolonged immobilization?
Explanation
Question 73
A 55-year-old man sustains a "terrible triad" injury of the elbow after a fall. Surgical management is planned. What is the standard recommended sequence of surgical repair for this specific injury pattern?
Explanation
Question 74
A 20-year-old rugby player felt a pop in his ring finger while grabbing an opponent's jersey. He is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs show a small bony avulsion fragment located at the level of the proximal interphalangeal (PIP) joint. According to the Leddy-Packer classification, what type of injury is this?
Explanation
Question 75
A 55-year-old manual laborer presents with persistent shoulder pain due to a symptomatic Type II SLAP tear that has failed conservative management. Given his age and occupation, which surgical procedure is associated with the most reliable clinical outcome and lowest rate of stiffness?
Explanation
Question 76
A 30-year-old man presents with chronic central dorsal wrist pain. Radiographs demonstrate ulnar minus variance and sclerosis of the lunate without architectural collapse (Lichtman Stage II). Which of the following is the most appropriate joint-leveling procedure for this patient?
Explanation
Question 77
A 35-year-old woman complains of volar forearm pain and numbness in the thumb, index, and long fingers. Which of the following physical examination findings best differentiates Pronator Syndrome from Carpal Tunnel Syndrome?
Explanation
Question 78
A 60-year-old woman with severe basilar thumb arthritis undergoes a ligament reconstruction and tendon interposition (LRTI) procedure. What is the most common radiographic complication associated with this surgery?
Explanation
Question 79
A 19-year-old collegiate pitcher complains of medial elbow pain during the late cocking and early acceleration phases of throwing. A moving valgus stress test is positive. Which specific bundle of the ulnar collateral ligament (UCL) is the primary restraint to valgus stress and is most likely injured?
Explanation
Question 80
A 24-year-old man presents with a scaphoid waist fracture nonunion 9 months after injury. MRI reveals avascular necrosis of the proximal pole. What is the most appropriate surgical graft choice to promote healing in this setting?
Explanation
Question 81
A 24-year-old professional baseball pitcher presents with vague anterior shoulder pain during the late cocking phase of throwing. The O'Brien test is positive, and MRI reveals a Type II SLAP lesion. What is the most appropriate initial management?
Explanation
Question 82
A 42-year-old bodybuilder feels a pop in his anterior elbow while lifting heavy weights. He exhibits weakness in supination and flexion, and the "hook test" is positive. What is the most common complication of a single-incision anterior approach repair for this injury?
Explanation
Question 83
A 45-year-old manual laborer presents with chronic wrist pain. Radiographs demonstrate a scaphoid nonunion with radioscaphoid and capitolunate arthritis, but the radiolunate joint is well preserved. What is the most appropriate surgical treatment?
Explanation
Question 84
A Martin-Gruber anastomosis involves a connection from the median to the ulnar nerve in the forearm. How does this anatomic variant classically affect electromyography/nerve conduction studies (EMG/NCS) of the ulnar-innervated intrinsic hand muscles?
Explanation
Question 85
A 35-year-old carpenter presents with a swollen, painful index finger 2 days after a puncture wound. Examination reveals severe pain with passive extension, flexed resting posture, and tenderness along the flexor sheath. He is taken to the OR, where the flexor tendon appears frankly necrotic. What is the most appropriate intraoperative step?
Explanation
Question 86
A 65-year-old woman is undergoing preoperative CT planning for an anatomic total shoulder arthroplasty. Imaging demonstrates a Walch B2 glenoid with 20 degrees of retroversion. If this excessive retroversion is left uncorrected during the procedure, what is the most likely mode of failure?
Explanation
Question 87
A 40-year-old man sustains a "terrible triad" injury to his elbow following a fall. According to standard biomechanical principles of reconstruction for this specific injury pattern, what is the most widely accepted surgical sequence?
Explanation
Question 88
A 32-year-old mechanic presents with dorsal wrist pain. Radiographs reveal sclerosis and early fragmentation of the lunate, with negative ulnar variance (Lichtman Stage IIIA). The carpal height ratio is maintained. What is the most appropriate surgical intervention?
Explanation
Question 89
A 28-year-old woman is unable to form a perfect "OK" sign with her thumb and index finger 4 weeks after a proximal forearm crush injury. She demonstrates a flat, pad-to-pad pinch. Sensation in her hand is completely normal. Which of the following muscles is most likely affected?
Explanation
Question 90
A 62-year-old woman sustained a nondisplaced distal radius fracture treated nonoperatively in a cast. Two weeks after cast removal, she suddenly loses the ability to actively extend her thumb interphalangeal joint. What is the primary pathophysiology of this specific complication?
Explanation
Question 91
A 72-year-old man is 3 years post-operative from a reverse total shoulder arthroplasty (rTSA) for massive cuff tear arthropathy. Radiographs demonstrate a large radiolucent area at the inferior aspect of the glenoid neck. Which surgical technique during the index procedure most effectively minimizes this complication?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding upper-extremity-2005-set-4-mcqs-3998